SOAP Note - Ashpmedia.org
advertisement

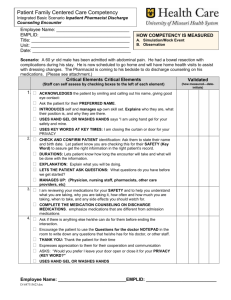
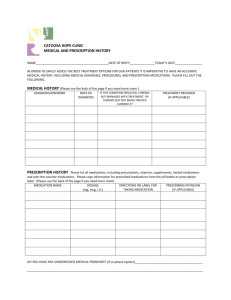
1 SOAP Note Date: XX/XX/XX Time In: 10 AM Pharmacotherapy Note: S: MM is a 51 YO CM who presented for follow-up regarding his diabetes selfmanagement education (DSME) and follow-up A1C testing. MM will begin group support classes at the DERC in January. MM does not have PCP physician at this time since he does not have insurance. He began a new job this month and hopes to have insurance within the next 90 days. Patient does not report any complaints today. PmHx: Type 2 DM (since June 2009) Melanoma on forehead ALL: NKDA CVD risk factors (-) tobacco (+) HTN (+)DM (+)Low HDL (-)FamHx Ht Dz (+)age (M> 45, W>55) = 4 risk factors (1 CVD equivalent) DM (-) polydipsia, polyphagia but has some increased urination last week when starting his new job. Nocturia x 0-2. (-)episode(s) of hypoglycemia since last visit. (+)tingling in wrist and calfs,(-) burning, and numbness of extremities or cramping. Pt reports (-)edema HTN: (+)HA 2 days ago resolved with ibuprofen and rarely occurs (-) dizziness, (-)chest pain. Trying to keep sodium intake <2g/d. Trying to follow dietary recommendations: eating three meals a day. Has already been in DSME part 1 and part 2 classes (carb counting) and is waiting to join a support group. Soc Hx: (-) Tob, (-) EToh, (-) illicit drugs, (+) caffeine (1 cup tea in AM with skim milk and sugar subst), not exercising right now due to left toe amputation in June. New position at different hotel, as an auditor on 11-7PM shift. SurgHx: Left toe amputation SMBG: per patient log (10/10-10/13): (FBG only) (133-144). No readings above 140mg/dl. Podiatry appt: to be scheduled Optometry appt: to be scheduled Immunizations: flu shot needed, refer to health department O: Sex: M HT: 68in BMI: 30 WT: 193 (Previous 197, 202) Race: Caucasian 2 BP 148/56 (no HTN medications taken today) (Prev) 114/76, 112/72mmHg P: 100 PPBG: 122mg/dl (ate cereal at 8:30AM) Prev FBG: 8/17 (184, 1hr PPBG) Date 7-09 K: 4.3 LFT: WNL Scr: 0.73 Lipids: WNL, except low HDL 21mg/dl Date TC 145 TG 135 LDL 97 HDL 21 EsGFR: (7/09) 148ml/min (CG), 120ml/min (MDRD) Microalbuminuria: none checked HbA1C: 5.7% (12.2%) (7/10/09) when hospitalized and diagnosed Outpt medications: (medication reconciliation documented and verified) Metformin 500mg PO BID (taking) Glipizide 5mg PO daily Clonidine 0.1mg PO TID (not taking) Lisinopril 20mg PO BID (not taking) Omeprazole 20mg PO daily (not taking) OTC Recommend ASA 81mg PO daily (has not been taking recently) Herbals None A: DM: Controlled based on SMBG log, hyperglycemia symptom improvement and A1C today. Reviewed meter instruction technique and importance of checking BG twice a day before breakfast and 2-hr after meals. Will need comprehensive annual foot exam and assessment for microalbuminuria, retinopathy assessment, annual influenza, and low dose ASA. (Goal FBG 70-130mg/dl, PPBG<180mg/dL, HbA1C< 6%-7% without causing hypoglycemia) HTN: Uncontrolled based BP today s s in clinic. Patient complained of adverse events associated with clonidine: sleepiness, lethargy, dizziness. He discontinued use without tapering as well as stopping lisinopril as he believed the side effects were related to both agents. Will reinitiate lisinopril at low dose (10mg) and re-evaluate for titration when RTC in 2 weeks. (Goal < 130/80 DM) Lipids: Controlled based on recent lipid panel with the exception of his HDL. Reinforced importance of physical activity as tolerated with his amputation and contingent on physician approval. Alternatives are swimming, stationary bike as well as reinforcing principles of the DASH diet and TLC to help improve HDL. (Goal TC<200mg/dl,TG <150mg/dl, HDL>40mg/dl, LDL<100, optional goal <70mg/dl) P: 1. Discussed the importance of checking blood glucose at least BID and provided log to report values. Provided medication instruction sheet and log for exercise. 3 2. Discussed the s/sx of hypo/hyperglycemia and what to do should they occur. Confirmed technique for meter instruction and will reassess in 3 months (December). 3. Reviewed all medications (provided med list) with patient and discussed reinitiation of lisinopril. Continue current dose of metformin 500mg PO BID with meals, ASA 81mg PO daily, Glipizide 5mg PO daily before breakfast, lisinopril 20mg 1/2T PO daily. Discussed common side effects to watch for with his regimen. 4. Call with any problems. Encouraged to continue a low-fat, low cholesterol, moderate CHO diet (130-150grms daily). 5. Expected level of patient adherence is: good. 6. Refer to NP today for comprehensive foot exam and health department for flu shot. 7. Will notify Dr. X (physician name here) of the pending blood work and assessment today. 8. Will need f/u lipid assessment in November along with microalbuminuria assessment, A1C in three months and should be screened for colorectal cancer. Follow-up standards of care 1. Podiatry q 6 months 2. Dentistry q 6 months 3. Optometry q 6 months 4. Nutrition prn Signature Seena Haines, PharmD, BC-ADM, CDE Pharmacotherapy Specialist Diabetes Education and Research Center Time Out: 60 minutes spent counseling/coordinating care Total Time Spent: 1 HR By using a standardized format, such as a SOAP note, other practitioners can get an understanding of the interaction with the patient as well as your assessment and plan to manage disease states that have been referred. Within the SOAP note example provided, pay attention to the key elements that pertain to pharmaceutical care such as past medical history (PMH), review of systems (ROS), and the medication reconciliation. Do all 4 medications have an indication for this patient? Screening for duplicate therapy or omissions is also important. Every medication should be accounted for within the PMH. Within this SOAP, also note the objective section, which allows you to formulate your assessment and then plan the two most important sections for communicating the care given to this patient. The assessment should be as complete as soon as possible so referring provider can know how the visit(s) has progressed as well as the care. The plan should be succinct and outline exactly what the goal is for the therapy used. Note the assessment and plan can be done together in the same paragraph or it can be separated. No matter which format used, always make sure to account for management issues that cannot be handled by the pharmacists. Notice that the end of the note contains a plan to ensure the patient referred to other care providers to handle preventive care that does not fall into the realm of the pharmacists’ scope. Even though it was not handled directly by the pharmacist, it is important to show that care is universal and that the pharmacist understands the entire scope of the patient’s problems. Basic 7 Lines of Questioning32,33 Location Quality Quantity Timing Setting Modifying factors Associated symptoms Where is the symptom(s)? What is it like? How severe it is? How long have symptoms been present? How did it happen or what was the patient doing? What makes it better or worse? What other occurrences have taken place of importance? A 21-year-old male (JL) approaches you, the pharmacist, and asks, "What can I take for my headache?" You ask the patient about his symptoms and he comments about studying for his final exams all week. “I felt like my head is going to explode this morning.” He goes on to describe the pain being dull now versus hours earlier. Pain index is 4/10. He has not taken any over-the-counter medicines, but he did try resting and lying down for several minutes; it did help some but all the studying and reading made it worse. You ask JL to describe where the pain is in his head and if it has spread anywhere. JL points to his head and also neck and shoulder area. Past medical history is significant for ulcers, and he has no known drug allergies (NKDA). Current medication: Omeprazole 20mg PO daily and multivitamin PO daily. The QuEST Method: SCHOLAR-MAC Symptoms Characteristics History Original pain was head exploding Dull consistent pain 4/10 Tried resting before presenting today 5 Onset Location Aggravating factors Remitting factors Medications ALL Comorbidities Early this morning Head and radiates to neck and shoulders Reading and studying Resting, lying down Prilosec NKDA PUD