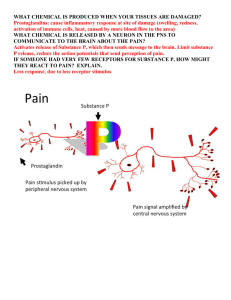
Leukotrienes, Gout and NSAIDs
advertisement

Class: Fundamentals II Professor: Pillion Date: 12/03/10 1 Scribe: Ashley Russell Proof: Louisa Warren Drug Targets and Classes Lecture: XLII. 2nd generation Antihistamines: [S42] a. you will need to know chemical names for test purposes; we won’t use brand names at all. Once in a while, if the brand name is common I’ll add it along with the chemical name to give you a clue. But need to know chemical names!! b. 2nd generation antihistamines are rapidly absorbed, have a long duration of action. They were designed to be a once a day drug. (Most common are once a day versions of the drug) c. They are designed to be given orally. d. They don’t get in to the brain, don’t cause much sedation. e. The first ones to come out were metabolized by the cytochrome P450 system o P450: a family of enzymes found in the liver. They will add and remove oxygen, oxidize and reduce. They basically take care of a lot of drug metabolic drug processes. o If you have a patient who is taking one of these antihistamines chronically, and you give them a new drug (i.e an antibiotic to prevent oral infection). What can happen, is that both of these drugs will get metabolized by the same cytochrome. So, the metabolism of one drug can affect the metabolism of the second drug. The net effect might be that you end up outside the effective dose range for one or both drugs so you need to adjust the dose. When you give a new antibiotic, you need to check out that drugs metabolic profile and know which cytochrome P450 breaks it down. o 95% of the drugs you give to people give inactivated by the cytochromes. o 5% of drugs are pro-drugs and will get activated by CYP450. o Is important to know if drugs are activated or broken down by the cytochromes and knowing which other drugs a person might be taking that would go through the same metabolic pathway. XLIII. Second Generation Antihistamines: [S43] a. The most common ones are cetirizine, loratadine and fexofenadine. o Fexofenadine came out first and has to be given twice a day. Is probably the least popular. o Cetirizine and Loratadine are given once a day, are more popular and are pretty effective as antihistamines. XLIV: Ocular Topical Antihistamines: [S44] a. There are ocular version of antihistamines: olopatadine and levocabastine. b. If you use these, you will “get the red out” if you will; are going to counteract the effect of histamine, which causes vasodialation, tearing and redness of the eyes. c. There are side effects associated with these drugs as well (See slide!) XLV: Allergic Conjunctaivitis: [S45] a. Allergic conjunctivitis can be treated with some of these antihistamines. They can also be treated with mast cell stabilizers, which block the release of histamine or with a drug that binds the binding of histamine. XLVI: Nasal Topical Antihistamines: [S46] a. Fluticasone is used a lot and Flonase is a popular brand (you don’t need a prescription for it) b. Fluticasone is used in the treatment of asthma and to prevent the onset of an asthma attack. Class: Fundamentals II Professor: Pillion Date: 12/03/10 2 Scribe: Ashley Russell Proof: Louisa Warren XLVII: REVIEW [S47] a. Which of the following drugs is least likely to cause sedation? a. All four of these drugs are antihistamines. b. On another test question, might see one of these drugs and have to ID which is an antihistamine. XLVIII: REVIEW [S48] a. Answer: Cetirizine. a. A second generation drug and its given orally once a day and doesn’t cause sedation. XLIV: REVIEW [S49] Which of the following mediators causes immediate symptoms after IgE is cross-linked by allergens? a. To give you a clue, those allergens are usually found on the IgE surface receptors which are found on mast cells. L: REVIEW [S50] ANSWER: Histamine LI: REVIEW [51] Which of the following is not a systemic effect of histamine? a. What do you associate with histamine? Do you associate gastric acid secretion? YES. The antihistamine drugs that block gastric secretions block H2 receptors. H2 receptors are present in the gastric secretion. b. Constriction of small blood vessels? Usually they dilate. c. Bronchoconstriction? Yes d. Formation of Edema? Yes. LII: REVIEW [52] ANSWER: Constriction of small blood vessels. SWITCH LECTURES: Leukotrienes, NSAIDs and Gout (12.03.10) I. Leukotrienes, NSAIDs and Gout (INTRO) [S1] a. We will spend more time talking about the NSAIDs because you don’t see as much gout in your practices. Occasionally we have patients with gout who are taking a specific therapy (NSAIDs) b. NSAID: non-steroidal anti-inflammatory drug i. These drugs are not steroids. ii. There are inflammatory drugs that ARE steroids. To inhibit inflammation can use a steroid or non-steroid. Sometimes one is better than the other. II. Overview [S2] a. Read slide b. Acetaminophen doesn’t really fit under the umbrella of an NSAID, but it is an antifever and anti-pain drug so its usually included in the discussion of NSAIDs because they are used as anti-fever and anti-pain drugs as well as anti-inflammatory drugs. III. Inflammation S3] a. what is inflammation? i. A dynamic vascular and cellular response to insult or injury ii. Your body gets some sort of insult and then responds to it. b. A hangover is not inflammation, but if you bang your knee into the door and it turns red, im seeing inflammation. c. Runners knee from 30 years of running is inflammation. Class: Fundamentals II Professor: Pillion Date: 12/03/10 3 Scribe: Ashley Russell Proof: Louisa Warren IV. Inflammation [S4] a. Can be caused by microorganisms, toxins, biochemical damage, heat cold, radiation, trauma, immunologic hypersensitivity. b. So, a lot of different things can trigger an inflammatory response. c. Usually this response is good because it tells our brain that our body has been injured. d. Anti-inflammatory drugs relieve the symptoms of inflammation, recognizing that sometimes this response isn’t good. (Some people argue inflammation is necessary and appropriate for healing to take place) V. INFLAMMATION [S5] a. Read slide VI. Sequence of Events in Inflammation [S6] a. A table of the events that go on: i. Change in blood flow ii. Permeability change iii. Hemostasis (or blood movement) is reduced and as a result you get swelling, pain, redness, loss of function. b. Read slide. VII. Mediators of Inflammation [S7] a. All of the drugs have their basis on interacting with the biochemistry. b. Normally, our cell membranes contain phospholipids (the bilayer) with a three carbon backbone called glycerol. i. two fatty acids attached in the first two positions and a phosphate attached in the third position. The phosphate has something else added to it (inositol, choline, etc.) ii. Usually, the fatty acid in the number 2 position is arachidonic acid. iii. Arachidonic acid is very “special”. It has 20 amino acids and 4 double bonds which makes it very floppy. It sits in the membrane as a precursor, waiting to be released. 1. Phospholipase A2 releases arachidonic acid 2. The enzyme that releases inositol triphosphate from phosphotidal inosital is a different phospholipase (phospholipase C). This enzyme is activated by some of are adrenergic and cholinergic pathways. iv. Phospholipase A2 cleaves off the free fatty acid, arachidonic acid and then inside our cells we have lipoxygenase and cyclo-oxygenase 1 and 2. 1. we usually think of Cox 1 as being constituative (i.e its on at all times) and cox 2 is inducible (gets ramped up at time of inflammation). 2. As a result of making more cox 2, you get more of the products that are a part of the inflammatory process. This has some implications in drugs that inhibit different enzymes. v. If any of the three enzymes are blocked completely, some bad stuff can happen. If you block one side of the pathway (either lipoxygenase or cox 1 and 2), you will have more “stuff” going to the other side of the pathway which will create an imbalance (can lead to toxicitiy) vi. NSAIDs primarily work by affecting cox 1 and 2 side of the pathway. c. 12:27 VIII. The Arachidonic Acid Cascade [S8] a. A cartoon that shows a phospholipid bilayer membrane. Phospholipase A2 cleaves off this arachidonic acid. b. Beacause arachidonic acid has 4 double bonds, it doesn’t lay flat in a long straight line (will flop over on itself). i. So, two types of enzymes can interact with it (one will form a ring structure and the other wont) Class: Fundamentals II Professor: Pillion Date: 12/03/10 4 Scribe: Ashley Russell Proof: Louisa Warren ii. The name “cyclooxygenase” means that you form a cyclized compound. This is what prostoglandans are made of. 1. Ex: prostacyclin, PGE2, PGD2, PGF2, Thromboxane A and Thromboxane B. 2. Each one is a different chemical derivative with different actions at different sites in the body. But, lots of different cells will interact with many different ones at the same time. c. Lipoxygenase will give you an intermediate called “ETYA”, then you go down this path and form leukotriene A which gets converted to leukotriene B, C, D and E. IX. Picture (NO TITLE) [S9] a. A better cartoon b. At the top left is a cell. i. Outer and nuclear membrane. 1. (Nucleus is purple, cytosol is in green and outside the cell is in yellow) c. In this picture, the site of action of Phospholipase A2 and the release of arachidonic acid is the nuclear membrane. i. The arachidonic acid gets acted upon by liooxygenase and produces luekotriene A4. 1. Leukotriene A4 gets converted to LC4 and LB4 2. These are fatty acid derivatives (lipid soluable) and can leave the cell, go in the blood stream and look for cells with receptors to these chemicals. d. The cell at the top right is in the blood stream and interacts with the leukotriene and chemotaxis takes place as a result of the leukotrieneB binding on that cell. This cell will change its outer shape and will interact with other cells causing a cascade of cells in the blood stream e. The airway cell in the bottom right corner has a receptor for a different leukotriene. (either C, D or E). All of these are formed in the blood stream and can react with this receptor. This is a leukotriene 1 receptor and causes smooth muscle constriction. 1. In an airway cell, you would actually have bronchoconstriction as a result. Bronchoconstriction is one part of inflammation that we don’t want. f. Two families of drugs you need to know about. i. Zileuton: inactivates 5-lipoxygenase. So if you give somebody zileuton, they won’t make leukotriene A4 (or any of the others). So, it’s a pretty good drug. Can also have side effects. Leukotrienes have beneficial effects in certain parts of the body so we’re shutting down both the good and the bad (it’s like “throwing out the baby with the bathwater”). 1. Side effects: increases the movement of chemicals through the other side of the pathway (the cyclooygenase pathway) ii. Monteleukast, Pranleukast and Zafirleukast: these drugs interact at the level of the receptor. Look like leukotrienes, and interact and block binding of leukotrieins to the receptor. They work in a different way from zileuton. 1. These don’t interfere with Leukotriene production, but interfere with leukotriene binding. 2. This gives you more leeway; and allows you to design drugs for specific receptors that will affect specific parts of the body. iii. Example test question: 1. “Which drug is a lipoxygenase inhibitor and which drug is a receptor blocker?” a. zileuton is the lioxygenase inhibitor and the leukasts are the receptor blockers. X. Actions of LTC4 (LTD4, LTE4) [S10] a. Actions of LTC4: i. Late onset, causes bronchoconstriction, increased vascular permeability so you get edma, arteriolar constriction XI. Leukotriene Antagonists [S11] Class: Fundamentals II Professor: Pillion Date: 12/03/10 5 Scribe: Ashley Russell Proof: Louisa Warren a. Zileuton: i. Read slide ii. 600 mg 4 times a day. iii. Will interact with warfarin. If you put them on this drug, can have a disastrous interaction between the two drugs. iv. Many patients who have a heart attack or valve replacement surgery get placed on long term warfarin therapy. Zileuton (among others) can cause their metabolism to change. 1. If a person is on an anti-coagulant and that level gets too high, that person can have a bleed that wont stop. Can have an intercerebral bleed and die. Or, if levels get too low, can have a thrombis form and cause an embolism. (don’t want warfarin levels to get too high or too low!) XII. Leukotriene Antagonists (part 2) [S12] a. Read slide b. Zafirlukast: given twice a day. Not as popular as some others. Can also interact with warfarin and cause liver damage. XIII. Leukotriene Antagonists (part 3) [S13] a. Read slide b. Montelukast: is given once a day (most popular). XIV. ARS Question [S14] a. Which of the following drugs inhibits 5-lopoxygenase? XV. Which of the following drugs inhibits 5-lipoxygenase? [S15] a. ANSWER: Zileuton. XVI. Nonsteroidal Anti-inflammatory Drugs (NSAIDS) [S16] a. NSAIDs are the other half of the pathway, the side that deals with prostoglandin formation. b. Read slide c. Salicylate was a precursor for aspirin. d. Will see patiens on more than 10 different NSAIDs. A wide number out there. i. They are each from different chemical families. e. Lots of chemical structures that can block prostoglandins synthesis. f. Not addictive, sedative, and don’t cause respiratory depression (yay!). g. At low doses they have analgesic properties, and at high doses they have antiinflammatory effects. i. If you want an anti-inflammatory response from aspirin, can’t take just one baby aspirin a day. XVII. NSAIDs Mechanism of Action [S17] a. Recognize that glucocorticoids block the action of phospholipase. They block everything! They are not NSAIDs. NSAIDs block the action of cyclo-oxygenases. XVIII. Roles of COX-1 and COX-2 [S18] a. Cox 1 is found in ceratin places where cox 2 isn’t. b. Cox 1 levels are usually the same even if there is no inflammation. i. It plays ordinary and normal roles in the GI tract and stomach. It accelerates the blood flow through the gastric lining of the stomach. If you inhibit this, blood flow is impaired, and you put yourself at risk for gastric inhibition. ii. In the platelets, will have more clots when cox 1 is active, and less clots when it is inactive (is a pro-coagulant). iii. Will maintatin blood flow throughout the kidney. If an NSAID is taken at too high of a dose, can get renal shut down. Prostoglandins normally aid in blood flow throughout the kidneys, so if you block prostoglandin production, blood flow through the kidney decreases c. The inducible form, cox 2, goes up when you have inflammation, pain, or fever. Cox 2 selective inhibitors have less effects on the GI and platelets, but will still have the negative effects on the kidney. XIX. Effects of Prostaglandins [S19] Class: Fundamentals II Professor: Pillion Date: 12/03/10 6 Scribe: Ashley Russell Proof: Louisa Warren a. Read slide b. PGE2 is protective for your GI tract and stomach c. PGF2 is important during pregnancy and can be given if trying to induce an abortion. Causes strong uterine contractions. d. TxA2= thrombxane e. So, get inhibition AND stimulation of clotting. Need a balance between the two. If you inhibit this pathway, need to be careful about platelet aggregation changes. XX. Clinical Effects of NSAIDs [S20] a. read slide XXI. Side-Effects of NSAIDS [S21] a. Read slide b. CNS effects are rare c. GI intolerance and increased bleeding are the most problematic. XXII. Gastroprotective Role of PGE [S22] a. Read slide b. Increased epithelial growth helps to repair damage or wounds. c. If you inhibit PGE, will have a negative effect (as far as the gastroprotective roles of PGE go). XXIII. Graph [S23] a. Does this GI toxicity represent a clinical problem? b. NSAIDs cause more deaths in the US than AIDS. c. Tens of thousands of people die every year from NSAIDs overuse i. Leads to GI bleedouts. ii. Those that do survive, lead to an enormous cost burden. XXIV. Renal Complications of NSAIDs [S24] a. Read slide b. Hyperkalemia = high potassium. XXV. Common Drug Interactions S25] a. can interfere with loop diuretics and thiazide which can effect how much urine we put out. b. SSRI: selective seratonin reuptake inhibitors (given for depression) i. The metabolism of SSRIs and Beta Blockers is the same as for NSAIDs, which can cause problems. c. Before you recommend that a patient take ibuprofin for pain, make sure you look and see what other medications they are taking. XXVI. Nonselective COX inhibitors [S26] a. These are different families of drugs; this list will increase the longer we are in practice. b. Some are very common, and others are used in specific niches. i. i.e indomethacin is used commonly in the treatment of gout as opposed to ibuprofin which is used more commonly for a headache. XXVII. Properties of NSAIDS [S27] a. Don’t have to memorize this chart, just recognize that there are drastic differences. b. Aspirin is sort of an outlier with a very quick halflife. i. Aspirin is checmially the acetylated form of *************** ii. That acetyl group makes it unique; can covalently bind to cyclooygenase and irreversibly inhibit it. 1. Every other NSAID is a reversible inhibitor of COX 2. This means that if I take a small dose of aspirin, the dose is high enough to interact with platelets and will interact the cyclooxygenase and irreversibly inactivate it. So, if a person has been taking aspirin, they will have a decreased clotting. Only way to recover is to make new platelet. To get a total turnover of new platelets, will take about a week. 3. This is not a complete shutdown of the clotting pathway, but diminishes one arm of the clotting pathway. Class: Fundamentals II Professor: Pillion Date: 12/03/10 7 Scribe: Ashley Russell Proof: Louisa Warren 4. Should get patients to stop taking aspirin about a week before a surgery. XXVIII. Aspirin (ASA) [S28] a. Read slide XXIX. Aspirin (ASA) part 2 [S29] a. If somebody ties to kill themselves with Aspirin, will get vomiting, tinnitus (ringing in the ears), decreased hearing, body temperature will go up, cardiac palpitations, and eventually will die. This is a common mechanism of suicide. b. Will want to pump the stomach or give activated charcoal to try and bind the aspirin in the stomach before it gets absorbed. c. If you make the urine more basic, can increase the removal of aspirin from the blood stream. d. Most kids with a fever are given Tylenol (acetaminophen) over aspirin because of Reye’s syndrome. XXX. Ibuprofin S30] a. Read slide. b. Have to go up to higher doses to get the anti-inflammatory affects. XXXI. Other commonly prescribed NSAIDs [S31] a. Read slide XXXII. Risk Factors for Serious NSAID GI toxicity [S32] a. Old people with a lot of aches and pains who take a lot of aspirin are the ones more likely to suffer from NSAID toxicitiy. XXXIII. CNS complications of NSAID use [S33] a. Read slide XXXIV. Inflammation and NSAIDs Summary [S34] a. Read slide XXXV. NSAID drug Interactions [S35] a. Read slide XXXVI. Selective COX-2 inhibitors a. introduced a few years; b. minimal effects on platelets and GI tract c. Still have negative effects on the kidneys XXXVII. Selective COX-2 inhibitors: a. Celecoxib, rofecoxib and valdecoxib b. Rofecoxib and valdecoxib have been recalled because of cardiovascular events c. Celecoxib is still on the market and is very carefully monitored and has a black box warning (could be dangerous, so it’s not used that much). XXXVIII. Roles of Cox I and Cox 2: a. Cox 2 is both inducible and constitutive. We want to block the inducible Cox2. b. The constitutive one goes along with it, unfortunately, so you get renal problems. XXXIX. Cox-2 selective NSAIDs a. pictures. XL. Cox-2 Inhibitors a. read slide XLI. Acetaminophen: a. Not a very good anti-inflammatory b. Usually the test question that you get with acetaminophen is: i. What is its toxicity? Why is it different? 1. Hepatic (liver) and is different because it’s not a good anti-inflammatory. People try to overdose and die becauses of liver damage. XLII. Acetaminophen: a. Read slide b. Is metabolized in the liver by glucuronidation or GSH conjugation. c. Toxic because it uses up all the GSH (normally, body has enough GSH to metabolize it all, but if you don’t have enough GSH, the acetaminophen will bind to the proteins in your liver. Class: Fundamentals II Professor: Pillion Date: 12/03/10 8 Scribe: Ashley Russell Proof: Louisa Warren i. Acetylcystein is the antidote. ARS Question: a. Thromboxane A2 is responsible for which biological effect? b. Different prostoglanins have different effects. XLIV. Review: a. ANSWER: D, platelet aggregation. XLV. ARS Question: a. Which one of the following drugs can cause vomiting, tinnitus, and vertigo at high doses? XLVI. Review: a. ANSWER: Aspirin XLVII. Gout a. A unique form of irritation from the build up of uric acid in the blood stream b. The levels of uric acid get so high that you get a build up of monosodium urate crystals c. So much of the salt builds up that you form a crystal (not a good thing to have in your body) i. Crystals will get in the way and cause inflammation and pain. ii. Cardinal sign is that the big toe gets red and inflamed from the presence of uric acid crystals d. There isn’t a lot you can do to treat it, but can give NSAIDs to help the inflammation. e. Two ways to treat gout: i. Decrease the amount of uric acid that you make: 1. Enzyme pathway can be inhibited by Allopurinol a. ii. Also, can get more uric acid to come out of your urine called Probenecid 1. Increases uric acid excretion. iii. Can give a person with drugs because they work differently f. Colchicine: not really an NSAID, but binds to microtubules and prevents cells from changing their shapes. i. Turns out, that if a person is on that drug, they won’t mount an inflammatory response as well as a person who is not on that drug. ii. Doesn’t cure gout, but can give some relief. Especially useful if given within 24 hours of an attack. XLVIII. Gout: Pathogenesis: a. High levels of uric acid is called hyperuricemia. b. Problem in gout: People will over produce uric acid or decrease their excretion of gout. XLIX. Gout Pathogenesis: L. Uric Acid Synthesis: a. Enzyme that is involved in producing uric acid is xanthine oxidase this is the site of allopurinol activity. LI. Clinical Presentation of Gout: a. In the big toe LII. Management of Gout: a. Management will include: i. Indomethacin, colchicine and glucocorticoids 1. Glucocorticoids like prednisone depleats their entire inflammatory response. LIII. Colchicine Colchicine is the anti-mitotic drug and binds tubulin, given in the first 12-36 hours of the attack. a. Best if given in the first 12-36 hours b. ASE: diarrhea is especially bad LIV. XLIII. Class: Fundamentals II Professor: Pillion Date: 12/03/10 9 Scribe: Ashley Russell Proof: Louisa Warren LV. Uricosurics: a. Will help to increase excretion of uric acid by increasing renal excretion b. Probenecid and Sulfinpyrazone are two drugs in this family. LVI. Probenecid LVII. Sulfinpyrazone LVIII. Allopurinol: a. Decreases uric acid production **Note: Dr. Pillion ran over these last several slides on gout very quickly. Most of the important information though, is listed in the slides. [End 49:50 mins]