PERI-IMPLANT DISEASE, A GROWING PROBLEM Dr Reena Wadia
advertisement

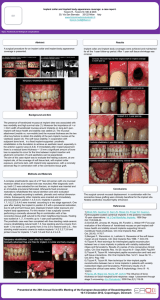
PERI-IMPLANT DISEASE, A GROWING PROBLEM Dr Reena Wadia BDS Hons (Lon), MJDF RCS (Eng) Associate at Pure Periodontics, London Specialist Registrar in Periodontology, Guy’s Hospital, London Dr Neesha Patel BSc Hon (Can), BDS (Glasg), MFGDP (UK), MClinDent Periodontics (Lon), MRD RCS (Ed) Practice Principle at Pure Periodontics Specialist in Periodontics Consultant Periodontist, Kings College Hospital, London INTRODUCTION In 1977, Brånemark et al published an article entitled ‘Osseointegrated implants in the treatment of the edentulous jaw; experience from a 10-year period’1. This study revolutionised clinical dentistry by demonstrating that it was possible to successfully use titanium implants to replace missing teeth. Implant-retained prostheses have since become a popular treatment modality, aiming to fulfil functional and aesthetic needs. As dental practitioners, we are constantly bombarded with updates about the latest dental implants, new techniques and expanded indications. However, the complications that may arise with implant rehabilitation are less commonly advertised and understood. Peri-implant disease is unarguably one of the most significant risks associated with implants. It is a multifactorial disease, which if not diagnosed at early stage, can ultimately lead to failure of the implant. As more and more implants are placed by clinicians of varying skill levels and clinical backgrounds, the numbers of patients presenting with the disease appears to be on the rise. WHAT IS PERI-IMPLANT DISEASE? Peri-implant disease is a condition that affects the tissues surrounding a functional implant; it includes both peri-implant mucositis and peri-implantitis. Peri-implant mucositis can be defined as ‘reversible inflammatory reactions in the soft tissues surrounding a functioning implant’2. Periimplantitis is characterised by ‘inflammatory reactions with loss of supporting bone in the tissues surrounding a functioning implant’3. Peri-implantitis yields many features in common with chronic periodontitis4. Both involve alveolar bone loss. However, there is a zone of connective tissues which is attached to the root surface in periodontitis. In contrast, connective tissue does not attach directly onto implants and there is no periodontal ligament. Therefore, the inflammatory lesion in peri-implantitis extends closer to the bone surface, which can be associated with a faster rate of progression and more aggressive consequences (Figure 1). Figure 1- Periodontitis (left) versus peri-implantitis (right)5 The prevalence of peri-implant disease is significant with peri-implant mucositis affecting up to 80% of implant patients and peri-implantitis affecting 25% of patients.6 AETIOLOGY AND RISK FACTORS Bacterial infections play the most important role in the failure of dental implants. Bacterial flora that are associated with periodontitis and peri-implantitis are found to be similar.7 Studies have shown that the bacteria at the failing implant site consists of gram-negative anaerobic bacteria, such as Porphyromonas gingivalis, Prevotella intermedia and Actinobacillus actinomycetemcomitans.8 The correlation between the presence of periodontitis and the development of peri–implantitis has been supported by a recent systematic review 9,10. Implants in partially dentate patients appear to be at a greater risk of peri-implantitis than implants in fully edentulous patients. There is a marked quantitative decrease in the number of periodontal pathogens around the implants in completely edentulous patients. It is possible that the natural teeth serve as reservoirs for periodontal pathogens from which colonisation of the implant sites occurs11. Other patient-related risk factors include: inadequate oral hygiene, smoking, parafunctional habits and underlying systemic conditions such diabetes. Biomechanical factors, such as an occlusal overload, may play an important role implant failure by resulting in progressive bone loss around the implant. The implants that suffer from traumatic failure have subgingival microflora representing a state of periodontal health12. Iatrogenic factors such as lack of primary stability, poorly positioned implants, premature loading during the healing period and poorly fitting abutments or restorations also appear to increase the likelihood of peri-implant disease.13,14 DIAGNOSIS Early diagnosis and treatment is often the key to complete resolution of the problem. However, although advanced cases of disease will be clearly identifiable, it is often a great challenge to diagnose early disease successfully. Diagnosis of peri-implant disease relies on crude parameters commonly used for the diagnosis of periodontal disease. Swelling and redness of the peri-implant marginal tissues and plaque/calculus accumulation are important signs of peri-implant disease (Figure 2). Figure 2- Inflammation of peri-implant tissues15 Probing the peri-implant sulcus with a blunt, straight, plastic or metal periodontal probe, allows the assessment of: peri-implant probing depth, bleeding on probing and suppuration from the peri-implant space. Studies have shown that successful implants generally allow a probe penetration of approximately 3-4mm in the peri-implant sulcus. Bleeding on probing and suppuration are clear indications of disease (Figure 3).15 Adequate baseline radiographs determine the peri-implant bone status as well as the marginal bone level. These can then be compared to future radiographs to determine if additional bone loss, beyond ‘normal’ has occurred. Progressive bone loss is a definite indicator of periimplantitis (Figure 3), but it should not be confused with physiological bone remodelling around the implant during the first year of function16. Implant mobility is an insensitive measure in detecting early implant failure. More advanced peri-implantitis is characterised by mobility of the fixture, indicating failure of osseo-integration. Figure 2- Bleeding on gentle probing5 Figure 3- Evidence of ‘saucer shaped’ bone loss around implant5 MANAGEMENT Comprehensive treatment of peri-implant disease remains an enigma to most dentists but is largely dependent on the underlying aetiology at play. When the main aetiological factor is bacterial infection, the first phase of treatment involves the control of acute infection and the reduction of inflammation. This involves the removal of plaque deposits and improved patient compliance with oral hygiene until a healthy periimplant site is established. This may be sufficient to re-establish gingival health. The implants that are affected with peri-implantitis are contaminated with soft tissue cells, microorganisms and microbial by-products. The defect must be debrided. Prophy jet and the use of a high pressure air powder abrasive has been advocated, as this removes the microbial deposits, does not alter the surface topography and has no adverse effect on cell adhesion. Various chemotherapeutic agents, such as contact with a supersaturated solution of citric acid have been used for the preparation of the implant surfaces. Soft tissue laser irradiation has also been used17. Additionally, the systemic administration of antibiotics that specifically target gram-negative anaerobic organisms has shown an alteration in the microbial composition and a sustained clinical improvement18. A local delivery device with fibers containing polymeric tetracycline has been tried and this resulted in significantly lower total anaerobic counts19. The type of osseous defects should be identified before deciding on the surgical treatment modality. If vertical 1 to 2-wall defects (< 3mm) are found, then the resective surgery may be used to reduce the pockets, to smoothen the rough implant surfaces, to correct the osseous architecture and to increase the area of the keratinized gingiva20. To arrest the progression of the disease and achieve a maintainable site for the patient, surfaces with threads may be indicated for alteration with high-speed diamond burs and polishers to produce a smooth continuous surface21. Various bone grafting techniques and materials and guided bone regeneration (Figure 4), have been successfully used for the regeneration in 3-wall or circumferential defects. Porous titanium granules have also recently been advocated to try and treat advanced peri-implant osseous defects. Figure 4- Peri-implant bone defect (left) and use of regeneration (right)23 When biochemical forces are considered as the main aetiological factors, occlusal equilibration i.e. improvement of the implant number and position and changes in the prosthetic design, can arrest progression. Long-term success of any peri-implant treatment strategy requires a strict maintenance programme at regular intervals. CONCLUSION Given the large number of implant placements each day around the world, a high prevalence of peri-implantitis can be anticipated, which underlines the necessity for a predictable therapy. Assiduous research is still required for the treatment of peri-implantitis, because there is still no standard protocol for its management. REFERENCES 1- Branemark PI, Hansson BO, Adell R, Breine U, Lindstrom J, Hallen O et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10 year period. Scand J Plast Reconstr Surg Suppl 1977;16:1-132 2- Albrektsson, T. & Isidor, F. (1994) Consensus report of session IV. In: Lang, N.P. & Karring, T., eds. Proceedings of the 1st European Workshop on Periodontology pp 365-369. Berlin: Quintessence. 3- Lindhe L, Meyle J. Peri–implant diseases: consensus report of the sixth European Workshop on Periodontology. J Clin Periodontol 2008; 35 (Suppl. 8): 282–285. 4- Mombelli, A., van Oosten, M. A., Schurch, E., Jr. & Land, N. P. (1987). The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol 2, 145-151. 5- Ho C, Tang T. Failing implants, maintenance and recall. Australasian Dental Practice January/February 2011; 138-146. 6- Zitzmann, N. U. & Berglundh, T. (2008). Definition and prevalence of peri-implant diseases. J Clin Periodontol 35 Suppl 8, 286-291. 7- Hydenrjik K, Majjer JA. Microbiota around root-form endosseous implants: A review. The Int J of Oral and Maxillofacial Implants. Nov/Dec 2002, Vol 17(6). 8- Mombelli A and Long NP. The diagnosis and treatment of Peri-implantitis. Periodontal 2000. 1998; 17: 6376. 9- Kotsovilis S, Karoussis IK, Trianti M, Fourmousis I. Therapy of peri–implantitis: a systematic review. J Clin Periodontol 2008; 35: 621–629. 10- Renvert S, Persson GR. Periodontitis as a potential risk factor for peri–implantitis. J Clin Periodontol 2009; 36 (Suppl. 10): 9–14. 11- Aspe P, Allen RP et al. Microbiota and crevicular fluid collagenase activity in the osseo integrated dental implant sulcus: a comparison of sites in edentulous and partially edentulous patients. J Perio Res 1989; 24: 96-105. 12- Mombelli A, Mericske-sterm R. Microbiological features of stable osseointegrated implants used as abutments for over denture. Clin Imp Res 1990; 1: 1-7. 13- Quirynen M, Van Der Mei HC, Bollen CML, Schotte A, Marechal M, Doornbusch GI et al. An in vivo study of the influence of the surface roughness of implants in microbiology of supra- and subgingival plaque. J Dent Res 1993; 72(9):1304-1309. 14- Lang NP, Bosshardt DD, Lulic M (2011) Do mucositis lesions around implants differ from gingivitis lesions around teeth? Journal of Clinical Periodontology 38 (Suppl. 1), 182–187. 15- Gupta HK et al. Peri-implantitis: A risk factor in implant failure. Journal of Clinical and Diagnostic Research. 2011 Feb, Vol-5(1):138-141. 16- Alberktsson T et al. The long term efficacy of currently used dental implants. A review and proposed criterion of success. Int J Oral Maxillofac Implants 1986; 1: 11-25. Meffert RM. Treatment of ailing and failing implants. J Cliff Dent Assoc 1992; 3: 162. 17- Deppi H et al. Peri-implant care of ailing implants with Co2 laser. Int J Oral Maxillofac Implants 2001; 16; 659-667 18- Roos-Jansaker C et al. Treatment of Perio-implant infections. A literature review. J Clin Periodontol 2003; 30: 467-485. 19- Mombelli A et al. Treatment of Peri-implantitis by local delivery of tetracycline. Clinical, microbiological and radiological results. Clin Oral Implant Res 2001; 12: 287-294 20- Jovanoic SA. The management of peri-implant breakdown around functioning osseointegrated dental implants. J Periodontol 1993; 64: 1176. 21- Jovanoic SA, Spickermann H and Richter EJ. Bone regeneration on titanium dental implants with dehisced defect sites. A clinical study. Int J Oral Maxillofac Implants 1992; 7: 233. 22- Newman HG, Takei HH, Carranza. Clinical Periodontology, 9th Edition,1987 p. 936-940. 23- GBR Image [online]. Available at: http://www.drpattychou.com.au/casestudies/guided-boneregeneration-case/ (accessed 28/04/13).