(Q6): Is laparoscopic liver resection applicable to donor hepatectomy?
advertisement
: Is laparoscopic liver resection applicable to donor hepatectomy?")
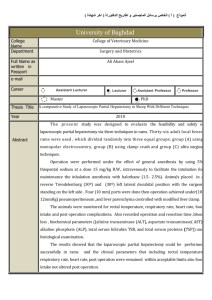
Q6 Recommendation The 2nd International Consensus Conference on Laparoscopic Liver Resection Question 6 (Q6): IS LAPAROSCOPIC LIVER RESECTION APPLICABLE TO DONOR HEPATECTOMY? Q 6 Working group Coordinator Roberto I. Troisi Literature Review Takeshi Takahara Working group Ki Hun Kim Olivier Scatton Go Wakabayashi Methods: This document is based on a comprehensive review of the literature as of August 18th 2014. To date, neither systematic reviews nor meta-analysis have been published on that matter. The MEDLINE, Embase, PubMed and Cochrane databases were searched. The following keywords were used: laparoscopic liver resection, laparoscopic donor hepatectomy, hybrid donor hepatectomy, fully laparoscopic living donor hepatectomy, single incision living donor hepatectomy, hand-assisted living donor hepatectomy, laparoscopic left lateral sectionectomy for living donor hepatectomy. The literature search shows that 26 publications were found on that subject after withdrawal of few previous preliminary experiences from the same center. Most of the publications are single-center experience; there are only 9 comparative studies (one prospective), case-control studies and some case reports. Therefore, the level of evidence is classified as “LEVEL III”. The transplants performed with minimally invasive technique are both in pediatric (initial reports) and adult recipient population. But, what stands out most from the analysis is the type of technique used. In fact, in addition to those previously defined in Louisville, minimally invasive (MI) techniques are divided in: hybrid/hand-assisted, laparoscopic assisted including single-port incision and pure laparoscopic. Both groups of techniques are divided for intraoperative and postoperative data. Two additional tables concerning comparative analysis are attached. The publication year range from 2006 to 2014, with a peak between 2012 and 2014. From the summarized tables (attached pdf file, tables 1 to 6) concerning the available data on case series of minimally invasive living donor hepatectomy, we can observe that: - In the HALS-Hybrid procedures most of the grafts were right lobes (n=147, vs.13 Left lobes-LH). The blood loss (BL) range from 212 to 520 ml (1 extra U transfusion) with and operative time (OT) of 265 -702 min. No conversions were reported (Table 1). Postoperative data shows an hospital stay (HS) from 4.3-12 d, 0% mortality, complication rates between 0-25% and a reoperation rate ranging from 0-6.7% (Table 2). - In the lap assisted/single incision groups, again more right lobes (n=88, vs. 37 LH and 18 LLS). The blood loss (BL) range from 200 to 870 ml (Transfusion 01.25 U). The OT is ranging from 278-435 min and the conversion rate is 0-10% (Table 3). The HS is 8-12 d, reoperation rate 0-5%, complications from 7.7-30% and no mortality reported (Table 4). - Looking to the pure (fully laparoscopic) procedures, we notice that the great majority of grafts are LLS (n=110, vs. 12LH and 4RH). The BL is ranging from 18-410ml and no transfusions have been done. The OT is 275-605 ml and conversion rate of 0-13.3% (Table 5). The HS is ranging from 4-10.8 days, the reoperation rates from 0-25%, the complications rate from 0-33% and, again, no mortality has been reported (Table 6). Nine comparative series between open and minimally invasive (MI) procedures (a mix of HA, hybrid and pure laparoscopic) are available at that moment, 2 out of 9 focusing on pure LLS for pediatric LDLT. Most of the grafts retrieved were right lobes (essentially performed with the HA and/or hybrid procedures), and precisely: 129 RH, 31 LH and 51 LLS. From the 7 comparative series (table 7) including RH, LH and LLS using HA, lap assist and single-port incision, several end-points have been addressed as per below: 1- Morbidity: this was ranging from 0-28% (open) vs. 0-21.3% (MI); 2- Mortality: no mortality has been reported so far in that series; 3- Operation time: this was ranging from 303-383 min (open) vs. 265-435 min (MI). In 4/7 center series MI procedures taken a longer time; in three experiences a statistical significance was reached; 4- Blood loss: this was ranging from 250-733 ml (open) vs. 290-1033 ml (MI). In 4/7 of the comparative series, blood loss was less for MI procedures (in one experience, a statistical significance was reached); 5- Blood transfusions: only one series described differences in BT (0.5 U for open vs. 0.25 U for MI). In three other, no additional BT were required; 6- Regarding the management of postoperative pain, 4 out of 5 studies shows a less analgesics use in MI procedures (stat sign); two studies showed less need of additional analgesia (stat signif). Analgesia for pain: 5/7 series reported data. Need for epidural/analgesics ranging from 3.2-4.4 days in open vs. 2.4 vs. 3.2 in MI in three studies. Another showed a difference in hrs. between open and MI (56h vs. 47h respectively). A fifth group reported no differences. Time for extra analgesia was described in two studies showing a shorter treatment in MI (3.8 vs. 1.2 days respectively for open vs. MI), no differences in the second (2.4 and 2.5 days respectively for open and MI). 7- Hospital stay: this was ranging from 3.9 -18.3 days in open vs. 4.3 -11.8 days in MI; 8- Costs: this issue was assessed in 3 studies, all showing slightly increased costs with the MI procedures. Two comparative series are available between pure laparoscopic LLS and standard procedures for pediatric LDLT (Table 8). In one the morbidity is higher in open procedures (stat not signif) and the OT time is longer in pure laparoscopic procedures; BL is significantly less in the first study, almost comparable in the second study. Postoperative pain is comparable, HS shorter in one study in case of laparoscopic approach whereas the costs are slightly increased in case of open procedures (probably reflecting a longer hospital stay) in the other study. Experts recommendations on Q6 Preamble: - Different techniques for minimally invasive living donor hepatectomy have been used; - Pure laparoscopic technique especially in LLS for pediatric LDLT, increasing procedure for LH grafts in A2ALDLT; - All available data are case series, case–control studies, comparative studies (only one prospective) Conclusions: 1. An exponential increase of number of procedures and center experiences has been observed since 2012 2. Despite the use of different MI techniques, no mortality has been reported with a comparable or lower morbidity respect to the standard approach 3. Presently, there is a trend in favor of pure laparoscopic approach for LLS for pediatric LDLT which could be considered as a safe procedure with potential advantages brought by the laparoscopic technique 4. Pure right donor hepatectomy still under evaluation (pending issues: higher morbidity linked to the graft volume retrieved or less stress and pain due to the MI technique) 5. Comparative studies suggests that MI living donor hepatectomy is feasible with possibly less morbidity in teams that are familiar with both open living donor and laparoscopic liver resections REFERENCES 1. Scatton O, Katsanos G, Boillot O, et al. Pure Laparoscopic Left Lateral Sectionectomy in Living Donors: From Innovation to Development in France. Ann Surg 2014. 2. Ha TY, Hwang S, Ahn CS, et al. Role of hand-assisted laparoscopic surgery in living- donor right liver harvest. Transplant Proc 2013; 45(8):2997-9. 3. Troisi RI, Wojcicki M, Tomassini F, et al. Pure laparoscopic full-left living donor hepatectomy for calculated small-for-size LDLT in adults: proof of concept. Am J Transplant 2013; 13(9):2472-8. 4. Nagai S, Brown L, Yoshida A, et al. Mini-incision right hepatic lobectomy with or without laparoscopic assistance for living donor hepatectomy. Liver Transpl 2012; 18(10):1188-97. 5. Marubashi S, Wada H, Kawamoto K, et al. Laparoscopy-assisted hybrid left-side donor hepatectomy. World J Surg 2013; 37(9):2202-10. 6. Choi HJ, You YK, Na GH, et al. Single-port laparoscopy-assisted donor right hepatectomy in living donor liver transplantation: sensible approach or unnecessary hindrance? Transplant Proc 2012; 44(2):347-52. 7. Soyama A, Takatsuki M, Hidaka M, et al. Standardized less invasive living donor hemihepatectomy using the hybrid method through a short upper midline incision. Transplant Proc 2012; 44(2):353-5. 8. Kurosaki I, Yamamoto S, Kitami C, et al. Video-assisted living donor hemihepatectomy through a 12-cm incision for adult-to-adult liver transplantation. Surgery 2006; 139(5):695-703. 9. Soubrane O, Perdigao Cotta F, Scatton O. Pure laparoscopic right hepatectomy in a living donor. Am J Transplant 2013; 13(9):2467-71. 10. Oya H, Sato Y, Yamamoto S, et al. A new technique of lateral approach for laparoscopy-assisted donor left hepatectomy. Hepatogastroenterology 2011; 58(110-111):1765-8. 11. Suh KS, Yi NJ, Kim T, et al. Laparoscopy-assisted donor right hepatectomy using a hand port system preserving the middle hepatic vein branches. World J Surg 2009; 33(3):526-33. 12. Soubrane O, Cherqui D, Scatton O, et al. Laparoscopic left lateral sectionectomy in living donors: safety and reproducibility of the technique in a single center. Ann Surg 2006; 244(5):815-20. 13. Troisi R, Debruyne R, Rogiers X. Laparoscopic living donor hepatectomy for pediatric liver transplantation. Acta Chir Belg 2009; 109(4):559-62. 14. Samstein B, Cherqui D, Rotellar F, et al. Totally laparoscopic full left hepatectomy for living donor liver transplantation in adolescents and adults. Am J Transplant 2013; 13(9):2462-6. 15. Rotellar F, Pardo F, Benito A, et al. Totally laparoscopic right-lobe hepatectomy for adult living donor liver transplantation: useful strategies to enhance safety. Am J Transplant 2013; 13(12):3269-73. 16. Yu YD, Kim KH, Jung DH, et al. Laparoscopic live donor left lateral sectionectomy is safe and feasible for pediatric living donor liver transplantation. Hepatogastroenterology 2012; 59(120):2445-9. 17. Kim KH, Jung DH, Park KM, et al. Comparison of open and laparoscopic live donor left lateral sectionectomy. Br J Surg 2011; 98(9):1302-8. 18. Suh KS, Yi NJ, Kim J, et al. Laparoscopic hepatectomy for a modified right graft in adult-to-adult living donor liver transplantation. Transplant Proc 2008; 40(10):352931. 19. Baker TB, Jay CL, Ladner DP, et al. Laparoscopy-assisted and open living donor right hepatectomy: a comparative study of outcomes. Surgery 2009; 146(4):817-23; discussion 823-5. 20. Makki K, Chorasiya VK, Sood G, et al. Laparoscopic assisted versus conventional (open) donor hepatectomy for live donors: When you know better, you do better. Liver Transpl 2014. 21. Lee KW, Kim SH, Han SS, et al. Use of an upper midline incision for living donor partial hepatectomy: a series of 143 consecutive cases. Liver Transpl 2011; 17(8):969-75. 22. Kasahara M, Sakamoto S, Shigeta T, et al. A 7-cm upper midline incision for living donor left lateral hepatectomy: singe-center consecutive 70 donor experience. Transplantation 2012; 93(8): e33-4. 23. Han HS, Cho JY, Yoon YS, et al. Total laparoscopic living donor right hepatectomy. Surg Endosc 2014. 24. Zhang X, Yang J, Yan L, et al. Comparison of laparoscopy-assisted and open donor right hepatectomy: a prospective case-matched study from china. J Gastrointest Surg 2014; 18(4):744-50. 25. Takahara T, Wakabayashi G, Hasegawa Y, Nitta H. Minimally Invasive Donor Hepatectomy: Evolution From Hybrid to Pure Laparoscopic Techniques. Ann Surg 2014 (in press). 26. Thenappan A, Jha RC, Fishbein T et Al. Minimal access live donor hepatectomy for transplantation. Am J Surg 2011, 201 450-455. Q6: Laparoscopic donor hepatectomy Table 1. Hybrid (Living Donor) ~ Intra-operative data~ Table 2. Hybrid (Living Donor) ~ post-operative data~ Table 3. Pure (Living Donor) ~ Intra-operative data~ Table 4. Pure (Living Donor) ~ Post-operative data~