1
Pharmacotherapeutics for Advanced Nursing Practice 433
Drugs that Act on Smooth Muscles:
Antihistamines, Decongestants, and Bronchodilators
Allergic rhinitis and asthma will be the prototypical disease states used to introduce these agents.
Allergic Rhinitis
Pathophysiology
Sympathetic stimulation causes vasoconstriction, resulting in reduction of tissue size and
airway widening.
Parasympathetic stimulation causes vasodilation and airway narrowing.
The nasal mucosa contains mast cells.
o Mast cells release histamine which increases epithelial permeability.
o This allows allergens to reach the submucosa where there is a high density of
mast cells
o Once a patient is susceptible, allergens react with IgE on these mast cells.
o The release of cytokines from these cells produces local inflammation.
Signs/symptoms commonly seen include: rhinorrhea, sneezing, itching in the nose and
throat, watery eyes
Complications (most common)
Exacerbations of asthma
Acute and chronic sinusitis
Treatment
Antihistamines and decongestants work to alleviate symptoms.
Nasal steroids and nasal cromolyn are also very helpful in reducing symptoms in chronic
patients.
Leukotriene inhibitors used for asthma have also been found to be of benefit for allergy
symptoms.
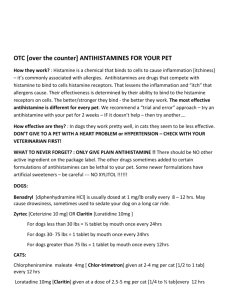
Antihistamines
Note: There are two types of histamine blockers (“antihistamines”): histamine1) H1 blockers are
used for treatment of seasonal allergic rhinitis, anaphylaxis, and insect reactions, whereas
histamine2 (H2) blockers are used in the treatment of gastric acid disorders such as ulcers. The
following discussion relates to histamine1 blockers.
2
Mechanism of action: antagonize the histamine receptor, preventing the action of
histamine.
o All antihistamines work best when given before allergen exposure.
Oral antihistamines are systemic; use especially if the person is experiencing eye
symptoms of allergy along with the nasal symptoms.
The use of antihistamines in allergic rhinitis is effective, but side effects and cost can
limit their use.
o All are equally effective.
o Size effects determine the choice of agent.
Effects of Various Antihistamines
Generic Name
brompheniramine
Brand Name
Anticholinergic
Effects*
Moderate
Sedative
Effects
Low
Moderate
High
High
Low
Moderate
Low to
Moderate
Low to
Moderate
chlorpheniramine
clemastine
diphenhydramine
Dimetane,
Codimal-A
Chlor-Trimeton
Tavist
Benadryl
dimenhydrinate
Dramamine
High
promethazine
hydroxyzine
Phenergan
Atarax, Vistaril
High
Moderate
High
Moderate
loratadine
desloratadine
cetirizine
fexofenadine
Claritin (OTC)
Clarinex
Zyrtec (OTC)
Allegra (OTC)
Low to none
Low to none
Low to none
Low to none
Low to none
Low to none
Low to none
Low to none
*
Comments
Cause less drowsiness and more
CNS stimulation; suitable for
daytime use
Substantial anticholinergic effects;
commonly cause sedation; with
usual doses drowsiness occurs in ~
50% of patients; diphenhydramine
and dimenhydrinate also used as
antiemetics; dimenhydrinate also
used as antivertigo
Also used as antiemetic, antivertigo
Also used as a tranquilizer,
sedative, antipruritic, and
antiemetic
Very few adverse effects from
anticholinergic or sedative effects;
almost exclusively antihistaminic
effects; can take during day
because no sedative effects. In
general they are longer activing and
have fewer side effects
If anticholinergic effects are “high”, high risk of urinary retention, paradoxical excitation.
Antihistamines with “high” anticholinergic effects should be used with caution in patients
with angle-closure glaucoma and prostatic hypertrophy……why?
The sedating agents are less expensive and generally safe, thus it may be worth beginning
therapy with these agents. Caution with elderly and others at risk for falls!
With sedating agents such as chlorpheniramine (Chlor-Trimeton), begin with 1 mg twice
a day (short-acting) and work up over 2-6 weeks to full dose (8-12 mg/day) to prevent
dose limiting side effects such as sedation in patients with significant allergy.
3
Antihistamines: Drug Effects
Cardiovascular system (small blood vessels)
o Histamine effects: Dilation of blood vessels, increased blood vessel permeability
(allows substances to leak into tissues)
o Antihistamine effects: Prevent dilation of blood vessels and increased
permeability
Smooth muscle (on exocrine glands)
o Histamine effects: Stimulates salivary, gastric, lacrimal, and bronchial secretions
o Antihistamine effects: Prevents salivary, gastric, lacrimal, and bronchial
secretions
Immune system (release of various substances commonly associated with allergic
reactions)
o Histamine effects: Mast cells release histamine and several other substances,
resulting in allergic reactions
o Antihistamine effects: Do not stabilize mast cells nor do they prevent the release
of the substances such as histamine, but they bind to histamine receptors and
prevent the actions of histamine.
Drug Interactions
Problem with the early non-sedating antihistamines (terfenadine [Seldane] and astemizole
[Hismanal]):
Metabolized by the liver
Erythromycin, ketoconazole (Nizoral), itraconazole (Sporanox) could inhibit their
metabolism.
In some patients, this could result in toxic concentrations of terfenadine and astemizole,
resulting in arrhythmias from prolongation of the QT interval.
These medications were removed from the market.
So, what pharmacokinetic process was the basis for the potentially fatal drug interaction
described above?
Decongestants
Decongestants are useful for immediate relief of symptoms while waiting for onset of action of
antihistamines and anti-inflammatories.
Local vasoconstriction – topical
Examples: oxymetazoline (Afrin, Dristan, Sinex) and phenylephrine (Neosynephrine)
Duration of therapy: use only when needed for no longer than 3-5 days.
4
o With prolonged therapy, “rhinitis medicamentosa” occurs in virtually all
patients.
o More of the drug is required to produce the same effects.
o Once the drug is stopped, there is rebound congestion (rebound vasodilation)
following the extreme vasoconstriction. Patients will want to use the drug again
to treat this.
o Treatment involves a 2-3 week wean of the topical agent while combining a nasal
anti-inflammatory agent such as cromolyn.
Systemic vasoconstriction – oral
phenylpropanolamine [PPA] (as in Allerest, Contac, Rhinedecon, and Dexatrim): pulled
from market in 2000 due to risk of hemorrhagic stroke, particularly in women.
pseudoephedrine (as in Pediacare, Sudafed): Still available.
o OK for use with hypertensive patients IF HTN is well-controlled, it is used for
only a short time, and the dosage used is the 30 mg, rather than 60 mg.
o Effective January 15, 2006, the Methamphetamine Precursor Control Act
(MPCA) makes pseudoephedrine and ephedrine “schedule V controlled
substances,” meaning they must be kept behind pharmacy counters. It requires
that all medications that contain any amount of pseudoephedrine or ephedrine in
any form be kept behind the pharmacy counter. Customers who want to purchase
these products do not need a prescription but they do need to show a governmentissued identification card, be at least 18 years of age, and sign a log. Customers
purchasing medications containing pseudoephedrine or ephedrine can purchase no
more than two packages, or 6000 milligrams, at a time and no more than 7500
milligrams in a month.
(http://www.illinoisattorneygeneral.gov/methnet/news/edition2/story3.html)
Phenylephrine (Neosynephrine, Sudafed on the shelf): Avoid in HTN patients
o Systemic phenylephrine is an alpha1 agonist…..why would this be a problem in
patients with HTN?
For those with uncontrolled HTN, there is Coricidin HBP, which does not contain a
decongestant….does contains chlorpheniramine (antihistamine)
o Can you think of any other option for patients with HTN?
Combination decongestant/antihistamine therapy – indications
o Useful in patients but usually for a short duration
o In most viral URIs patients do not require an antihistamine; therefore combination
products are generally not recommended after gaining initial control of symptoms
o Works well with patients who have congestion along with an underlying allergy problem
o Examples: Claritin-D, Allegra-D, Zyrtec-D)
5
Intranasal Anti-Inflammatories (Steroids)
o Examples
o cromolyn sodium (Nasalcrom)
1 spray 3-4X/day
o beclomethasone (Beconase AQ)
1-2 sprays 2X/day
o budesonide (Rhinocort Aqua)
1 spray/day (up to 4 sprays/day)
o fluticasone (Flonase, Veramyst)
2 sprays/day (can decrease to 1/day)*
Flonase Allergy Relief available OTC in spring 2015)
o mometasone (Nasonex)
2 sprays/day (can decrease to 1/day)*
o triamcinolone (Nasacort AQ)
2 sprays/day (can decrease to 1/day)*
*
With control of symptoms, can decrease to 1 spray/day.
o Good if patient’s only allergy symptoms are nasal
o All of these agents may be more effective than antihistamines for long term control of
allergic rhinitis.
o They need to be used once the patient is decongested and with clear nasal passages
o The steroids work by stabilizing the epithelial mediator cells and decreasing epithelial
permeability.
o Cromolyn works by stabilizing the mast cells.
o They have little additive effect when used in combination with antihistamines
o Their onset is within a few days to 2 weeks.
o During this time it is useful to use an antihistamine and decongestant if needed.
o NOTE: These can be very drying, which can cause nasal bleeding. Warn patients of
drying effect. Avoid use in nasal trauma.
Intranasal Antihistamine
o Antihistamine for allergic and non-allergic rhinitis (including vasomotor rhinitis)
o Example: azelastine (Astelin) 2 sprays/nostril twice a day
o Good if patient’s only allergy symptoms are nasal
If patient’s symptoms also include watery eyes, will need a systemic medication:
o Oral antihistamine (discussed above)
o Caution with older males: antihistamines can cause urinary retention, especially
in patients with BPH
o Leukotriene inhibitor (Singulair 10 mg daily)
6
Asthma
Types of Asthma
o Allergic
o May be seasonal or non-seasonal
o Most likely cause: allergens (antigens) such as animal dander, dust, and molds
o Idiopathic
o Most likely cause: poorly defined etiologic factors; may be induced by stress,
respiratory infections or strenuous exercise
o Mixed
o Most likely cause: combination of allergens and some of the idiopathic factors
Pharmacologic Treatment Options
o Beta-Agonists (=sympathomimetics)
o Cause relaxation of the smooth muscle that surrounds the airways
o May stimulate alpha and beta receptors, beta1 and beta2 receptors, or just beta1
receptors
o Beta2 stimulants are the most specific for the lungs and have the fewest side
effects
o Examples:
Beta2 agonist: albuterol (ProAir HFA, Proventil HFA, Ventolin HFA);
levalbuterol (Xopenex HFA)
Alpha-beta agonist: epinephrine (Adrenalin, Primatene, Bronkaid)
Long-acting: salmeterol (Serevent) – 2 puffs every 12 hours
Long-acting: formoterol (Foradil Aerolizer) – 12 mcg inhalation every 12
hours (12 mcg/powder cap)
Long-acting: indacaterol (Arcapta Neohaler) 75 mcg/capsule inhaled once
daily
CAUTION: A 2002 study (Salmeterol Multi-center Asthma Research Trial
[SMART] showed a statistically significant greater number of primary events and
asthma-related events, including deaths, in patients taking salmeterol compared to
those taking placebo. This was seen in African Americans enrolled in the study,
but not in Caucasian patients in the study.
Recommendations: National Asthma Education and Prevention Program
(NAEPP) guidelines recommend patients requiring more than as-needed shortacting beta2 agonists should be prescribed regular and adequate doses of an
inhaled anti-inflammatory asthma medication, such as inhaled corticosteroids, for
optimal benefit in the management of their asthma. Consistent with these
7
guidelines and reinforced by trends seen in the interim analysis of the SMART
data, GlaxoSmithKline recommends that patients receiving salmeterol for asthma
should normally also be receiving regular and adequate doses of an effective
asthma controller medication, such as inhaled corticosteroids.
(Source: Safety information released by GSK in 2003)
New as of 2010: The FDA required label changes and other initiatives to
promote safe use of long-acting beta agonist (LABA) agents, noting that these
agents should never be used alone in children or adults with asthma. This
affected the two single-agent LABAs approved for asthma: salmeterol
(Serevent) and formoterol (Foradil). The labels were changed to require that
the drugs always be used in combination with an asthma controller
medication such as an inhaled corticosteroid. (Also applies to newest LABA,
Arcapta)
o Contraindications to use: history of cardiac disease, dysrhythmias, angina, CAD,
HTN, seizure disorders.
o Side effects: tremor, insomnia, restlessness, vascular headache
o Interactions:
o Beta-agonist bronchodilator + nonselective beta-blocker = antagonizes the
bronchodilation
o For patients with diabetes: epinephrine increases blood glucose levels
o
Inhaled Corticosteroids
o Work by stabilizing the membranes of cells that release harmful
bronchoconstricting substances
o Not first-line agents; commonly used when conventional short-acting
bronchodilators fail
o Examples: beclomethasone (Qvar HFA), budesonide (Pulmicort Flexhaler),
ciclesonide (Alvesco), flunisolide (Aerospan HFA), fluticasone (Flovent HFA,
Flovent Diskus), mometasone (Asmanex HFA, Asmanex Twisthaler)
o Inhaled steroids do not suppress HPA axis except at high doses
o
Combination Products
o Examples: fluticasone/salmeterol (Advair Diskus 100/50, 250/50, 500/50),
budesonide/formoterol (Symbicort 80/4.5, 160/4.5), mometasone/formoterol
(Dulera 100/5, 200/5)
o If not currently on a steroid, can start with lower dose (such as Advair 100/50)
o If currently on a steroid, start with higher dose (such as Advair 250/50 or 500/50)
o Taper to lowest effective dose
8
o Anticholinergics
o Work by blocking the bronchoconstrictive effects of acetylcholine
o Used for maintenance and not relief of acute bronchospasm associated with
COPD (chronic bronchitis and emphysema) (** Not asthma)
o Examples of agents
o umeclidinium/vilanterol (Anoro Ellipta)
o ipratropium bromide (Atrovent HFA)
o albuterol/ipratropium (Combivent Respimat)
o tiotropium (Spriva HandiHaler, Spiriva Respimat)
o aclidinium (Tudorza Pressair)
o Indirect-Acting Agents
o Work by stabilizing the mast cell wall, thereby preventing potentially harmful
vasoconstrictive substances from being released
o Only used prophylactically; available in nebulization form
o Example: cromolyn sodium
o Xanthines
o Work by inhibiting phosphodiesterase, which breaks down cAMP, which is
needed to relax smooth muscles
o Examples: caffeine, theophylline
o Theophylline is the most common xanthine used; aminophylline is the parenteral
form of theophylline
o Contraindications to use: history of GI tract disorders or peptic ulcer disease
o Factors affecting theophylline clearance
o Decrease clearance: cimetidine, erythromycin, allopurinol, propranolol,
OCPs, ciprofloxacin, norfloxacin, ofloxacin, febrile viral illness
o Increase clearance: rifampin, carbamazepine, phenobarbital, phenytoin,
smoking, high-protein diet, charcoal broiled meat
o Theophylline half-life:
o Neonates:
20-30 hours
o Child 1-12 years old
3-4 hours
o Nonsmoking adult
7-8 hours
o Smoking adult
4-5 hours
o Elderly
9-10 hours
o Leukotriene Receptor Antagonists
o Used only for long-term control of asthma
o Affect the late phase of the asthmatic response
9
o Block binding of leukotriene D4 to its receptor; alters pathophysiology
associated with inflammatory process that contributes to signs/symptoms
of asthma
o Useful alternative if patients are unable to tolerate the side effects of the
other medications
o May be effective as first-line therapy for patients with mild-to-moderate
asthma when used alone or in combination with beta-agonists used PRN
o May be especially effective in patients with exercise or aspirin-induced
asthma
o Oral administration is useful for patients who have difficulty using
inhalers
o Very low incidence of side effects
o Examples
montelukast (Singulair) – 10 mg once daily in evening
zafirlukast (Accolate) – 20 mg twice daily (take 1 hour before or 2
hours after meals)
zileuton (Zyflo, Zyflo CR) – Zyflo 600 mg 4X/day; Zyflo CR 1200
mg twice daily within 1 hour after morning and evening meals.
Monitor LFTs
o Use of Inhaler
o Only 10-15% of the dose actually gets to the lungs; only 30-45% of patients use
proper technique
o Use of spacer
o Use of non-HFA devices: diskus, respimat, twisthaler, etc.
o How to check if full-empty – floating in water is NOT adequate; need to count
doses, keep a spare!
o Demonstrate/return demonstration
o If using separate bronchodilator and steroid: Use bronchodilator (beta-agonist)
first, wait 2-5 minutes, then use inhaled steroid
o Rinse mouth after using steroid
 0
0