11 Inflammation
advertisement

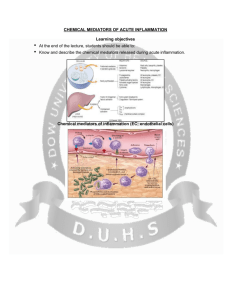
11TH LECTURE Physiotherapy INFLAMMATION ACUTE INFLAMMATION A rapid response to an injurious agent that serves to deliver leukocytes and plasma proteins to the site of injury TRIGGERS OF ACUTE INFLAMMATION Infections (bacteria, virus, parasite) Physical and chemical agents (thermal injury, irradiation, chemicals) Tissue Necrosis Trauma Foreign bodies (splinters, dirt, sutures) Hypersensitivity or autoimmune reactions MAJOR COMPONENTS OF INFLAMMATION: 1. Vascular response Increased vascular diameter Increased flood flow Endothelial cell activation increased permeability that permits plasma proteins and leukocytes to leave the circulation and enter the tissue edema increased expression of cell adhesion molecules e.g. Eselectin, ICAM 2. Cellular response Migration of leukocytes (diapedesis/extravasation), accumulation, effector functions THE CLASSIC SYMPTOMS OF INFLAMMATION • • • • • Redness (rubor) Swelling (tumor) Heat (calor) Pain (dolor) Loss of function (functio laesa) Resident phagocytes get activated by PRR signalization upon recognition of danger signals Production of cytokines and chemokines, Intracellular killing Antigen presentation (activation of adaptive responses) ORDER OF INNATE CELLS APPEARANCE IN THE INFLAMED SITE NEUTROPHIL GRANULOCYTES • 68% of circulating leukocytes, 99% of circulating granulocytes • Phagocytic cells • Not present in healthy tissues • Migration elimination of pathogens (enzymes, reactive oxygen intermediates) • Main participants in acute inflammatory processes NEUTROPHIL CHEMOTAXIS NEUTROPHIL TRANSENDOTHELIAL MIGRATION (DIAPEDESIS) PATHOGENS ACTIVATE MACROPHAGES TO RELEASE CYTOKINES AND ARE THEN PHAGOCYTIZED AND DIGESTED IN PHAGOLYSOSOMES THE EFFECTS OF CYTOKINES ON VARIOUS TISSUES Local effect Systemic effect THE ARACHIDONIC ACID PATHWAY NSAIDs and Paracetamol prevent the synthesis of prostaglandins by inhibiting COX-1 and COX-2 CHEMICAL MEDIATORS AND INFLAMMATION COMPONENTS II Vasodilation – Prostaglandins (PG), nitric oxide (NO) Increased vascular permeability – vasoactive amines (histamine, serotonin), C3a and C5a (complement system), bradykinin, leukotrienes (LT), PAF Chemotactic leukocyte activation – C3a, C5a, LTB4, chemokines (e.g. IL-8) CHEMICAL MEDIATORS AND INFLAMMATION COMPONENTS II Fever • IL-1, IL-6, TNFα, PGE2 Pain • Prostaglandins, bradykinin Tissue damage • Neutrophil and Macrophage products – lysosomal enzymes – Reactive oxygen species (ROS) – NO TREATING INFLAMMATION Goals 1) Pain relief 2) Slow or arrest tissue-damaging processes NSAIDs Aspirin DMARDs Corticosteroids NSAIDs have analgesic and antipyretic effects, but its their anti-inflammatory action that makes them useful in management of disorders where pain is related to the intensity of an inflammatory process (rheumatic diseases for ex.) NSAIDs mechanism of action: 1. Inhibiting prostaglandin synthesis 2. Inhibiting chemotaxis 3. Downregulation of IL-1 expression 4. Decrease free radicals and superoxides NSAIDs NON-STEROIDAL ANTI-INFLAMMATORY DRUGS Flurbiprofen Naproxen Ibuprofen Diclofenac Gels containing an anti-inflammatory agent are commonly used in physiotherapy, both for pain relief and for minimizing the tissue damage related to chronic inflammation SALICYLATES ASA Mesalazine / Mesalamine CORTICOSTEROIDS Prednisolone Methylprednisolone Triamcinolone betamethasone Budesonide THE ACUTE PHASE RESPONSE IL- 6 C-reactive protein Mannose binding lectin/protein Opsonization Complement activation MBL/MBP Opsonization Complement activation Liver SP-A and SP-D Opsonization in the lung Serum Amyloid Protein (SAP) Opsonization Binding of mannose/galactose (chromatin, DNA, influenza) Complement activation Fibrinogen Blood clot formation Converts thrombin fibrin ACUTE-PHASE RESPONSE PROTEINS Opsonization Complement activation RESOLUTION OF ACUTE INFLAMMATION Monoclonal antibodies (MAb) Products of one B-lymphocyte clone Homogeneous in antigen specificity, affinity, and isotype BIOLOGICAL THERAPY MONOCLONAL ANTIBODIES (MAB) THERAPEUTIC USE OF MAB 1) Anti-TNF-α therapy in rheumatology 2) Anti tumor therapy / Targeted chemotherapy. CD20+ anti-B-cell monoclonals in non-Hodgkin lymphoma. Monoclonal antibodies are cell-type specific, but not specific to malignant cells! 3) Immunsuppression. cell-type specific. Prevention of organ rejection after transplantation. !!! 1) Anti-TNF-α therapy 1. Anti-TNF-α antibodies Infliximab (Remicade): since 1998, chimeric Adalimumab (Humira): since 2002, recombinant human 2. Etanercept (Enbrel) – dimer fusion protein, TNF-α receptor + Ig Fc-part Not a real monoclonal antibody, no Fab end, the specificity is given by TNF-receptor! Indications of anti-TNF-α therapy • Rheumatoid arthritis • Spondylitis ankylopoetica (SPA - M. Bechterew) • Psoriasis vulgaris, arthritis psoriatica • Crohns’ disease, colitis ulcerosa (usually - still – not in the first line!) 2) Anti tumor therapy 2) Anti tumor therapy Transtuzumab Rituximab Anti-ErbB2 For breast cancer Anti CD20 for non-hodgkin’s lymphoma Cetuximab Anti EGFR Bevacizumab Anti VEGF For colorectal cancer 3) Immunosuppression Daclizumab Basiliximab Immunosuppresion by targeting IL-2Rs on T cells prevention of transplantation rejection Others: Omalizumab Anti-IgE for moderate to severe allergic asthma (binds mIgE-expressing B cells, not those already bound to the high affinity FcεRI