Add your student`s picture here. GSLC Allergy Management Plan
advertisement

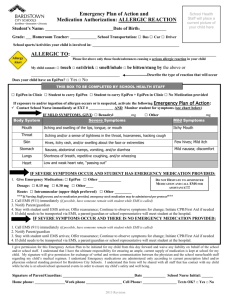
Add your student’s picture here. GSLC Allergy Management Plan 2012-2013 Sunday School Year Name of Student: Age: Is the student asthmatic? Date of Birth: Grade: Yes* No *Higher risk for reaction Please list all Allergies: Symptoms of an allergic reaction in my student may include (please add more symptom detail specific to your student at the end of each symptom): Mouth – itching and swelling of the lips, tongue or mouth. Throat – itching and/or a sense of tightness in the throat, hoarseness, and a hacking cough. Skin – hives, itchy rash, and or swelling about the face or extremities, flushing or paleness of the skin. Gut – nausea, abdominal cramps vomiting, and/or diarrhea. Lung – shortness of breath, repetitive cough, wheezing. Heart – rapid pulse, drop in blood pressure, unconsciousness. Sunday School Management Plan: Avoidance Strategies (Please list all instructions that Sunday School volunteers should know about how to prevent exposure to your child’s allergen. Consider sources contained in food, craft materials and environment.) *Does this student have an antihistamine? Yes Location of antihistamine during Sunday School? On-Child Teacher Parent *Does this student have an Epipen? Yes Location of Epipen during Sunday School? On-child Teacher Parent No No *Please complete the Medication Administration and Emergency Notification sections on Page 2 of this document. To be completed by Sunday School Staff: Reviewed by: ________________ Copy placed in Rm Binder: Y N Date: _______________________ Student listed on Allergy List: Y N ALLERGY TREATMENT PLAN In the event of exposure to an allergen, the following steps should be taken: MEDICATION ADMINISTRATION 1) If a student has been exposed to an allergen, but shows no symptoms, administer: No Medication Epipen* Antihistamine* Other Medication* *If this box is checked, please complete the following information: Name of Medication: Dosage: **If Epipen is administered, call 9-1-1 IMMEDIATELY. 2) If a student has been exposed to an allergen and is showing the signs of an allergic reaction, administer: No Medication Epipen* Antihistamine* Other Medication* *If this box is checked, please complete the following information: Name of Medication: Dosage: **If Epipen is administered, call 9-1-1- IMMEDIATELY. EMERGENCY NOTIFICATION: In the event of allergic exposure, parents/guardians will be contacted by Sunday School volunteer/staff. Parent/Guardian Name: Parent/Guardian Emergency Number(s): Emergency Contact: Emergency Contact Number: Relationship: Student’s Doctor: Doctor’s Phone Number: Parent/Guardian Signature: Date: To be completed by Sunday School Staff: Reviewed by: ________________ Copy placed in Rm Binder: Y N Date: _______________________ Student listed on Allergy List: Y N