DRAFT Key Points: Ensure patient has a personal asthma action
advertisement

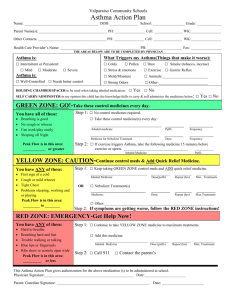
BCCG Formulary Choices: Asthma Treatment Guidelines for Adults and children over 12 years Key Points: Ensure patient has a personal asthma action plan which includes warning signs of poor asthma control and what to do during an attack Start treatment at the step most appropriate to initial severity of their asthma. Patients should receive training for each device prescribed, and be able to demonstrate satisfactory technique. Try to limit number of different devices a patient has Check concordance and reconsider diagnosis if response to treatment is unexpectedly poor. Perform yearly asthma review Consider a spacer device for patients prescribed a metered dose inhaler (MDI) who are: o Having difficulty co-ordinating actuation and inhalation. o Receiving high doses of inhaled corticosteroid (ICS) (>800 mcg of beclometasone or equivalent daily). Indicators associated with increased risk of death (from NRAD report) Recent hospitalisation Previous severe attacks Non-attenders for planned review LABA monotherapy without ICS Using more than 12 reliever inhalers per year Using less than 12 preventer inhalers per year Step 1: Inhaled SABA prn Salbutamol MDI 100mcg / dose inhaler CFC free 1-2 puffs PRN Stepping Up? Think T.T.T. Adherence with Therapy- Do they use it? Technique- Can they use it? Trigger factors Refer to Community pharmacist for New Medicine Service or Medicine Use Review. Step 2: Add in regular ICS [BDP 400mcg/day] Clenil Modulite® (beclometasone) 100 microgram per dose + / - spacer 2 puffs twice daily Can decrease dose if controlled Step 3 - initial: Replace with LABA/ICS combination Fostair® CFC free inhaler (beclometasone / formoterol) 100 microgram / 6 microgram +/- spacer 1 puff twice daily [BDP 500 mcg/day] (Child 12-17 years) Symbicort 200/6 Turbohaler® [BDP 400-800 mcg / day] 1 or 2 puffs twice daily reduced to 1 puff once daily if control maintained. Can decrease dose if controlled Step 3 – follow on: Benefit from LABA/ICS but inadequate response, increase ICS dose in combination inhaler Fostair® CFC free inhaler (beclometasone / formoterol) 100 microgram / 6 microgram +/- spacer 2 puffs twice daily [BDP 1000mcg/day] If no response to LABA/ICS, review diagnosis. Stop LABA and initiate higher dose ICS [BDP 800mcg/day] Clenil Modulite® (beclometasone) 200 microgram per dose + / - spacer 2 puffs twice daily If asthma still not controlled add either a leukotriene receptor antagonist (LTRA) (Montelukast 10mg tablets in the evening; (Child 12 – 15 years- Montelukast 5mg tablets or chewable tablets 5mg in the evening) or SR theophylline (Phyllocontin Continus® tablets 225mg twice daily for one week then increased to 2 tablets twice daily if necessary.) Maintenance and reliever therapy Consider only for stable patients on step 3 with a personal asthma plan able to manage their own treatment. Caution – can become expensive and needs closer monitoring of patient / prescriptions. Only consider for patients using < 2 SABA inhalers per year. Use Fostair® CFC free inhaler (beclometasone / formoterol) 100 microgram / 6 microgram +/- spacer 1 puff twice daily; for the relief of symptoms 1 puff as needed; max. 8 puffs daily. Step 4: Consider trial of: Increasing ICS dose up to BDP 2000mcg/day – Clenil Modulite® (beclometasone) 200 microgram per dose +/- spacer up to 4 puffs twice daily or Clenil Modulite® (beclometasone) 250 micrograms per dose +/- spacer up to 4 puffs twice daily . If previously on ICS/LABA add in formoterol Easyhaler® 12 mcg/dose 1 puff twice daily. Or addition of either a LTRA (Montelukast 10mg tablets in the evening; (Child 12 – 15 years- Montelukast 5mg tablets or chewable tablets 5mg in the evening) or SR theophylline (Phyllocontin Continus® tablets 225mg twice daily for one week then increase to 2 tablets twice daily if necessary.) If trial of an add-on treatment is ineffective seek specialist advice before proceeding. Stepping Down? Reduce ICS dose slowly Aim to use the lowest effective ICS dose Consider a treatment review every 12 weeks Step 5: Refer to respiratory specialist Flow chart based on recommendations from the British Thoracic Society and Scottish Intercollegiate Guidelines Network BCCG Formulary Choices: Asthma Treatment Guidelines for Children aged 5 to 12 years Key Points: Ensure patient has a personal asthma action plan which includes warning signs of poor asthma control and what to do during an attack Start treatment at the step most appropriate to initial severity of their asthma. Patients should receive training for each device prescribed, and be able to demonstrate satisfactory technique. Try to limit number of different devices a patient has. Metered dose inhaler (MDI) with a spacer device is the preferred option for children Check concordance and reconsider diagnosis if response to treatment is unexpectedly poor. Perform yearly asthma review Regularly review the use of high dose inhaled corticosteroids in children Indicators associated with increased risk of death (from NRAD report) Recent hospitalisation Previous severe attacks Non-attenders for planned review LABA monotherapy without ICS Using more than 12 reliever inhalers per year Using less than 12 preventer inhalers per year Stepping Up? Think T.T.T. Step 1: Inhaled SABA prn up to once daily Salbutamol MDI 100mcg / dose inhaler CFC free + / - spacer 1-2 puffs PRN Adherence with TherapyDo they use it? TechniqueCan they use it? Trigger factors Refer to Community pharmacist for New Medicine Service or Medicine Use Review. Step 2: Add in regular ICS Clenil Modulite® (beclometasone) 100 microgram per dose + spacer 1 puff twice daily [BDP 200mcg/day] Can decrease dose if controlled consider alternative preventer if ICS cannot be used i.e. Leukotriene receptor antagonist (LRTA) (5 years – Montelukast chewable tablets 4mg in the evening; 6-12 years Montelukast chewable tablets 5mg in the evening.) Step 3 - initial: Replace with LABA/ICS combination Symbicort 100/6 Turbohaler® (6-12 years 2 puffs twice daily) [BDP 400 mcg / day] Step 3 – follow on: If no response to LABA/ICS, review diagnosis. Discontinue LABA and continue ICS Clenil Modulite® (beclometasone) 100 microgram per dose + spacer 2 puffs twice daily [BDP 400mcg/day] If asthma still not controlled add either LTRA (5 years – Montelukast chewable tablets 4mg in the evening; 6-12 years Montelukast chewable tablets 5mg in the evening) or SR theophylline (Phyllocontin Continus® tablets 225mg – body weight over 40kg initially one tablet twice daily increased after 1 week to 2 tablets twice daily according to plasma theophylline concentrations) Step 4: Consider trial of: Increasing ICS dose up to BDP 800 mcg/day – Clenil Modulite® (beclometasone) 100 microgram per dose + spacer up to 4 puffs twice daily plus Formoterol Easyhaler® 1 puff (up to 2 puffs) twice daily if LABA of benefit. Consider risk vs benefit of using off label combination ICS/LABA in children Symbicort 200/6 Turbohaler® (6-12 years -up to 2 puffs twice daily) [up to BDP 800mcg / day] Or addition of either a LTRA (5 years – Montelukast chewable tablets 4mg in the evening; 6-12 years Montelukast chewable tablets 5mg in the evening) or SR theophylline (Phyllocontin Continus® tablets 225mg – body weight over 40kg initially one tablet twice daily increased after 1 week to 2 tablets twice daily according to plasma theophylline concentrations) If trial of an add-on treatment is ineffective seek specialist advice before proceeding. Stepping Down? Reduce ICS dose slowly Aim to use the lowest effective ICS dose Consider a treatment review every 12 weeks Step 5: Refer to respiratory specialist Flow chart based on recommendations from the British Thoracic Society and Scottish Intercollegiate Guidelines Network Flow chart based on recommendations from the British Thoracic Society and Scottish Intercollegiate Guidelines Network