Research Report Sample.

An Investigation in Surgical Cases and Socioeconomic Status
Connor Zale, Thomas J. VanderMeer M.D. and Laura Fitzgerald
Department of Research at Robert Packer Hospital
Guthrie Healthcare
1 Guthrie Square, Sayre, PA 18840
Abstract
This project was designed to analyze if there is a disparity in access to surgical care due to socioeconomic status for patients in the Twin Tiers region. Elective and emergent cholecystectomies were used as indicators for access to surgical care. Socioeconomic status was determined by insurance status, education, and income. Healthcare Association of New York
(HANYS) was accessed in order to obtain patient records that have undergone a cholecystectomy between January 2007 and June 2014.
The report collected 15,767 patient records and elective cases (11,165, 70.8%) outnumbered emergent cases (4,601, 29.2%). Laparoscopic cases (15,299, 97.04%) were the preferred procedure compared to open procedures (467, 2.96%). Cholecystectomy rates per capita by zip code were modeled with socioeconomic census data and trend was analyzed using non-parametric regression.
A higher elective cholecystectomies rate per capita was found to occur in middle income households and also in communities with a 15-18 percent in poverty. Elective cholecystectomy rate per capita was found to decrease dramatically when the percent of the community with a high school degree was greater than 90 percent. The rate of emergent cholecystectomies per capita was uniform across all socioeconomic indicators. Future research will investigate what community resources may be available to account for the variable rate of elective cholecystectomies. The role of urban and rural setting will also be investigated in the future to determine the effect on cholecystectomy case type.
Introduction
Diseases of the gallbladder are the most commonly treated of all the digestive system diseases. The two primary types of gallbladder disease are gallstones, cholelithiasis, and gallbladder cancer
1
. Gallstones affect large portion of Americans and treatment of gallstones has become a substantial portion of the national healthcare cost. It has been estimated that over 20 million Americans suffer from gallstones. Gallbladder disease has been approximated to consume 6.2 billion dollars annually and it has increased over 20% over the last 3 decades 2 .
Due to the enormous amount spent on cholecystectomies each year, this surgical procedure was selected to model patients’ access to care. It was hypothesized that patients with higher socioeconomic status will undergo the procedure electively and patients from a lower socioeconomic status will delay the procedure. This may cause a higher proportion of emergent cholecystectomies for patients of lower socioeconomic status.
The gall bladder is a small organ that lies underneath the liver and it is connected to the duodenum by the common bile duct. The role of the gallbladder is to store bile which is produced by the liver and the bile is stored until it is released into the duodenum in order to digest fats. Bile is composed of bile salts, bilirubin and cholesterol. Gallstones can be composed of hardened cholesterol or complexes of calcium salts, bilirubin, copper, cholesterol and protein 3 .
There are several risk factors for an increased incidence of gallstones. The primary risk factors are age, gender, number of pregnancies, BMI, oral contraceptives, estrogen therapy, family history and genetics. It has been noted that increased age results in an increased risk for gallstones and cholecystitis. Females are 2.4 times more likely to have gallbladder issues than men due to hormones, estrogen and progesterone. Obesity has also been determined to be a risk factor for gallstone formation
8
.
The presence of gallstones may not cause symptoms until complications arise such as, inflammation, infection and obstruction of the common bile duct. Patients that experience symptoms from gallstones commonly state the presence of biliary colic which is a visceral pain that is believed to be caused by the obstruction of the cystic duct. Patients can be treated for gallstones with surgical and non-surgical interventions. An oral dose of bile acids can assist in the treatment of gallstones by medical dissolution therapy. The common surgical treatments are open or laparoscopic cholecystectomy and open or laparoscopic cholecystostomy. A cholecystectomy is the complete removal of a gallbladder and primarily is completed as laparoscopic procedure. A cholecystostomy is the process of forming an opening in the gallbladder and a tube is placed inside the gallbladder for drainage. A cholecystostomy is usually performed when there are preexisting issues that to do not make a cholecystectomy possible 4 .
The Society of American Gastrointestinal and Endoscopic Surgeons provide guidelines for laparoscopic operations on the gallbladder and biliary tree, which allow procedures for symptomatic cholelithiasis, biliary dyskinesia, acute cholecystitis and complications related to the common bile duct stones
5
. A cholecystectomy can be determined to be elective in most cases when the complications of gallstones due not pose an immediate threat to the patient. A cholecystectomy can be advised to the patient when biliary colic is negatively affecting the patient and the patient does not have any major issues in order to undergo surgery
6
. Other indications for a prophylactic cholecystectomy include calculi greater than 3 cm in diameter for individuals from regions with a higher prevalence of gallbladder cancer, a chronically obliterated cystic duct, a nonfunctioning gallbladder, a calcified gallbladder, a gallbladder polyp larger than
10 mm and growing in size, gallbladder trauma or an anomalous junction of the pancreatic and biliary ducts 7 .
Methods
Electronic Medical Records were accessed using Healthcare Association of New York
State database (HANYS). Records were collected for patients that underwent an open or laparoscopic cholecystectomy between January 2007 and June 2014. Age, Gender, Zip Code,
Insurance Status, Procedure and Case type (elective or emergent) was obtained for analysis.
Emergent cholecystectomies were identified by an emergency room code that was attached to the case type within the report. Pregnant women and children were excluded from this study.
Patient zip code was paired to U.S. Census data for median income, percentage of the population in poverty and percentage of population with at least a high school level degree.
T-tests were performed for age by case type for each gender separately. Insurance status for emergent cases was compared to institutional data for all patients at Robert Packer Hospital and Corning Hospital. Scatter plots were constructed using cholecystectomy rates and socioeconomic indicators to determine if there was a trend. The trend for each graph was created using local polynomial regression fitting (LOESS). Statistical tests were conducted using R software. Figures were created with R software and Microsoft Excel.
This project was reviewed and approved by Guthrie Institutional Review Board prior to data collection. This project was determined to be a minimal risk study because the only patient identifier, B number, was removed prior to statistical analysis. A waiver for patient consent was obtained for this study since it was a retrospective chart review by design.
Results
The HANYS report collected 15,767 total cholecystectomy cases for patients that reside within Guthrie’s primary and secondary service area (Figure 1). There were 11,165 elective cases (70.8%) and 4,601 emergent cases (29.2%) (Figure 2). One case was identified as unknown case type and this was excluded from case type analysis. The elective cases included
11,045 laparoscopic procedures and 120 open procedures. Emergent cases included 4,254 laparoscopic procedures and 347 open procedures. There were 15,299 laparoscopic procedures
(97%) and 467 open procedures (3%) in total.
The number of elective cholecystectomies by gender was 8,076 female (72.3%) and
3,088 male (27.7%). There were 2,820 females (61.3%) and 1,781 males (38.7%) that underwent an emergent cholecystectomy (Figure 2). T-tests were performed for age for elective and emergent cases by gender. There was a significant difference between the age of elective and emergent cases for men and women (p<2.2E-16 and p<2.2E-16) (Table 1).
The insurance statuses for emergent and elective cases were compared to determine disparities in access to care. The most common insurance plans were Medicare and Blue Cross for elective and emergent cholecystectomies. Medicare was the top insurance plan for emergent procedure and Blue Cross was the most common insurance plan for elective procedures.
Medicaid is the third most frequent insurance plan for the emergent cases but Commercial plans is the third most frequent for elective cases. (Table 2 and Figure 3).
Census data was paired to the patient’s Zip Code information to determine rates of cholecystectomies per capita (Tables 3 and 4). The Zip Codes with greater than thirty patients for emergent procedure and greater than 90 patients for elective procedures were utilized for these models. This resulted in 34 top Zip Codes for elective case type and 35 top Zip Codes for
emergent case types. Scatter plots were constructed with the cholecystectomy rate for elective and emergent case types and socioeconomic status indicators (Figures 4, 5 and 6). The rate of emergent cholecystectomies was primarily uniform across all socioeconomic indicators. The trend for highest rates of elective cholecystectomies occurred in middle class communities with
$40,000-50,000 median household income. A higher elective cholecystectomy rate was also determined in communities with moderate percentage in poverty (15-18%) out of the studied Zip
Codes. The rate of elective cholecystectomies per capita dramatically dropped in communities that had more than 90% of individuals with a high school degree.
Limitations
This project was unable to present a strong relationship between socioeconomic status and rates of emergent and elective cholecystectomies. Several aspects of this project can be identified as limitations for this study. Pairing secondary census data to primary zip code data may not provide an accurate representation for the specific patient’s socioeconomic status.
Discussion
This study determined that the incidence for cholecystectomies from the twin tiers region is comparable to National average for males and females. The elective cases outnumber emergent cases 2.4 to 1. This may be due attributed to each surgeon’s preference to perform a cholecystectomy when gallstones are asymptomatic. Only 20% of patients with gallstones will become symptomatic and will present with cholecystitis. The higher percentage of elective procedures can be due to prophylactic removal or to early treatment of initial symptoms of cholecystitis. Laparoscopic procedures (97%) far outweighed open procedures (3%).
Laparoscopic procedures are the preferred surgical option because the recovery time and infection rates are lower than open procedures.
There was a significant difference determined between ages of patients that have undergone an elective or emergent procedure by gender. The emergent cholecystectomies had a higher average age for both genders than emergent cholecystectomies. The p- value should be noted to be extremely low due to the large sample size for both groups. While this result is significant, the average ages only differ by about 6-7 years for men and women between elective and emergent procedures.
The insurance status did show a difference in insurance types between patients that have undergone an elective or emergent cholecystectomy. Many more patients belonged to a
Medicare insurance plan that received an emergent cholecystectomy than elective cholecystectomy. This information also supports the evidence that the patient population for emergent cholecystectomies had a higher average age than the patient population receiving elective cholecystectomies. Emergent cholecystectomy patients may also have a lower socioeconomic status than elective cholecystectomy patients because a higher proportion of patients belonged to a self-pay plan and a lower percentage of patients belonged to commercial insurance plans when compared to elective cholecystectomy patients.
Secondary census data had to be applied to HANYS patient data in order to study cholecystectomy rates per capita by Zip Code for any trends across income, education level and poverty level. Findings revealed higher elective cholecystectomy rates per capita were found for communities with middle level median household incomes and communities with a poverty level between 15 and 18 percent. Elective cholecystectomy rates dropped for communities that had a
high school graduation rate greater than 90 percent. It is indeterminate at this point why these specific communities presented these unique trends across the socioeconomic indicators.
Results from this study may provide healthcare organizations with preliminary list of hot spot communities for emergent and elective cholecystectomies. This may then allow organizations with necessary information to target these communities with outreach for nutrition and healthy lifestyle initiatives in order to decrease patients’ risk factors for gallstones and cholecystitis. Healthcare organizations in these geographical areas can also sponsor information sessions for primary care providers in these communities to identify and manage high risk patients in these hot spot communities.
Future studies will compare the resources available within these various communities to determine why the rate of elective cholecystectomies is higher in middle level income communities and how some communities have lower elective procedures when there is a higher high school graduation rate. Future studies can also investigate cholecystectomy rates per capita and socioeconomic status between urban and rural communities. A national healthcare database can be utilized to obtain a comprehensive list of cholecystectomies in these regions in order to study if there is a trend for access to surgical care and type of residence. Studies will also have to include a larger patient population to study a larger geographical area.
Acknowledgements
The authors thank Guthrie Marketing Department for compiling the data for this study; Guthrie
Institutional Review Board for approving and overseeing this project; Guthrie Healthcare for supporting this project; and faculty and staff at Robert Packer Hospital for their assistance.
References
1. Digestive Diseases and Gallbladder Disease. New York Presbyterian.
<nyp.org/services/digestive/gallbladder-diseases.html>
2. Stinton, Laura M. and Eldon A. Shaffer. Epidemiology of Gallbladder Disease:
Cholelithiasis and Cancer. Gut and Liver. Apr 2012, 6(2) 172-187.
3. Gallstone Disease. Johns Hopkins University. 2013. <hopkinsmedicine.org>
4. Preeti Malladi MD et al. Laparoscopic Cholecystectomy. Sept 2014. UptoDate.
5. Society of American Gastrointestinal and Endoscopic Surgeons. Guidelines for the
Clinical Application of Laparoscopic Biliary Tract Surgery. Jan 2010.
6. I. Halldestam, E. Kullman and K Borch. Defined Indications for Elective
Cholecystectomy for Gallstone Disease. British Journal of Surgery. May 2008 Volume 95
Issue 5 620-626.
7. Danny A. Sherwinter MD. Laparoscopic Cholecystectomy. MedScape. Aug 6 2014.
8. Siddiqui, Ali A., Cholelithiasis. Merck Manual Professional Version. 2013.
9. U.S. Census Bureau. U.S. Department of Commerce. 2010.
10. TO KB, Cherry-Bukowiec JR et all. Emergent versus Elective Cholecystectomy: conversion rates and outcomes. Surgery Infection (Larchmt). December 2013; 14: 512-519.
11. Alessia G Farrarese, Mario Solej et all. Elective and Emergency Laparoscopic
Cholecystectomy in the Elderly: our experience. BMC Surgery 2013. 13: S21.
Tables
Table 1: Comparison of Age and BMI for Case Type by Gender
Elective (n=559) Emergent (n=25) P value
Men Age (mean± SD), years 52.72± 16.66
59.62± 17.49
<2.2E-16
Women Age (mean± SD), years 45.99± 17.73
51.51± 20.50
<2.2E-16
T-tests were performed for age by case type with each gender. There was a significant difference between age and case types by gender.
Table 2: Insurance Status and Cholecystectomy Case Type
Elective Surgery
Insurance Type Number of Patients
Blue Cross
Medicare
Commercial
Medicaid
4047
2510
1913
1620
Self Pay
HMO Other
Self-Insured Admin Plan
Unknown
Other Government
VA
Corrections
No Charge
Workers Compensation
375
327
139
81
78
30
27
13
5
Emergency Surgery
Insurance Type Number of Patients
Medicare
Blue Cross
Medicaid
Commercial
1741
1137
654
597
Self Pay
HMO Other
Self-Insured Admin Plan
Other Government
Unknown
VA
Corrections
No Charge
Workers Compensation
265
75
42
27
24
23
12
4
0
The insurance status for patients that have undergone an elective or emergent procedure and reside in the Twin Tiers region is displayed above. Medicare and Blue Cross were the top insurance plans that patients were enrolled.
Table 3: Elective Cholecystectomy Rate per Capita by Zip Code
ZipCode Geographic Area Population Median Houshold Income % Graduated Highschool Poverty Percent Cases Rate
16947 Troy 4818 48322 87.6
14.3
130 0.027
18421
14572
Forest City
Wayland
4754
5081
46725
42660
89.7
83.1
15
19.3
124 0.026
130 0.026
18657
18419
Tunkhannok
Factoryville
18847 Susquehanna
14801 Addison
14843
18848
14810
Hornell
Towanda
Bath
11985
4634
6024
5475
13043
9193
12356
50278
53750
38404
45810
40638
48580
43750
89.7
91.5
87.9
85.5
89.6
84
82.9
12.9
8.5
17.5
19.3
17.3
14.8
16.5
293 0.024
109 0.024
132 0.022
119 0.022
278 0.021
182 0.020
241 0.020
17724
14870
18801
14830
Canton
Painted Post
Montrose
Corning
14867
14903
Newfield
Elmira 2
18810 Athens
13901 Binghamton 1
5424
9821
8266
19850
5569
7567
6162
19773
41232
59469
49944
51902
49464
45000
43193
41344
86.4
91.2
90.3
90.9
84.9
92.8
91
89.2
16.5
7.7
11.3
15
12.7
16.8
16.8
19.2
105 0.019
190 0.019
159 0.019
342 0.017
91 0.016
123 0.016
98 0.016
311 0.016
13827 Owego
13904 Binghamton 3
13760
13865
Endicott
Windsor
18840
14845
14892
Sayre
Horseheads
Waverly
14904
13732
Elmira 3
Apalachin
14905 Elmira 4
13903 Binghamton 2
13790
14901
Johnson City
Elmira 1
13905 Binghamton 4
13850 Vestal
14850 Ithaca
11759
9579
44264
6371
10731
20453
8189
16269
8153
9070
18763
19104
16736
28026
22004
63886
56025
40985
50420
51236
48731
61005
49623
36250
74842
59159
44267
39518
28844
34520
62061
46331
91.3
85
92.8
89.7
89.9
93.7
86.3
85.1
95.3
94.8
88.1
88.8
81.1
85.5
93.8
94.1
8.8
21.9
12.2
9.1
8.8
8
14.8
25
4.5
9.8
23.4
19.2
29.9
31.6
6.8
26.9
184 0.016
148 0.015
674 0.015
97 0.015
159 0.015
299 0.015
113 0.014
224 0.014
109 0.013
121 0.013
245 0.013
244 0.013
207 0.012
311 0.011
239 0.011
380 0.006
The elective cholecystectomy rate per capita, population and socioeconomic data is displayed above. The population and socioeconomic data was obtained from U.S. Census 2010 information.
Table 4: Emergent Cholecystectomy Rate per Capita by Zip Code
ZipCode Geographic Area Population Median Houshold Income % Graduated Highschool Poverty Percent Cases Rate
18421 Forest City 4754 46725 89.7
15 54 0.0114
14904
18840
Elmira 3
Sayre
16269
10731
36250
48731
85.1
89.9
25
8.8
149
97
0.0092
0.0090
14903
14892
14845
14901
14801
Elmira 2
Waverly
Horseheads
Elmira 1
Addison
7567
8189
20453
16736
5475
45000
49623
61005
28844
45810
92.8
86.3
93.7
81.1
85.5
16.8
14.8
8
29.9
19.3
66
71
45
0.0087
0.0087
175 0.0086
140 0.0084
0.0082
13743
18657
18810
Candor
Tunkhannok
Athens
14572 Wayland
13790 Johnson City
13903 Binghamton 2
13073 Groton
3806
11985
6162
5081
19104
18763
6423
55000
50278
43193
42660
39518
44267
50561
92.1
89.7
91
83.1
88.8
88.1
90.7
6.6
12.9
16.8
19.3
19.2
23.4
12.1
31
96
48
0.0081
0.0080
0.0078
37 0.0073
137 0.0072
132 0.0070
44 0.0069
14905 Elmira 4
13904 Binghamton 3
13760 Endicott
13901 Binghamton 1
18419 Factoryville
13905 Binghamton 4
14830 Corning
14810
13827
14871
14867
13732
13850
13865
14843
18848
18801
Bath
Owego
Pine City
Newfield
Apalachin
Vestal
Windsor
Hornell
Towanda
Montrose
14870 Painted Post
16901
14850
Wellsboro
Ithaca
9070
9579
44264
19773
4634
28026
19850
12356
11759
5456
5569
8153
22004
6371
13043
9193
8266
9821
10243
63886
59159
40985
50420
41344
53750
34520
51902
43750
56025
64468
49464
74842
62061
51236
40638
48580
49944
59469
45995
46331
94.8
85
92.8
89.2
91.5
85.5
90.9
82.9
91.3
88.7
84.9
95.3
93.8
89.7
89.6
84
90.3
91.2
91.6
94.1
9.8
21.9
12.2
19.2
8.5
31.6
15
16.5
8.8
1.9
12.7
4.5
6.8
9.1
17.3
14.8
11.3
7.7
9.8
26.9
80
76
35
33
48
62
65
0.0068
0.0068
299 0.0068
133 0.0067
31 0.0067
186 0.0066
131 0.0066
0.0065
0.0065
0.0064
0.0059
0.0059
128 0.0058
36
72
0.0057
0.0055
48
43
51
0.0052
0.0052
0.0052
45 0.0044
148 0.0023
The emergent cholecystectomy rate per capita, population and socioeconomic data is displayed above. The population and socioeconomic data was obtained from U.S. Census 2010 information.
Figures
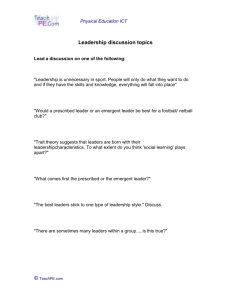
Figure 1: Primary and Secondary Service Area for Guthrie
The map above displays the primary (green) and secondary (red) service area for Guthrie
Healthcare. Patients that have undergone a cholecystectomy and reside in the region were included in the HANYS report.
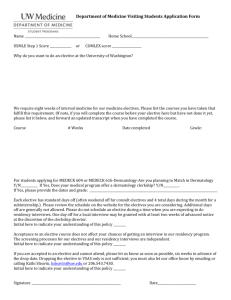
Figure 2: Cholecystectomies by Case Type and Procedure
The figure above displays the number and procedure type for elective and emergent cholecystectomies performed for patients residing in the Twin Tiers Region.
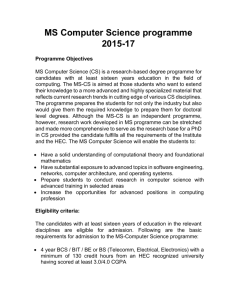
Figure 3: Insurance Status of Emergent and Elective Cholecystectomies
The insurance status for emergent cholecystectomies and elective cholecystectomies is displayed above. The majority of patients were insured by Blue Cross or Medicare in both groups.
Medicaid was the third most popular insurance type for patients that underwent an emergent cholecystectomy. Medicaid was the fourth most common insurance type for elective cholecystectomies.
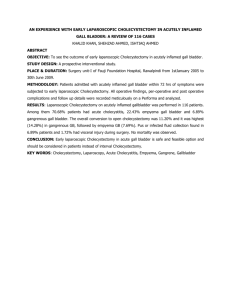
Figure 4: Elective and Emergent Cholecystectomy Rates per Capita and Median Income by Zip
Code
The figure above displays the cholecystectomy rate per capita and median income by Zip Code.
Elective procedures are displayed in black and emergent procedures are displayed in red. A higher cholecystectomy rate trend occurs between 40,000 and 50,000 for elective procedures.
The trend for emergent procedures is uniform across all median household incomes.
Figure 5: Elective and Emergent Cholecystectomy Rates per Capita and Percentage Graduated
High School by Zip Code
The figure above displays the cholecystectomy rate per capita and percentage of the population that have graduated high school by Zip Code. Elective procedures are displayed in black and emergent procedures are displayed in red. The trend for elective cholecystectomy rates per capita drops after the percentage of the population with a high school degree passes 90 percent.
The trend for emergent procedures is uniform across all graduation percentages.
Figure 6: Elective and Emergent Cholecystectomy Rates per Capita and Percentage in Poverty by Zip Code
The figure above displays the cholecystectomy rate per capita and percentage of the population in poverty by Zip Code. Elective procedures are displayed in black and emergent procedures are displayed in red. The trend for elective cholecystectomy rates is greatest when the poverty level is between 15 and 18 percent.