Erythropoietin in the Increase of Quality of Life and Survival of the

Is there a role to erythropoiesis-stimulating proteins in the treatment of anemic chronic heart failure patients: a meta-analysis of randomized controlled trials
Bárbara Vieira, barbara_n_vieira@hotmail.com
; Diana Pires, dianaifpires@hotmail.com
;
Iolanda Vieira, yolanda_vieira_15@hotmail.com
;
João Novo, joão_novo26@hotmail.com; José
Machado, jpnamora@sapo.pt
; Lia Rodrigues, liajmr@gmail.com
; Maria Lume, maria_j_c_lume@hotmail.com
;
Mário Sousa, med060809@med.up.pt
;
Mónica Pereira, monicapereira_mdl@hotmail.com
;
Patrícia Gouveia, patirigouveia@hotmail.com
; Pedro Vieira pedro.manuel.vieira@hotmail.com
Dra. Filipa Almeida, turma 6
ABSTRACT:
Problem: The study aim is to define if treatment of anemia with erythropoietin stimulating proteins influences and improves survival, prognosis and quality of life of severe heart failure patients.
Summary of background: Anaemia is frequently observed in patients with chronic heart failure
(CHF). Erythropoietin (EPO) is a glycoprotein hormone that acts on erythroid stem cells of the bone marrow to stimulate proliferation and differentiation. It has been successfully used in the treatment of many types of anaemia.
Methods: We performed a systematic review and meta-analysis of randomized controlled trials reporting outcomes of heart failure patients with anaemia treated with erythropoietin stimulating proteins (ESP) versus placebo or iron therapy. Our systematic review compares ESP therapy with standard care in severe CHF patients published in Medline, IsiWeb of Knowledge and Scopus. Data were analyzed using the software SPSS 16 ® and the meta-analysis software in Review Manager 5 ® .
Results: The electronic search retrieved 1187 eligible articles. 1174 were rejected initially and the other 13 were detailed evaluated and 5 of them were rejected. 8 studies were included in the metaanalysis. The outcomes selected to the meta-analysis were exercise duration (p< 0.00001)), sixminute walk distance (p= 0.03), left ventricular ejection fraction (LVEF) (p=0.02) and the peak Vo
2
(p=0.03), New York Heart Association classification (p=0.01), serum ferritin (p=0.92), haemoglobin concentration(p<0.00001) and mortality (p=0.48).
Conclusion: The advantages of erythropoietin administration in patients with HF and anaemia are significant, this treatment should, therefore, be considered a serious therapeutic option.
KEY WORDS: Anaemia, Chronic heart failure, Erythropoietin
INTRODUCTION: Heart failure (HF) is a condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Chronic HF refers to a persistent symptomatic HF and is the most common form of HF leading to hospital admission, accounting for 80% of cases [1]. The prevalence of HF is between 2 and 3% and rises sharply at 75 years old, so the prevalence in 70 to
80-year-old people is between 10 and 20% [2].
Anaemia is frequently observed in patients with chronic heart failure (CHF). Prevalence of anaemia depends both on the severity of CHF and diagnostic criteria used to define it. Using the most commonly employed definition of the World Health Organization (Haemoglobin [Hb] <12g/dL in women and <13g/dL in men), anaemia is present in one-third of the CHF patients [3, 4]. Its pathogenesis in CHF is complex and renal dysfunction, inflammation; changes in plasma volume, hematinic deficiencies, and drug treatment are common causes [5].
Anaemia in patients with HF is frequently associated with a substantially decreased aerobic capacity, a subjective experience of fatigue and reduced functional status and poor quality of life. Anaemia in
CHF is independently associated with increased morbidity and mortality, and is considered as a useful prognostic marker [3], suggesting that treatment for anaemia should benefit patients
.
The recognition of the high prevalence and the independent prognostic role of anaemia in HF have contributed to intensification of research for an effective treatment.
Erythropoietin (EPO) is a glycoprotein hormone that acts on erythroid stem cells of the bone marrow to stimulate proliferation and differentiation. It has been successfully used in the treatment of many types of anaemia such as anaemia due to kidney failure [6] and anaemia associated with cancer [7].
A central role of erythropoietin in cardiorenal anaemia syndrome has been proposed. Treatment of anaemia with erythropoiesis-stimulating proteins in patients with CHF would thus seem attractive and has been explored in several studies [3, 8-12]. Several randomized controlled trials (RCT) have demonstrated the safety and efficacy of erythropoietin-stimulating proteins (ESP) in correcting anaemia in patients with HF. However, as some studies have failed to show benefit, the role of this novel therapy in the treatment of HF is not defined.
The aim of this study is to define if treatment of anemia with erythropoietin stimulating proteins influences and improves survival, prognosis and quality of life of severe heart failure patients.
METHODS
Study objectives and design: We performed a systematic review and metanalysis of randomized controlled trials reporting outcomes of heart failure patients with anaemia treated with erythropoietin stimulating proteins versus placebo or iron therapy. The primary endpoints evaluated were effects of the therapy in mortality rates, prognosis defined as readmission rates, NYHA functional class, exercise capacity and quality of life, evaluated with validated questionnaires. The second endpoint
was evaluation of complication rates and safety of erythropoietin stimulating proteins treatment. The outcomes of interest were mortality, readmission rates, left ventricle ejection fraction, NYHA functional class, exercise capacity defined by oxygen consumption in the exercise test and 6 min walking test and vascular complications.
Search Strategy : We preformed a Systematic review of randomized controlled trials that compare
ESP therapy with standard care in severe CHF patients published in Medline, IsiWeb of Knowledge and Scopus, since 1985 (year when ESP were first described and synthesised) until February 2009.
In the search criteria defined the Mesh Terms: heart failure; anemia; erythropoietin recombinant and the text words: heart failure; congestive heart failure; chronic heart failure; heart insuficiency; systolic dysfunction; symptomatic heart failure; anemia; epoetin delta; erythropoiesis stimulating protein, human; darbepoetin alfa; recombinant erythropoietin; erythropoietin; erythropoietin recombinant, were used. The final query used to select the articles was: ("Heart Failure“ [Mesh] OR "heart failure“
[All Fields] OR "congestive heart failure“ [All Fields] OR "chronic heart failure“ [All Fields] OR "systolic dysfunction“ [All Fields] OR "symptomatic heart failure“ [All Fields])
AND ("Anaemia
“ [Mesh] OR
"anaemia
“ [All Fields] OR "anaemia“ [All Fields])
AND
("Erythropoietin, Recombinant“ [Mesh] OR
"epoetin delta“ [Substance Name] OR "erythropoiesis stimulating protein, human“ [Substance Name]
OR "darbepoetin alfa“ [Substance Name] OR "recombinant erythropoietin“ [All Fields] OR
"erythropoietin“ [All Fields] OR "erythropoietin“ [MeSH Terms] OR "erythropoietin recombinant“ [All
Fields])
Study Selection : We included randomized controlled trials whose primary objective was to compare
ESP treatment in CHF patients with placebo or iron therapy. Titles and abstracts of all articles were evaluated independently by two reviewers and rejected on initial screen if they: 1) included subjects other than CHF patients or evaluated erythropoietin therapy in other diseases; 2) had no evaluation of hemoglobin (Hb) or hematocrit (Ht) levels; 3) were not randomized controlled trials; 4) were published only in abstract form; 5) were published in another language than English or Portuguese.
After obtaining full texts of the selected studies, the same reviewers independently assessed eligibility according to the following criteria: 1) studies that compared Erythropoietin group or erythropoietin + iron therapy vs placebo group or iron therapy; 2) studies where treatment of heart failure other than ESP is optimize in the 2 groups; 3) Articles that evaluate prognosis, mortality and quality of life; 4) articles addressing animal experiments and not phase III or IV RCT. Differences in data between the 2 reviewers were solved by rereviewing corresponding articles, and the final set was agreed on by consensus.
Data extraction : Two reviewers extracted independently pre-specified data elements from each study, and data was organized in five different categories: study sample, effect of ESP treatment on anaemia, effect of ESP on mortality and prognosis, effect on quality of life and complication events.
Charts were used to compile the data of each category. The following variables we created according to the four categories: (1) study sample variables: total patients in each group, age and heart failure treatment; (2) effect of ESP treatment on anaemia variables: hemoglobin level and serum ferritin for each group before and after treatment; (3) effect of ESP on mortality and prognosis variables: NYHA, left ventricle ejection fraction, peak of oxygen volume, distance in the 6 min walking test, in each group before and after treatment and mortality in the two groups; (4) quality of life variables: type of questionnaire used, global score before and after intervention in the 2 groups; (5) complication events variables: which complication event and incidence per group.
Statistical analysis : Data were analyzed using the software SPSS 16
®
on an intention to treat basis.
Where appropriate, data from all trials were combined using the meta-analysis software in Review
Manager 5
®
. Random effects meta-analysis was conducted to determine a summary estimate of the relative risk and the 95% confidence interval and estimate the magnitude of the effect of ESP treatment in anemic heart failure patients and the primary endpoints determined. We performed tests of heterogeneity between studies using a standard chi-square test and I2 statistic.
Statistical significance was set at p < 0.05.
RESULTS:
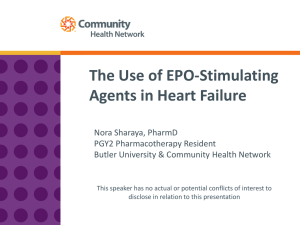
Potential eligible studies screened
(n= 1187)
Description of the included articles: The electronic search retrieved 1187 eligible articles. On initial screening, 1174 were rejected based on title and abstract and the other 13 were detailed evaluated. Of
Potential eligible studies that were detailed review
(n = 13)
Reject based on title and abstract
(n = 1174)
Reject based on full text article
(n =5) the 13 screened full text articles, 5 were rejected. Thus
8 studies were included in this meta-analysis (Fig.1).
The characteristics of the included articles are listed
Table 1. Data were analyzed using the software SPSS
16
®
on an intention to treat basis and data from all trials were combined using the meta-analysis software in
Review Manager 5
®
.P-values up to 0,1 indicates homogeneity.
Meta-analysis findings: According to the information available in the 8 articles, the outcomes selected to the
Studies included in meta-analysis
(n= 8)
Figure 1 Flow Chart for articles selection meta-analysis were exercise duration, six-minute walk distance, left ventricular ejection fraction (LVEF) and the peak Vo
2
, serum ferritin, haemoglobin concentration, mortality (objective variables), and New
York Heart Association classification (subjective variable). To evaluate the efficiency of the treatment with erythropoietin were also analysed the variation of haemoglobin concentration and serum ferritin.
On the other hand duration of exercise data was available in 4 articles [14, 17, 21] and its analysis showed a statistically significant increase (p < 0.00001) of the distance walked (Fig.3). Relatively to the heterogeneity test, it was homogeneous (95% CI; p=0.59). Six-minute-walk distance improved with erythropoietin administration.
Six-minute-walk distance data was available in 4 articles [15, 18, 20, 21] . Analysis revealed that there is a statistically significant improvement (p = 0.03) of this outcome in patients treated with erythropoietin compared with placebo group (Fig.2). The p-value of heterogeneity test (95% CI; p=0.01) indicates that exercise duration data is heterogeneous.
Left ventricular ejection fraction, an efficiency marker, was measured in 4 studies. The mean LVEF increased significantly (p = 0.02) in patients treated with erythropoietin compared with placebo group
(Fig.4) and its test was heterogeneous (95% CI; p=0.009).
Peak Vo
2
was evaluated in 3 articles [14, 17, 21] and analysis shows that it significantly increased (p
= 0,03) in treatment group compared with placebo (Fig.5) while the heterogeneity test p-value demonstrated that this variable is heterogeneous (95% CI; p=0.0002). Although the heterogeneity graph represents an homogeneous distribution.
Changes in New York Heart Association classification were evaluated in 6 articles [15, 16, 17, 18, 19,
20]. Data analyse revealed a significant decrease (p = 0,01) in NYHA class in experimental group compared with placebo group (Fig.6) and meta-analysis showed that NYHA class has an heterogeneous distribution (95% CI; p<0.00001).
Mortality was considerate in all 8 articles which promote a better analysis with efficient results. There is no significant difference (p = 0,48) between the groups (Fig.7) and its distribution is homogeneous according to the heterogeneity test (95% CI; p=0.33).
Variation in Haemoglobin (Hb) concentration was monitored in 7 articles [14, 15, 16, 17, 18, 20, 21].
There was a significantly increase in Hb concentration (p < 0.00001) as result of the administration of erythropoietin (Fig.8). Hb concentration distribution is homogeneous according to the test of heterogeneity (95% CI; p=0.08). Although this heterogeneity is not too much significant as the pvalue indicates because it is not to much lower than 0.1 and the heterogeneity graph representation also doesn’t show a bigger heterogeneity.
Serum ferritin was measured in only 3 articles [15, 16, 18] and there is no significantly changes (p =
0,92) between the study groups (Fig.9). The heterogeneity test indicates an homogeneity in the distribution of serum ferritin data (95% CI; p=0.27).
Table 1
Article identifiation
1
2
3
4
5
6
7
8
Description of the included articles
Title Authors
N placebo
N study
Age
(Placebo)
Age (Study) Outcomes
Effect of darbepoetin alfa on exercise tolerance in anemia patients with symptomatic chronic heart failure
Piotr Ponikowski, MD,
PHD, Stefan D. Anker, et al 22 19 72 ± 7 70 ± 7
Mortality, hemoglobin, exercise duration, peak
VO
2
.
Randomized, doubleblind, placebo- controlled study o evaluate the effect of two dosing regimens of darbepoetin alfa in patients with heart failure and anaemia
Dirk J. van Veldhuisen,
Kenneth Dickstein,
Alain Cohen-Solal, et al
55
The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized study controlled
Donald S. Silverberg,
MD, Dov Wexler, MD,
David Sheps, et al
16
Erythropoietin improves anemia exercise tolerance and renal function and reduces B-type natriuretic peptide and hospitalization in patients with heart failure and anemia
Alberto Palazzuoli,
MD, PhD,a Donald
Silverberg, MD,b
Francesca Iovine, MD, et al
18
Effects of darbepoetin
α on right and left ventricular systolic and diastolic function in anemic patients with chronic heart failure secondary to ischemic or idiopathic cardiomyopathy dilated
John T. Parissis, MD,a
Kallirrhoe Kourea,
MD,a Fotios Panou, et al
11
Randomized double-blind trial of darbepoetin alfa in patients with symptomatic heart failure and anemia
Jalal K. Ghali, Inder S.
Anand, William T.
Abraham, et al
157
Effect of darbepoetin- alfa on plasma pro-inflamatory cytokines, anti- inflamatory cytokine interleukin- 10 and solube
Faz/Faz ligand system in anemic patient with chronic heart failure
Kallirrhoe Kourea 1,
John T. Parissis ,
Dimitrios Farmakis, et al
20
Effect of Erythropoietin on
Exercise Capacity in
Patients With Moderate to
Severe Chronic Heart
Failure
Donna M. Mancini,
Stuart D. Katz, Chim
C. Lang,
LaManca, et al
John
8
110
16
20
21
162
21
15
71 ± 9
72.2 ± 9.9
75 ± 6
69 ± 4
69 ± 10
68 ± 13
55 ± 7
71 ± 11
75.3 ± 14.6
72 ± 5
72 ± 5
68 ± 12
72 ± 5
60 ± 12
Mortality,
NYHA walk class, distance, ventricular
Mortality,
NYHA walk ventricular hemoglobin,
6-minute hemoglobin, class, 6-minute distance, left ejection fraction, serum ferritin. left ejection fraction, serum ferritin.
Mortality,
NYHA class, peak VO
Mortality,
NYHA class, 6-minute walk distance, left ventricular fraction. hemoglobin, class, hemoglobin,
2
.
Mortality, NYHA class. left ventricular ejection fraction serum ferritin.
Mortality, exercise duration, NYHA
Mortality, exercise minute peak VO
2
. walk hemoglobin, ejection hemoglobin, duration, 6distance,
Figure 2 Exercise duration
Figure 3 Six-minute walk distance
Figure 4 Left ventricular ejection fraction (LVEF)
Figure 5 Peak Vo
2
Study or Subgroup
A.H. Journal 2006 (4)
A.H. Journal 2008 (5)
A.H. Journal 2008 (6)
ELSEVIER 2007 (7)
JACC 2001 (3)
JACC 2007 (2)
Erythropoietin
Mean SD Total
Placebo
Mean SD Total Weight
2.2
2.1
2.43
2.8
2.2
2.3
0.7
0.5
0.32
0.5
0.7
0.64
20
21
162
21
16
110
3.9
3.2
2.52
2.55
3.9
2.315
0.3
0.6
0.36
0.5
0.3
0.68
18
11
157
20
16
55
16.5%
16.0%
17.5%
16.7%
16.3%
17.1%
Mean Difference
IV, Random, 95% CI
-1.70 [-2.04, -1.36]
-1.10 [-1.51, -0.69]
-0.09 [-0.16, -0.02]
0.25 [-0.06, 0.56]
-1.70 [-2.07, -1.33]
-0.02 [-0.23, 0.20]
Mean Difference
IV, Random, 95% CI
Total (95% CI) 350 277 100.0%
Heterogeneity: Tau² = 0.48; Chi² = 175.90, df = 5 (P < 0.00001); I² = 97%
Test for overall effect: Z = 2.44 (P = 0.01)
-0.71 [-1.28, -0.14]
-2 -1 0 1
Favours experimental Favours control
2
Figure 6 New York Heart Association classification
Figure 7 Mortality
Figure 8 Haemoglobin concentration
Figure 9 Serum Ferritin
DISCUSSION: This is the first meta-analysis to evaluate survival and quality of life related aspects in patients with Heart Failure and anaemia treated with erythropoietin.
We found statistically significant improvements in many aspects associated with quality of life in patients treated with erythropoietin, such as exercise duration, six-minute walk distance, left ventricular ejection fraction (LVEF) and peak Vo
2
.
A significant decrease in NYHA classification in experimental group is a positive subjective consequence which seems to be associated to the treatment. Haemoglobin also improved with erythropoietin administration comparing with the placebo group. Therefore we can conclude that erythropoietin treatment benefices haemoglobin concentration in patients.
The differences found in mortality frequency weren’t statistically significant. So, we conclude that the treatment with erythropoietin does not improve patient’s survival.
Three of the studies included in meta-analysis [14, 15, 18 ] refer rates complication after the treatment and it let us conclude that exist an higher level of safety associated with the treatment.
Another three articles [14, 15, 21] evaluate quality of life trough two type of questionnaire: Kansas
City Cardiomyopathy Questionnaire (KCCQ) and Minnesota Living with Heart Failure Questionnaire
(MLHFQ). The first one was used only in articles [14], where quality of life improved in experimental group and it was statistically significant, and [15] where the improve of quality of life was not statistically significant. The MLHFQ was mentioned in the three articles. The quality of life improved with erythropoietin administration in all of them but only in article [21] it was statistically significant.
The advantages of erythropoietin administration in patients with HF and anaemia are significant, this treatment should, therefore, be considered a serious therapeutic option.
After this analysis we may suggest that should not be done more randomized controlled clinical trial about erythropoietin administration in patients with Chronic Heart Failure because of ethical questions. Studies made until now are enough, so people should not be submitted to this type of treatment if it is not necessary.
Study limitations . Limitation of meta-analysis basically included heterogeneity, absence of full article and differences in data presentation used in the selected articles which difficult data aggregation.
The articles that weren’t available were excluded. In articles with same variables in different units we tried to convert them into the same unit. If it was not possible, the variable was excluded.
Some relevant variables, as B-type Natriuretic Peptide (BNP), an important data to evaluate the efficiency of treatment, rate readmission and safety, were mentioned only in less than three articles, so it wasn’t possible include them into the meta-analysis.
These limitations led to the impossibility of running a meta-analysis with a larger number of variables and analyzing more articles which titles and abstracts indicated them relevant for our study.
During the meta-analysis using meta-analysis software in Review Manager 5
®
the heterogeneity test values were affected because of the restrict number of article values therefore, sometimes, the pvalue allowed us to conclude heterogeneity that did not exist in the graphic interpretation.
REFERENCES
1. Kenneth D., Alain C., et al.
ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008 . Eur. HeartJ. 2008; 29: 2388-2442.
2. Dunlay S., Weston S., et al. Anaemia and heart failure: A community study . Acad Med 2008; 121:
726-732.
3. Vedhuisen D., Dickstein K., et al. Randomized double-blind, placebo- controlled study to evaluate the effect of two dosing regimens of darbepoetin alfa in patients with heart failure and anaemia.
Eur. HeartJ. 2007; 28.
4. Groenveld H., Januzzi J., et al. Anaemia and mortality in heart failure patients - A systematic review and meta-analysis.
J. Am. Coll. Cardiol. 2008; 52: 818-827.
5. Westenbrink B., de Boer R., etal. Anaemia in chronic heart failure: etiology and treatment options .
Curr. Opin. Cardiol. 2008; 23: 141-147.
6. Michael J., Lloyd I., et al. Impact of epoetin alfa on clinical end points in patients with chronic renal failure: A meta-analysis. Kidney International 2004; 65: 757 –76.
7. Crawford J., Recombinant human erythropoietin in cancer-related anaemia. Review of clinical evidence. Oncology 2002;16: 41-53
8. Ghali J., Anand I., et al. Randomized double-blind trial of darbepoetin alfa in patients with symptomatic heart failure and anaemia.
Circulation 2008; 117: 526-535.
9. Silverberg DS, Wexler D, Sheps D, Blum M, Keren G, Baruch R, Schwartz D,Yachnin T,
Steinbruch S, Shapira I, Laniado S, Iaina A. The effect of correction of mild anaemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study.
J Am Coll Cardiol 2001;37:1775
–1780.
10. Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne AS. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure . Circulation
2003;107:294 –299.
11. Palazzuoli A, Silverberg D, Iovine F, Capobianco S, Giannotti G, Calabro A, Campagna MS, Nuti
R. Erythropoietin improves anaemia exercise tolerance and renal function and reduces B-type natriuretic peptide and hospitalization in patients with heart failure and anaemia . Am Heart J
2006;152:1096.e9
–e15.
12. Ponikowski P, Anker SD, Szachniewicz J, Okonko D, Ledwidge M, Zymlinski R, Ryan E,
Wasserman SM, Baker N, Rosser D, Rosen SD, Poole-Wilson PA, Banasiak W, Coats AJS,
McDonald K. Effect of darbepoetin alfa on exercise tolerance in anemic patients with symptomatic chromic heart failure . J Am Coll Cardiol 2007;49:753 –762.
13. Donald S. Silverberg, Dov Wexler, Miriam Blum, Doron Schwartz, Gad Keren, David Sheps and
Adrian Iaina. Effect of Correction of anemia with erythropoietin and intravenous iron in resistant heart failure in octogenarians . IMAJ 2003; 5:337-339
14. Piotr Ponikowski, Stefan D. Anker, Joanna Szachniewicz, Darlington Okonko, Mark Ledwidge,
Robert Zymlinski, Enda Ryan, Scott M. Wasserman, Nigel Baker, Dylan Rosser, Stuart D.Rosen,
Philip A. Poole-wilson, Waldemar Banasiak. Effect of Darbepoietin Alfa on Exercise Tolerance in
Anemic Patients With Symptomatic Chronic Heart Failure . JACC 2007, Vol 49, No 7
15. Dirk J. Van Veldhusien, Kenneth Dickstein, Alain Cohen-Solal, Dirk J.A. Lok, Scott M.
Wassermans, Nigel Baker, Dylan Rosser, John G.F. Cledand, Piotr Ponikowskis. Randomized, double-blind, placebo-controlled study to evaluate the effect os two dosing regimens of darbepoetin alfa in patients with heart failure and anemia . European Heart Journal (2007) 28,
2208 –2216
16. Donald S. Silverberg, Dov Wexler, David Sheps, Miriam Blum, Gad Keren, Ron Baruch, Doron
Schwartz, Tatyana Yachnin, Shoshana Steinbruch, Itzhak Shapira, Sholomo Laniado, Adrian
Iaina. The Effect of Correction of Mild Anemia in Severe, Resistant Congestive Heart Failure Using
Subcutaneous Erythropoietin and Intravenous Iron: A Randomized Controlled Study . JACC 2001,
Vol 37, No 7
17. Alberto Palazzuoli, PhD Donald Silverberg, Francesca Iovine, Stefano Capobianco, Giovanna
Giannoti, Anna Calabro, Maria stella Campagna, Ranuccio Nuti. Erythropoietin improves anemia exercise tolerance and renal function and reduces B-type natriuretic peptide and hospitalization in patients with heart failure and anemia . American Heart Journal, September 2006
18.
John T. Parissis, Kallirrhoe Kourea, Fotios Panou, Dimitrios Farmakis, Ioannis Paraskevaidis,
Ignatios Ikonomidis, Gerasimos Filippatos, Dimitrios Th Kremastinos. Effects of darbepoetin alfa on right and left ventricular systolic and diastolic function in anemic patients with chronic heart failure secondary to ischemic or idiopathic dilated cardiomyopathy . American Heart Journal, April
2008
19. Jalal K. Ghali, Inder S. Anand, William T. Abraham, Gregg C. Fonarow, Barry Greenberg, Henry
Krum, Barry M. Massie, Scott M. Wasserman, Marie-Louise Trotman, Yan Sun, Beat Knusel, Paul
Armstrong. Randomized Double-Blind Trial of Darbepoetin Alfa in Patients With Symptomatic
Heart Failure and Anemia . Circulation 2008;117;526-535
20.
Kallirrhoe Kourea, John T. Parissis, Dimitrios Farmakis, Fotios Panou, Ioannis Paraskevaidis,
Koula Venetsanou, Gerasimos Filippatos, Dimitrios Th. Kremastinos. Effects of darbepoetin-alpha on plasma pro-inflammatory cytokines, anti-inflammatory cytokine interleukin-10 and soluble
Fas/Fas ligand system in anemic patients with chronic heart failure . ELSEVIER, Atherosclerosis 199
(2008) 215 –221
21. Donna M. Mancini, Stuart D. Katz, Chim C. Lang, John LaManca, Alhakam Hudaihed and Ana-
Silvia Androne. Effect of Erythropoietin on Exercise Capacity in Patients With Moderate to Severe
Chronic Heart Failure . Circulation 2003;107;294-299