An Investigation in Surgical Cases and
advertisement

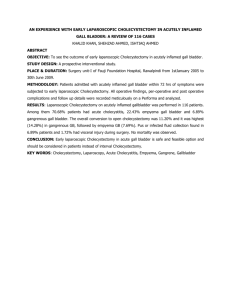
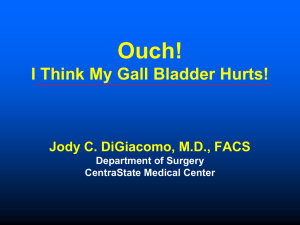
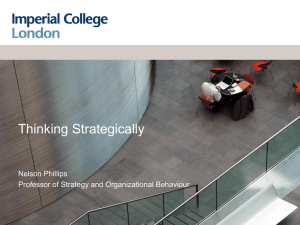
An Investigation in Surgical Cases and Socioeconomic Status of Guthrie Patients Connor Zale, Thomas J. VanderMeer M.D. and Laura Fitzgerald Department of Research at Robert Packer Hospital Guthrie Healthcare 1 Guthrie Square, Sayre, PA 18840 Abstract This project was designed to analyze if there is a disparity in access to surgical care due to socioeconomic status for patients in the Twin Tiers region. Elective and emergent cholecystectomies were used as indicators for access to surgical care. Socioeconomic status was determined by insurance status, education, and income. Guthrie’s Epic System was accessed in order to obtain patient records that have undergone a cholecystectomy between 1/11/2011 to 3/31/2012. The report collected 584 patient records and elective cases (559, 95.72%) outnumbered emergent cases (25, 4.28%). Laparoscopic cases (562, 96.23%) were the preferred procedure compared to open procedures (22, 3.77%) with a 0.707% conversion rate. Generalized linear models were constructed using cholecystectomy rates per capita by zip code and socioeconomic census data, median income and percentage of high school graduates. No definitive trend for elective and emergent cholecystectomies and socioeconomic status could be determined from the current data. Limitations can be attributed to the small sample size and physician referral to nonGuthrie hospitals. Continued research will seek to include all patients that have undergone a cholecystectomy in the Twin Tiers region using national healthcare data in order to the study if a trend exists between socioeconomic status and cholecystectomy case type. Introduction Diseases of the gallbladder are the most commonly treated of all the digestive system diseases. The two primary types of gallbladder disease are gallstones, cholelithiasis, and gallbladder cancer1. Gallstones affect large portion of Americans and treatment of gallstones has become a substantial portion of the national healthcare cost. It has been estimated that over 20 million Americans suffer from gallstones. Gallbladder disease has been approximated to consume 6.2 billion dollars annually and it has increased over 20% over the last 3 decades2. Due to the enormous amount spent on cholecystectomies each year, this surgical procedure was selected to model patients’ access to care. It was hypothesized that patients with higher socioeconomic status will undergo the procedure electively and patients from a lower socioeconomic status will delay the procedure. This may cause a higher proportion of emergent cholecystectomies for patients of lower socioeconomic status. The gall bladder is a small organ that lies underneath the liver and it is connected to the duodenum by the common bile duct. The role of the gallbladder is to store bile which is produced by the liver and the bile is stored until it is released into the duodenum in order to digest fats. Bile is composed of bile salts, bilirubin and cholesterol. Gallstones can be composed of hardened cholesterol or complexes of calcium salts, bilirubin, copper, cholesterol and protein3. There are several risk factors for an increased incidence of gallstones. The primary risk factors are age, gender, number of pregnancies, BMI, oral contraceptives, estrogen therapy, family history and genetics. It has been noted that increased age results in an increased risk for gallstones and cholecystitis. Females are 2.4 times more likely to have gallbladder issues than men due to hormones, estrogen and progesterone. Obesity has also been determined to be a risk factor for gallstone formation8. The presence of gallstones may not cause symptoms until complications arise such as, inflammation, infection and obstruction of the common bile duct. Patients that experience symptoms from gallstones commonly state the presence of biliary colic which is a visceral pain that is believed to be caused by the obstruction of the cystic duct. Patients can be treated for gallstones with surgical and non-surgical interventions. An oral dose of bile acids can assist in the treatment of gallstones by medical dissolution therapy. The common surgical treatments are open or laparoscopic cholecystectomy and open or laparoscopic cholecystostomy. A cholecystectomy is the complete removal of a gallbladder and primarily is completed as laparoscopic procedure. A cholecystostomy is the process of forming an opening in the gallbladder and a tube is placed inside the gallbladder for drainage. A cholecystostomy is usually performed when there are preexisting issues that to do not make a cholecystectomy possible4. The Society of American Gastrointestinal and Endoscopic Surgeons provide guidelines for laparoscopic operations on the gallbladder and biliary tree, which allow procedures for symptomatic cholelithiasis, biliary dyskinesia, acute cholecystitis and complications related to the common bile duct stones5. A cholecystectomy can be determined to be elective in most cases when the complications of gallstones due not pose an immediate threat to the patient. A cholecystectomy can be advised to the patient when biliary colic is negatively affecting the patient and the patient does not have any major issues in order to undergo surgery6. Other indications for a prophylactic cholecystectomy include calculi greater than 3 cm in diameter for individuals from regions with a higher prevalence of gallbladder cancer, a chronically obliterated cystic duct, a nonfunctioning gallbladder, a calcified gallbladder, a gallbladder polyp larger than 10 mm and growing in size, gallbladder trauma or an anomalous junction of the pancreatic and biliary ducts7. Methods Electronic Medical Records were accessed using Robert Packer Hospital’s EPIC System. Records were collected for patients that underwent an open or laparoscopic cholecystectomy between 1/11/2011 and 3/31/2012. Age, race, gender, zip code, BMI, procedure and case type (elective or emergent) was obtained for analysis. Emergent cholecystectomies were identified by an emergency room code that was attached to the case type within the EPIC report. Insurance status was obtained from billing department. Pregnant women and children were excluded from this study. Patient zip code was paired to U.S. Census data for median income and percentage of population with at least a high school level degree. T-tests were performed for age and BMI by case type for each gender separately. Insurance status for emergent cases was compared to institutional data for all patients at Robert Packer Hospital and Corning Hospital. General linearized models were constructed using median income and high school graduation rate to determine if there was a correlation to rate of cholecystectomies per capita. Statistical tests were conducted using R software. This project was reviewed and approved by Guthrie Institutional Review Board prior to data collection. This project was determined to be a minimal risk study because the only patient identifier, B number, was removed prior to statistical analysis. A waiver for patient consent was obtained for this study since it was a retrospective chart review by design. Results The EPIC report collected 584 total cholecystectomy cases at Robert Packer Hospital (RPH) and Corning Hospital (Figure 1). There were 559 elective cases (95.72%) and 25 emergent cases (4.28%). The elective cases included 537 laparoscopic procedures and 22 open procedures. Emergent cases were only performed laparoscopically. There were 562 laparoscopic procedures (96.23%) and 22 open procedures (3.77%) in total. The conversion rate from laparoscopic to open procedure was 0.7067%. The number of elective cholecystectomies by gender was 401 female (71.74%) and 158 male (28.26%). There were 18 females (72%) and 7 males (28%) that underwent an emergent cholecystectomy (Figure 2). The patient population was reported to be 98.1% white. T-tests were performed for age and BMI for elective and emergent cases by gender. The collected BMI cases were matched for age, race, gender and number of cases between elective and emergent cases. There was no significant difference between the age of elective and emergent cases for men and women (p=0.604 and p=0.737) (Table 1). There also was no significant difference between the BMI of elective and emergent cases for men and women (p=0.298 and p=0.305). The insurance status for emergent, RPH and Corning Hospital were compared to determine disparities in access to care. The primary insurance plans were Medicare and Blue Cross among all three groups. Medicaid is the third most frequent insurance plan for the emergent cases but Commercial plans is the third most frequent for RPH and Corning Hospital. (Figure 3). Census data was paired to the patient’s zip code information to determine rates of cholecystectomies per capita (Tables 2, 3 and 4). General linearized models were created with median income and percentage of the population graduated high school to model cholecystectomy rate per capita by zip code (Table 5 and Figure 4). The zip codes with greater than nine patients were utilized for the model. This incorporated a total of twelve zip codes for the model including all cholecystectomy cases. General linearized models were also constructed for emergent and elective cholecystectomy rates per capita using median income and high school graduation information (Table 6 and Figure 5). The zip codes including more than 9 cases were used for the elective cases. This included a total of 12 zip codes. All zip codes for the emergent cases were used which included 13 unique zip codes. The constant value of 1 produced the lowest AIC value of -12.42 for the models of cholecystectomy rates per capita. The lowest AIC value of -14.56 for elective case models occurred for the constant value of 1. Emergent cases were best modeled by median income with an AIC value of -48.44 but the constant value of 1 produced a very similar AIC value of -48.31. Limitations This project was unable to present a clear analysis for a correlation between socioeconomic status and rates of emergent and elective cholecystectomies. Several aspects of this project can be identified as limitations for this study. The cholecystectomy rates per capita were not accurate due to physician referral. All data was obtained from Guthrie Healthcare EPIC data. Cholecystectomy rates performed at neighboring hospitals were not included in the data selection. Pairing secondary census data to primary zip code data may not provide an accurate representation for the specific patient’s socioeconomic status. The sample size was also too small to determine insurance, education, or income trends for cholecystectomy rates per capita. Discussion This study determined that the incidence for cholecystectomies from Guthrie data is comparable to National average for males and females. The elective cases outnumber emergent cases 22 to 1. This may be due attributed to each surgeon’s preference to perform a cholecystectomy when gallstones are asymptomatic. Only 20% of patients with gallstones will become symptomatic and will present with cholecystitis. The larger percentage of elective procedures can be due to prophylactic removal or to early treatment of initial symptoms of cholecystitis. Laparoscopic procedures (96.23%) far outweighed open procedures (3.77%). Laparoscopic procedures are the preferred surgical option because the recovery time and infection rates are lower than open procedures. The institutional data did not present an association between emergent cases and insurance status but this may be due to the low number of emergent cases that were studied. There also was no significant difference between BMI and age by gender for elective and emergent cases. Since Guthrie data does not contain patient information on income or education level, current Guthrie data does not allow for identification of vulnerable and at risk patients according to socioeconomic status. Secondary census data had to be applied to Guthrie patient data in order to design linear models for income, education level and cholecystectomy rates. No definitive correlation could be determined for socioeconomic status and rates of elective or emergent cholecystectomies. This was concluded due to the constant value of 1 model being a better predictor for cholecystectomy rate per capita than socioeconomic indicators, such as income and education level. Results from this study have provided Guthrie Healthcare with preliminary list of hot spot communities for emergent and elective cholecystectomies. This allows Guthrie with necessary information to target these communities with outreach for nutrition and healthy lifestyle initiatives in order to decrease patients’ risk factors for gallstones and cholecystitis. Guthrie can also sponsor information sessions for primary care providers in these communities to identify and manage high risk patients in these hot spot communities. Future studies can provide a more accurate analysis for cholecystectomy rates per capita and socioeconomic status by including all cholecystectomies performed in the Twin Tiers region. A national healthcare database can be utilized to obtain a comprehensive list of cholecystectomies in this region in order to study if there is a trend for cholecystectomy case type and socioeconomic status. Studies will also have to include a larger patient population due to the low number of emergent cases in order to further study insurance type and procedure. Acknowledgements The authors thank Guthrie EPIC Report Team for compiling data for this study; Guthrie Institutional Review Board for approving and overseeing this project; Guthrie Healthcare for supporting this project; and faculty and staff at Robert Packer Hospital for their assistance. References 1. Digestive Diseases and Gallbladder Disease. New York Presbyterian. <nyp.org/services/digestive/gallbladder-diseases.html> 2. Stinton, Laura M. and Eldon A. Shaffer. Epidemiology of Gallbladder Disease: Cholelithiasis and Cancer. Gut and Liver. Apr 2012, 6(2) 172-187. 3. Gallstone Disease. Johns Hopkins University. 2013. <hopkinsmedicine.org> 4. Preeti Malladi MD et al. Laparoscopic Cholecystectomy. Sept 2014. UptoDate. 5. Society of American Gastrointestinal and Endoscopic Surgeons. Guidelines for the Clinical Application of Laparoscopic Biliary Tract Surgery. Jan 2010. 6. I. Halldestam, E. Kullman and K Borch. Defined Indications for Elective Cholecystectomy for Gallstone Disease. British Journal of Surgery. May 2008 Volume 95 Issue 5 620-626. 7. Danny A. Sherwinter MD. Laparoscopic Cholecystectomy. MedScape. Aug 6 2014. 8. Siddiqui, Ali A., Cholelithiasis. Merck Manual Professional Version. 2013. 9. U.S. Census Bureau. U.S. Department of Commerce. 2010. 10. TO KB, Cherry-Bukowiec JR et all. Emergent versus Elective Cholecystectomy: conversion rates and outcomes. Surgery Infection (Larchmt). December 2013; 14: 512-519. 11. Alessia G Farrarese, Mario Solej et all. Elective and Emergency Laparoscopic Cholecystectomy in the Elderly: our experience. BMC Surgery 2013. 13: S21. Tables Table 1: Comparison of Age and BMI for Case Type by Gender T-tests were performed for age and BMI by case type with each gender. There was no significant difference between age and BMI for case types by gender. Samples were controlled for age, race, gender and number of cases to test differences in BMI between case types. Table 2: Cholecystectomy Rate per Capita by Zip Code The cholecystectomy rate per capita, population and socioeconomic data is displayed above. The population and socioeconomic data was obtained from U.S. Census 2010 information. Table 3: Elective Cholecystectomy Rate per Capita by Zip Code The elective cholecystectomy rate per capita, population and socioeconomic data is displayed above. The population and socioeconomic data was obtained from U.S. Census 2010 information. Table 4: Emergent Cholecystectomy Rate per Capita by Zip Code The emergent cholecystectomy rate per capita, population and socioeconomic data is displayed above. The population and socioeconomic data was obtained from U.S. Census 2010 information. Table 5: AIC Values for Cholecystectomy Linear Models The AIC values for cholecystectomy linear models are displayed above. The best predictive model uses a constant value of one. This may be due to lack of comprehensive list of cholecystectomy cases by zip code. Table 6: AIC Values for Elective and Emergent Cholecystectomy Linear Models The AIC values for elective and emergent cholecystectomy linear models are displayed above. The best predictive model uses a constant value of one for the elective cholecystectomies per capita by zip code. The model median income model for emergent cholecystectomies produced an AIC value that is very similar to the constant value of one model. This results in a model with weak predictive ability for emergent cholecystectomies per capita by zip code. This may be due to lack of comprehensive list of cholecystectomy cases by zip code. Figures Figure 1: Cholecystectomies at Guthrie by Case Type and Procedure The figure above displays the number and procedure type for elective and emergent cholecystectomies performed at Guthrie hospitals. Figure 2: Elective and Emergent Surgeries by Gender The number of elective and emergent cholecystectomies by gender is displayed above. There were 401 females and 158 males that underwent an elective cholecystectomy. 18 Females and 7 males were reported to have an emergent cholecystectomy. Figure 3: Insurance Status of Emergent Cholecystectomies and Institutional Data The insurance status for emergent cholecystectomies and institutional data is displayed above. The majority of patients were insured by Blue Cross or Medicare in all three groups. Medicaid was the third most popular insurance type for patients that underwent an emergent cholecystectomy. Medicaid was the fourth most common insurance type for RPH and Corning Hospital patients. Figure 4: Correlation for Cholecystectomy Rate per Capita and Median Income by Zip Code The graph above displays a linear model for rate of cholecystectomies per capita and median income by zip code. Figure 5: Correlation for Elective and Emergent Cholecystectomy Rate per Capita and Median Income by Zip Code The graph above displays linear models for rate of elective and emergent cholecystectomies per capita and median income by zip code.