Allergy / Anaphylaxis Care Plan
advertisement

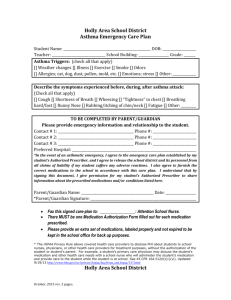
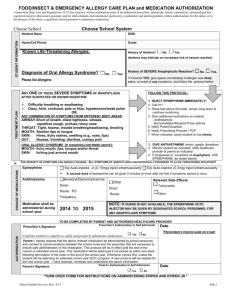
Holly Area School District Allergy/Anaphylaxis Care Plan Student Name: ____________________________________________________ DOB: ___________________ Teacher: _______________________________________ School Building: ___________________________ ALLERGY: (Check appropriate box and list specific allergen) [] Foods: ___________________________________________________________________________________________ [] Latex: [] Type I; anaphylaxis [] Type IV; contact dermatitis [] Stinging insects: _______________________________________________________________________________ [] Other: ___________________________________________________________________________________________ *HISTORY OF ASTHMA: [] YES [] NO (If yes, higher risk for severe reaction) TO BE COMPLETED BY PHYSICIAN OR AUTHORIZED PRESCRIBER [] IF ALLERGEN IS INGESTED, GIVE EPI-PEN IMMEDIATELY AND CALL 911 For Minor Reactions Symptoms: ____________________________________________________________________________________________ Give Antihistamine: [] Diphenhydramine (Benadryl) [] Other: ___________________________________ Dose: _____________ [] Liquid [] Fast-melt [] Tablet [] Other: _____________Route: _________________ Contact the parent/guardian. Stay with student to observe for more serious symptoms. Be prepared to give Epi-Pen. *Any student suspected to have been exposed to the known allergen(s) listed above, requiring Benadryl and/or having a minor reaction, should not participate in any physical activity for a minimum of 2 hours after exposure occurs. This includes but is not limited to; gym, recess, sports. For Major Reactions Symptoms: ____________________________________________________________________________________________ Give Epinephrine: Dose: ____________ Route: ___________ Give Epinephrine immediately (Press hard against outer thigh, through clothing if necessary until click. Hold in place for 10 seconds) CALL 911 immediately. (Always call 911 when Epinephrine is given) Contact parent/guardian. School personnel should accompany student to the hospital if no parent/guardian available. If symptoms worsen, prepare to do CPR [] This medication must be carried on the student’s person at all times. [] This medication must accompany student on the bus. [] This medication must accompany student for school related extracurricular events such as field trips, sports, clubs, etc. The student is both capable and responsible for self-administering of this medication: [] Yes, supervised [] Yes, unsupervised [] No Prescriber’s Name & Credentials: __________________________________________Date: __________________ *Prescriber’s Signature: _________________________________________ Phone #: _________________________ Rev. October, 2015 Holly Area School District Allergy/Anaphylaxis Care Plan Student Name: ____________________________________________________ DOB: ___________________ Teacher: _______________________________________ School Building: ___________________________ SYMPTOMS OF AN ALLERGIC REACTION THAT CAN PROGESS AND BECOME LIFE THREATENING REQUIRING IMMEDIATE USE OF EPI-PEN: Itching and hives spreading over the face and body. Wheezing, difficulty swallowing/shortness of breathe. Swelling, itching, or tingling of face, tongue, lips, or neck. Vomiting or abdominal pain SIGNS OF SHOCK: EXTREME PALENESS, CLAMMY SKIN, FEAR, APPREHENSION, FATIGUE, CHILLS, LOSS OF CONSCIOUSNESS TO BE COMPLETED BY PARENT/GUARDIAN Please provide emergency information and relationship to the student. Contact # 1: _____________________________________________ Phone #: __________________________ Contact # 2: _____________________________________________ Phone #: __________________________ Contact # 3: _____________________________________________ Phone #: __________________________ Preferred Hospital: __________________________________________________________________________ *In the event of an allergic/anaphylactic reaction, I agree to the emergency care plan established by my child’s Authorized Prescriber, and I agree to release the school district and its personnel from all claims of liability if my child suffers any adverse reactions. I also agree to furnish the correct medications to the school in accordance with this care plan. I understand that by signing this document, I give permission for my child’s Authorized Prescriber to share information about the prescribed medications and/or allergic conditions listed here. Parent/Guardian Name: ___________________________________________ Date: __________________ *Parent/Guardian Signature: _______________________________________________________________ Fax this signed care-plan to: ______________________: Attention School Nurse. There MUST be one Medication Authorization Form filled out for each medication prescribed. Please provide an extra set of medications, labeled properly and not expired; to be kept in the school office for back up purposes. * The HIPAA Privacy Rule allows covered health care providers to disclose PHI about students to school nurses, physicians, or other health care providers for treatment purposes, without the authorization of the student or student’s parent. For example, a student’s primary care physician may discuss the student’s medication and other health care needs with a school nurse who will administer the student’s medication and provide care to the student while the student is at school. See 45 CFR 164.512(b)(1)(vi). Updated 9/19/13 http://www.hhs.gov/ocr/privacy/hipaa/faq/ferpa_and_hipaa/517.html Rev. October, 2015