Your Biological Brothers & Sisters
advertisement

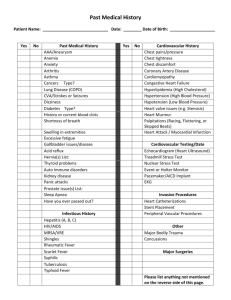
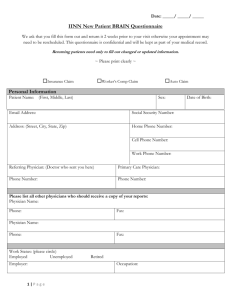
Why have I been given a family history form? You have been given a Family History Form because of concerns about the cancers that have occurred in your family. This may be because there have been several cancers in your family or because you or a relative had cancer at a young age. In most families, cancers will have occurred by chance. However, a small proportion of cancers (less than 10%) are due to an inherited predisposition. Before we try and answer your questions about your risk of cancers and whether extra screening is beneficial for you, it is important to try and collect as much information as possible about your family history, using this form. How is the information I give used? The information you provide will be used to: ✪ Assess your personal risk of developing cancer. ✪ Suggest an appropriate screening (surveillance) program for you. ✪ Help provide similar advice for other members of your family. How should I fill in the form? Please complete the form giving as much information as possible about your blood relatives, including those who have not had cancer. Indicate half brothers and sisters with an asterisk (*) and whether they are related to you through your mother or through your father. An example of how to fill in a row for someone who has had cancer is given on the form. If you need extra space, use the Additional Relatives sheet on the back of the Medical History Form, and you can continue on a separate sheet if necessary. What if I don’t know all these details? If you do not know all the information, perhaps someone else in the family would be able to help you. If this is not possible please do not worry, just provide the information you can. You can write “don’t know” in the boxes you cannot fill. Dates of birth/death: If you do not know the full date, the year or a rough date is still helpful (eg. 1920-1930). Type of cancer: We need to know where in the body individuals had cancer(s) (eg. breast, bowel, lung) or if they have had bowel polyps. If a relative had cancer but you don’t know where, write “Unknown cancer”. If a cancer started in one place and then spread to another, it does NOT become a different cancer. For example, if breast cancer spread to someone’s bones, it is only breast cancer. It is NOT now bone cancer. Age at diagnosis: Please put the age at which your relative was diagnosed for each cancer they had. If you have any questions regarding this form please contact Caring For Women: Phone (940) 591-6700 Email: forms@cfwdenton.com Fax (940) 320-1220 Personal History Name: Date of Birth: Which provider is your Cancer Prevention Plan schedule with? Yes Have you or any of your relatives had genetic testing? If yes, please complete the information below. Name Relationship Gene tested No Laboratory used Result Please check the ethnic/ racial background that best describes you and your parents. Check all that apply. White/ Caucasian Black/ African American Asian Spanish/ Hispanic/ Latino Unknown Other What countries are your ancestors from? (Example: Mexico, China, England) Mother’s side: Father’s side: Is either side of your family of Ashkenazi (Eastern/Central European) Jewish descent? Have you ever been diagnosed with any type of cancer? If yes, what type(s) and at what age(s) were you diagnosed? Age Yes Yes No Cancer Type Age at first period Age at first birth Have you had any breast biopsies? If yes, how many? Yes Age at menopause No If yes, at what age(s)? If yes, what were the results? Did the biopsy show atypical hyperplasia? DCIS or LCIS? Yes No Yes No Unknown 3 Have you had a hysterectomy (removal of uterus)? If yes, at what age? No Reason Have you had an oophorectomy (removal of ovaries)? If yes, at what age? Yes Yes No Reason Do you have unusual skin findings (lumps, bumps, lesions, light or dark spots)? Describe: Have you had colon polyps? Yes No Type (example: hyperplastic, adenoma, etc.) Age Number Yes No No Family History Your Biological Parents First Name Mother: Father: Alive/ Deceased Current age or age at death Affected with cancer? Age at cancer diagnosis Type of cancer Smoker A/D Y/N Y/N A/D Y/N Y/N Your Biological Grandparents Current age or age at death Affected with cancer? Age at cancer diagnosis First Name Alive/ Deceased Type of cancer Your Mother’s Mother A/D Y/N Y/N Your Mother’s Father A/D Y/N Y/N Your Father’s Mother A/D Y/N Y / NY / N Your Father’s Father A/D Y/N Y/N Smoker Your Biological Children First Name Alive/ Deceased Current age or age at death Affected with cancer? Age at cancer diagnosis Smoker A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N Have any of the relatives listed on this page been diagnosed with colon polyps? If so, please list names Type of cancer Yes No Your Biological Brothers & Sisters **Note – include full and half siblings. Please indicate any half siblings with an asterisk (*) and “M” or “F” to indicate which parent you share. Current age or Affected Age at Alive/ age at with cancer First Name Deceased death cancer? diagnosis Cancer type Smoker A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N Your Nieces & Nephews (Children of your brothers & sisters) First Name Sex Child of which Alive/ sibling Deceased Current age or age at death Affected with cancer? Age at cancer diagnosis Type of cancer Smoker M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N Have any of the relatives listed on this page been diagnosed with colon polyps?: If so, please list names Yes No Your Maternal Aunts & Uncles (your mother’s brothers and sisters) First Name Alive/ Deceased Current age Affected Age at or age at with cancer death cancer? diagnosis Type of cancer Smoker A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N Your Maternal Cousins (children of your maternal aunts & uncles) First Name Sex Child of which sibling Current age or Alive/ age at Deceased death Affected Age at with cancer Type of cancer? diagnosis cancer Smoker M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N Have any of the relatives listed on this page been diagnosed with colon polyps? If so, please list names Yes No Your Paternal Aunts & Uncles (your father’s brothers and sisters) First Name Alive/ Deceased Current age or age at death Affected with cancer? Age at cancer diagnosis Type of cancer Smoker A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N A/D Y/N Y/N Your Paternal Cousins (children of your paternal aunts and uncles) First Name Sex Child of which sibling Alive/ Deceased Current age or age at death Affected with cancer? Age at cancer diagnosis Type of cancer Smoker M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N M/F A/D Y/N Y/N Have any of the relatives listed on this page been diagnosed with colon polyps? If so, please list names Yes No Additional Relatives Please list any additional relatives who have had cancer in the space below. Also note how this person is related to you. First Name Alive/ Deceased Current age or age at death Affected with cancer? A/D Y/N A/D Y/N A/D Y/N A/D Y/N A/D Y/N A/D Y/N A/D Y/N A/D Y/N Please list any other important information here: Age at cancer diagnosis Type of cancer Related How?