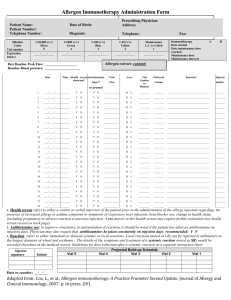
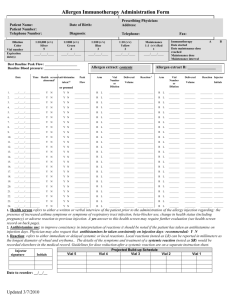
Immunotherapy Vaccine Administration Form
advertisement

Prescribing Physician: Address: Patient Name: Date of Birth: Patient Number: Telephone Number: Diagnosis: Call to reorder when next to last AI given. Fax this form to FAX number. This will be required before any new extract can be prepared. Best Baseline Peak Flow: ___________________ Baseline Blood Pressure: ___________________ Dilution Color Telephone: Phone: Fax: E-mail: Immunotherapy Vaccine Administration Form 1:1,000,000 Peach #7 1:100,000 Pink #6 1:10,000 (v/v) Silver #5 1:1000 (v/v) Green #4 1:100 (v/v) Blue #3 1:10 (v/v) Yellow #2 Maintenance 1:1 (v/v) Red #1 Vial D Expiration date(s) ____/____/___ ____/___/__ ____/____/___ ____/____/___ ____/____/___ ____/____/____ ____/____/___ Vial E Expiration date (s) ____/____/___ ____/___/__ ____/____/___ ____/____/___ ____/____/___ ____/____/____ ____/____/___ Vial F Expiration date (s) ____/____/___ ____/___/__ ____/____/___ ____/____/___ ____/____/___ ____/____/____ ____/____/___ Vaccine content Abbreviations* Tree: T Mold: M Grass: G Cat: C Weed: W Dog: D Ragweed: R Cockroach: Cr Mixture: Mx Dust Mite: Dm Allergy E prepared:_________ Made by:_________ Left office: ________ Total Units: _______ INJECTION INTERVAL IS EVERY_________DAYS _________WEEKS VIAL D: Date Time Health AntiPeak Flow screen histamine 2 abnorm taken? Pre Post al1 Arm Vial E: Vial Dilution Delivered Volume Reaction 3 Vial F: Arm Delivered Volume 3 Reaction Arm Vial Dilution Delivered Reaction3 Volume Injector Initials Vial Dilution 1. ____/____/____ _______ Y N Y N ____________ ____________ ________ ____________ ________ ________ ____________ L L ________ ____________ _______ ________ R R ________ Y N L L ________ N R R ________ Y L L ________ _______ R R ________ 2. ____/____/____ ________ ________ ____________ _______ 3. ____/____/____ _______ Y N Y N R L ________ ________ ____________ R L ________ ________ ____________ R L ________ ________ ____________ _______ 4. ____/____/____ _______ Y N Y N R L ________ ________ ____________ R L ________ ________ ____________ R L ________ ________ ____________ _______ 5. ____/____/____ _______ Y N Y N R L ________ ________ ____________ R L ________ ________ ____________ R L ________ ________ ____________ _______ 6. ____/____/____ _______ Y N Y N R L ________ ________ ____________ R L ________ ________ ____________ R L ________ 7. ____/____/____ _______ Y N Y N R L ________ ________ ____________ R L ________ ________ ____________ R L ________ 8. ____/____/____ _______ Y N Y N R L ________ ________ ____________ R L ________ ________ ____________ R L ________ ________ ____________ _______ ________ _______ ____________ ________ ____________ _______ L ________ ________ ____________ R L ________ ________ ____________ R L ________ ________ ____________ _______ L ________ ________ ____________ R L ________ ________ ____________ R L ________ ________ ____________ 9. ____/____/____ _______ Y N Y N R 10. ____/____/____ _______ Y N Y N R 1. Health screen refers to either a written or verbal interview of the patient prior to the administration of the allergy injection regarding: the presence of increased allergy or asthma symptoms or symptoms of respiratory tract infection, beta-blocker use, change in health status (including pregnancy) or adverse reaction to previous injection. A yes answer to this health screen may require further evaluation (see health screen record on back page). 2. Antihistamine use: to improve consistency in interpretation of reactions it should be noted if the patient has taken an antihistamine on injection days. Physician may also request that antihistamines be taken consistently on injection days: recommended: Y N Vial D ( # vials sent = _____) Conc Color Volume Projected Build-up Schedule Vial E ( # vials sent = _____) Conc Color Volume Vial F ( # vials sent = _____) Conc Color Volume 3. Reaction: refers to either immediate or delayed systemic or local reactions. Local reactions (noted as LR) can be reported in millimeters as the longest diameter of wheal and erythema.. The details of the symptoms and treatment of a systemic reaction (noted as SR) would be recorded elsewhere in the medical record. Injector signature Initials Days since last AI ≤ 1 ½ x interval: continue to increase ≤ 2 x interval: repeat previous dose ≤ 3x interval: reduce by 25% ≤ 4x interval: reduce by 50% > 4x interval: see Dr. Wallace (See enclosed sheet for examples) Locals >2.5 cm + last 24 hours: repeat dose >6 cm, go back one dose