New Patient Questionnaire
advertisement

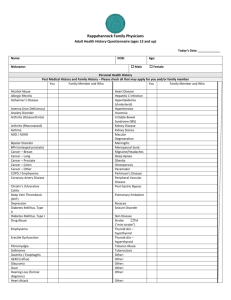
Rush University Internal Medicine Patient Questionnaire—New Patient This questionnaire will help us collect important information about your medical history. Once this information is entered into our electronic medical record, this document will be shredded. Name: __________________________________DOB:__________ Date: ________ What issues would you like to discuss with the doctor today? Other than the concerns mentioned above, list your ongoing medical problems? When did you last see a doctor? What reason? When was your last complete physical exam? Have you ever undergone SURGERY? If yes, please list surgery and year. □ Yes □ No Have you ever been HOSPITALIZED other than for surgery? If yes, please list. □ Yes □ No Are you taking any prescription medications? If yes, please list. _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ Do you have any ALLERGIES to medications? If yes, please list. □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No Do you take any over-the-counter medications, herbal medicines, vitamins, or nutritional supplements? If yes, please list. Do you see any other doctors? If yes, please list and give the condition for which they treat you. Health Habits Do you smoke cigarettes or cigars? If yes: How many do you smoke in a typical day? For how many years have you smoked? If you do not currently smoke, did you ever smoke? If yes: When did you quit? How many did you smoke in a typical day? For how many years did you smoke? □ Yes □ No _____________ _____________ □ Yes □ No _____________ _____________ _____________ Name: ___________________________________DOB:_________ Date: _________ How many alcoholic beverages do you drink in a typical day? About your consumption of alcohol: Ever been concerned about the amount consumed? Ever intentionally cut back the amount consumed? Do you ever drink more than 5 drinks in a day? _____________ □ Yes □ Yes □ Yes □ No □ No □ No Do you use any illicit (street) drugs? Have you ever used intravenous drugs? □ Yes □ Yes □ No □ No Do you exercise? If yes, please describe type and frequency of exercise. □ Yes □ No Nightly, how many hours do you typically sleep? How would you describe your sleep? Do you have problems: Falling asleep? Staying asleep? Awakening early? Do you awaken feeling refreshed? Do you have problems staying awake during the day? _____________ □ Restful □ Not restful □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No Vaccination History In what year was your last tetanus booster? ________ Did this tetanus booster include the pertussis (whooping cough) vaccine? ________ Were you immunized for the current influenza season? □ Yes □ No If yes, when was it given? ________ Were you ever given the pneumococcal (“pneumonia”) vaccine? □ Yes □ No If yes, when was it last given? ________ Have you ever had chickenpox? □ Yes □ No Were you ever given the chickenpox vaccination? □ Yes □ No If yes, when was it last given? ________ Were you ever given the Hepatitis B vaccination? □ Yes □ No If yes, when was it given? ________ If over age 60, were you given the Zoster (Shingles) vaccine? □ Yes □ No Were you ever given the HPV vaccine? □ Yes □ No Do you know if you are immune to rubella? □ Yes □ No In the past 10 years, were you given any other vaccinations? □ Yes □ No If yes, please list: Personal History Where was your birthplace? ________________________________________________________ Where were you raised? ___________________________________________________________ What was the highest level of education you finished? __________________________________ Were you ever in the armed forces? □ Yes □ No What is your occupation? __________________________________________________________ Weekly, how many hours do you typically work? _______________________________________ Are you retired from working? □ Yes □ No If yes, what work did you retire from? __________________________________________ If yes, at what age did you retire? ______________________________________________ How do you like to spend your free time? _____________________________________________ 2 Name: ___________________________________DOB:__________ Date: ________ List the people living with you. Are there any problems at home which disturb you? Have you had any recent major life events or changes? □ Yes □ Yes □ No □ No Family medical history Relative Age (or circle age at death) Medical conditions Natural mother Natural father Maternal: Grandmother Grandfather Paternal: grandmother grandfather Sisters: Brothers: Children: Reproductive/Sexual History (women only) Do you menstruate? □ Yes □ No If yes: At what age did your menses start? ____________ How long is your menstrual cycle? ____________ What is the duration of your menstrual period? ____________ Describe your menstrual flow. ________________________________________________ Do you have any distressing symptoms during your periods? □ Yes □ No If yes, describe. __________________________________________________________ If no: At what age did your menses start? ____________ At what age did your menses cease? ____________ Are you taking hormone replacement therapy? □ Yes □ No If yes, for how many years? ____________ If no, did you ever take it? □ Yes □ No 3 Name: ___________________________________DOB:_________ Date: _________ Are you sexually active? If yes, with men, women, or both? If you are sexually active with men, do you use contraception? If yes, what type? Does your partner use any form of contraception? Do you and your partner practice “safe” sex? Have you had any pregnancies? If yes: How many pregnancies Were there any complications? Have you had any miscarriages? Have you undergone any abortions? Have you ever had any sexually transmitted diseases? Do you experience any difficulty enjoying sex? □ Yes □ No □ Men □ Women □ Both □ Yes □ No _________________ □ Yes □ No □ Yes □ No □ Yes □ No ___________ □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No Reproductive/Sexual History (men only) Are you sexually active? If yes: With women, men, or both? Do you use condoms? Does your partner use contraception? Do you and your partner practice “safe” sex? Have you ever had any sexually transmitted diseases? Do you experience any difficulty enjoying sex? Have you fathered children? □ Yes □ No □ Women □ Men □ Both □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No Screening History (women) When was your last Pap smear? Ever had a Pap smear which showed dysplasia (pre-cancer)? Did you ever test positive for HPV? If you are over age of 40 years, when was your last mammogram? Have you ever had an abnormal mammogram? If yes, please explain. Do you perform breast self-examinations monthly? If you have gone through menopause, have you ever had a bone density test? If yes, was it normal? ____________ □ Yes □ No □ Yes □ No ____________ □ Yes □ No □ Yes □ Yes □ Yes □ No □ No □ No Screening History (men) If you are over age 50 years, or over age 40 years with a family history off prostate cancer, have you ever been counseled about prostate cancer screening? When was your most recent prostate exam? ____________ When was your most recent PSA blood test? ____________ Screening History (men and women) When was your last eye exam? Was it normal? ____________ □ Yes □ No 4 Name: ___________________________________DOB:_________ Date: _________ When was your last cholesterol level? ____________ Was it normal? □ Yes □ No If you are over age 50 years, or over age 40 years with a family history of colon cancer: Have you had a colonoscopy? □ Yes □ No If yes, when was the last exam? ____________ Do you examine your skin regularly looking for skin cancer? □ Yes □ No When was your last dental exam? ____________ Review of Systems: Currently, do any of these apply to you? If yes, check box. Review of Systems: Currently, do any of these apply to you? If yes, check box. □ feel at risk for falling Pain (if present, specify where the pain is) □ experienced daily: ____________________ □ experienced infrequently: ______________ Constitutional □ weight loss greater than 10 pounds □ weight gain greater than 10 pounds □ fatigue without effort □ loss of appetite □ persistent fever Head □ headaches □ facial pain Eyes □ failing vision not correctable □ sudden loss, dimming, blurring □ eye pain □ eye redness □ double vision Ears □ difficulty hearing □ recurrent ear infections □ ear injuries □ persistent ringing/buzzing Nose □ inability to smell □ frequent nosebleeds □ persistent congestion/drainage □ difficulty breathing through the nose Mouth □ sores that do not heal □ tooth loss □ change in taste Throat □ frequent sore throats with fever □ hoarse voice without a cold Neck □ lumps or swelling in your neck Breast □ lump in the breast (or under the nipple) □ discharge from or pain in the nipple Cardiovascular □ chest discomfort, pressure, tightness, pain □ shortness of breath with exertion □ awakening at night short of breath □ palpitations (hard or racing heart beat) □ heart murmur □ pain or cramping in legs when walking □ swollen legs Respiratory □ shortness of breath with exertion □ persistent cough □ chronic sputum production □ coughing up blood □ abnormal chest x-ray □ wheezing at rest, with exertion, or at night □ pain in chest with breathing Gastrointestinal □ difficulty swallowing □ frequent or severe heartburn □ frequent or severe abdominal pain □ frequent or new nausea or vomiting □ vomiting blood or black material □ long-standing constipation □ recent-onset constipation □ frequent, loose, or watery stools □ recent change in character of stools □ black or bloody stools □ bleeding from the rectum □ rectal pain Genitourinary □ frequent urination □ burning urination □ urinary infections □ losing control of urine □ bloody, black, or brown urine 5 □ kidney stones □ loss of balance while walking □ numbness or tingling in arms or legs □ loss of control of bowels or bladder □ repeated muscle spasms/cramps □ inability to sleep adequately at night □ chronic sleepiness, fatigue, tiredness women only: □ persistent or severe vaginal discharge □ no menses for more than 6 months unrelated to pregnancy or menopause □ bleeding between menstrual periods □ heavier or more prolonged menses □ bleeding after intercourse □ distressing symptoms related to menses □ losing interest in sex □ hair growth on face, chest, abdomen Psychiatric □ treated for any psychiatric illness □ depressed moods □ diminished interest/pleasure in activities □ difficulty sleeping or sleeping too much □ fatigue/loss of energy □ decreased ability to concentrate □ decreased ability to make decisions □ nervousness, anxiety, irritability □ intense fear or discomfort Endocrine □ elevated blood sugar □ elevated cholesterol □ bone fractures not caused by trauma □ a tendency to always feel hot □ a tendency to always feel cold □ increased thirst all the time □ increased appetite Hematologic □ anemia □ easy bruising □ persistent bleeding from cuts/scratches □ gums that bleed easily if tooth brushing Allergic □ sneezing, chronic runny nose, itchy nose, watery eyes □ persistent coughing not associated with a cold □ cough associated with exercise or exertion □ allergies (dust, mold, ragweed, cats, etc.) men only: □ weak or slow urinary stream □ prostate problem □ burning or discharge from penis □ swelling or lumps in the testicles □ pain in the testicles □ losing interest in sex □ unable to attain or sustain erections □ development of abnormal breast tissue Musculoskeletal □ aching muscles □ lasting or repeated back pain □ lasting or repeated neck pain □ painful, swollen, or stiff joints □ painful feet Skin □ persistent skin problem □ skin rash □ dark moles □ change in skin pigmentation □ unusual hair loss □ skin lesion that bleeds or does not heal Neurologic □ dizziness (spinning) □ loss of consciousness □ seizures □ weakness in an arm or leg If you are ever unconscious following surgery, in an emergency room, or in a hospital, with whom do you authorize us to discuss your case? Does this person have the authority to make decisions for you? Have you completed a Durable Power of Attorney for Health Care? Have you completed a Living Will? Signed: ______________________________________ 6 Date: _______ 7