CRCMedCxForm-DOH348-082-Jan2016
advertisement

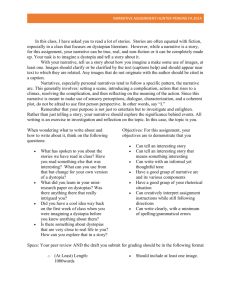
SPOKANE REGIONAL HEALTH DISTRICT PHONE 509-323-2851 FAX 509-324-1408 WWW.SRHD.ORG DOH 348-082 Jan 2016 MEDICAL COMPLICATIONS REPORTING FORM COLORECTAL CANCER SCREENING AND DIAGNOSIS Initial Reporting Date: Click here to enter a date. Follow-Up Date: Click here to enter a date. Follow-Up Date: Click here to enter a date. Follow-Up Date: Click here to enter a date. Number Criteria 1 2 3 4 5 6 7 CCDE Med-IT ID Number: Click here to enter text. Region: Choose an item. Response Procedure related to medical complication Choose an item. Indication for Examination Choose an item. Results of Examination: Choose an item. Bowel Preparation Adequate Choose an item. Segment reached (if sigmoidoscopy or colonoscopy Choose an item. Difficult Examination Choose an item. Biopsy/polypectomy performed Choose an item. Procedure(s)/Technique(s) performed Check all that apply: done) Submucosal injection Snare polypectomy Hot biopsy forceps or cautery 8 Cold biopsy Ablation Medical Complication(s) Control of bleeding Unknown Other Click here to enter text. Check all that apply: Emergency Room visit Bleeding Cardiopulmonary events Complications related to anesthesia 9 Perforation Other Click here to enter text. Death Cause of Death: Click here to enter text. Excessive abdominal pain For persons with disabilities, this document is available on request in other formats. To submit a request, please call 1-800-525-0127 (TDD/TTY 711). DOH 348-082 Jan 2016 SPOKANE REGIONAL HEALTH DISTRICT PHONE 509-323-2851 FAX 509-324-1408 WWW.SRHD.ORG Number Criteria Client Medications 10 Response Check all that apply: Aspirin Number Inhaled corticosteroids H2 Blockers Oral corticosteroids NSAIDS Proton pump inhibitor Anticoagulants None Other Hospital Admission Required 11 Current Status of Client Click here to enter text. Choose an item. Hospital Admission Date: Click here to enter a date. Hospital Discharge Date: Click here to enter a date. Initial Status Narrative: Click here to enter text. Follow-Up Narrative: Click here to enter text. 12 Follow-Up Narrative: Click here to enter text. Interventions Performed to address complications with pertinent dates 13 Follow-Up Narrative: Click here to enter text. Initial Narrative: Click here to enter text. Follow-Up Narrative: Click here to enter text. Follow-Up Narrative: Click here to enter text. Follow-Up Narrative: Click here to enter text. Instructions: Complete the form for medical complications resulting from screening or diagnostic purposes occurring during or within 30 days. Medical Complications Requiring Hospitalization: Prime Contractors (PCs) should notify the Washington State Breast, Cervical and Colon Health Program (BCCHP) Public Health Nurse Consultant (PHNC) within 24 hours of the notification of the hospitalization The PHNC will notify the Centers for Disease Control and Prevention (CDC) technical assistance team by email within 36 hours of notification The PC will submit the form to the BCCHP PHNC within 2 days of notification of the hospitalization The PHNC will submit the form to the CDC within 3 days of notification of the hospitalization The form will be updated by the PC and the PHNC monthly or more frequently as the client’s status changes to CDC until resolved. Updates require response to only require Questions #12 and #13 of the form. Complete fields of the CCDE record in Med-IT on this client and submit when due Medical Complications NOT Requiring Hospitalization: PCs should notify the Washington State BCCHP PHNC within 15 days of the notification of the complication The BCCHP PHNC will notify the CDC quarterly on September 1 st, December 1st, March 1st and June 1st The PC will submit the form to the BCCHP PHNC within 30 days of notification The form will be updated by the PC and PHNC quarterly and submitted to CDC if the medical complication was not resolved within the quarter period until resolution – Updates require response to Follow-up date, #12 and #13 of the form. Complete fields of the CCDE record in Med-IT on this client and submit when due For persons with disabilities, this document is available on request in other formats. To submit a request, please call 1-800-525-0127 (TDD/TTY 711).