Food Allergy Action Plan - Shanghai American School
advertisement

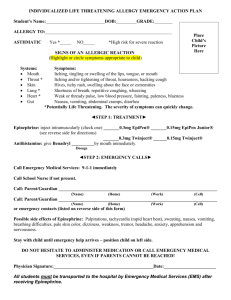
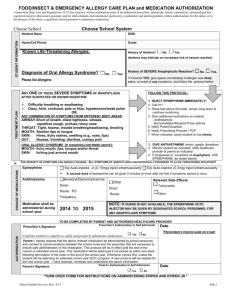
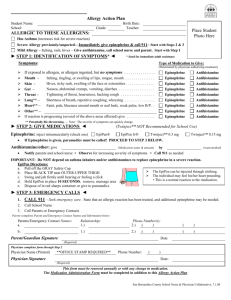
FOOD ALLERGY MANAGEMENT PLAN STUDENT NAME:_____________________________________ D.O.B:_______Class :_________ ALLERGY TO:___________________________________________________________ Asthmatic � Yes* � No *Higher risk for severe reaction STEP 1: IDENTIFY SYMPTOMS Symptoms When Exposed to Allergen: check and / or circle all that apply � Mouth: Itching, tingling, or swelling of lips, tongue, mouth � Skin: Hives, itchy rash, swelling of the face or extremities, itchy or swollen eyes � Gastro-intestinal: Nausea, abdominal cramps, vomiting, diarrhea � Throat: Tightening of throat, hoarseness, hacking cough � Lung: Shortness of breath, repetitive coughing, wheezing � Heart: Thready pulse, low blood pressure, fainting, pale, blueness � Other: __________________________________________________________________________ � If reaction is progressing (several of the above areas affected), the school nurse may give: � Epinephrine and/or � Antihistamine STEP 2: TREATMENT AND EMERGENCY ACTION Medication Given When Allergy Occurs: check and / or circle all that apply � Epinephrine – given intramuscularly: (circle one): EpiPen® EpiPen® Jr. Twinject™ 0.3 mg Twinject™ 0.15 mg � Antihistamine: give _______________________________________________________(medication/dose/route) � Other: give ________________________________________________________(medication/dose/route) *If your child has a history of using an epinephrine injection device for a food allergy, it is strongly recommended to keep an extra EpiPen®, EpiPen® Jr., Twinject™ 0.3 mg, or Twinject™ 0.15 mg in the Nurses Office EpiPen® and EpiPen® Jr. along with Benadryl tablets are labeled and kept in an unlocked, labeled drawer in each School Nurse’s office In addition to the school nurse, the following staff members have been trained in use of the Epipen: School Counselors Health Teachers Team Leaders D:\116091023.doc Page 1 of 2 STEP 2: TREATMENT AND EMERGENCY ACTION (continued) In cases of severe reaction and/or anaphylaxis and if EpiPen® or Twinject™ is used, the student will be taken immediately to an Emergency Healthcare facility. The following lists the actions the School Nurse will take in this situation: 1. Transport student to an Emergency Healthcare facility Hospital/Clinic of Parents choice: ___________________________________________ *If you are unsure where your child should be treated, the school nurse will take your child to the Shanghai United Family Hospital Emergency Room (Puxi campus) or Shanghai East International Medical Center (Pudong campus) 2. Call Parents 3. Call Emergency contacts if unable to reach parents 4. School Nurse will remain with student until parents/guardian/emergency contact are present at the Emergency Healthcare Facility and have been given an update on the child’s treatment I give my permission for the School Nurse to administer Epinephrine or an antihistamine to my child in case of severe and/or anaphylactic allergic reaction. I understand that after the medication has been administered the School Nurse will immediately take my child to the designated Emergency Healthcare facility and notify me of the situation. Parent/Guardian Signature: _______________________ Date_____________ For children with multiple food allergies, consider providing separate Management Plans for different foods. **Medication checklist adapted from the Authorization of Emergency Treatment form developed by the Mount Sinai School of Medicine. Used with permission. Please Return to School Nurse