SOAP Note Avascular Necrosis
advertisement

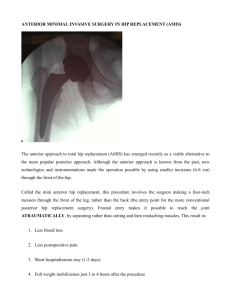
SOAP Note Avascular Necrosis Elijah Hanna PA-S Lock Haven University PA Program 7-22-12 Name: ***** **** MRN: ******** Race & Gender: Caucasian Male Insurance: Blue Cross Blue Shield Date Of Birth: 12/13/1974 Date: 7/14/2012 S: CC: “Left hip pain for the last 6 months” HPI: A 37-year-old Caucasian male presents to the orthopedic clinic by referral from his PCP for left hip pain that has been going on since February. The patient denies any history of trauma or specific injury in February or before. He says the pain is within the groin area and radiates to his lateral left hip. He rates the pain as a 2/10 at rest, and an 8/10 with movement (10/10 being when he fractured his 5th metacarpal). Patient states that the pain has progressively gotten worse, and when it started in February he had no pain at rest. The pain is described as achy at rest and sharp with movement. The patient states that he has tried Aleve for the pain, which helped initially, but no longer has a beneficial effect. He says that any movement of his legs or long periods of sitting make the left hip hurt. Specifically, he says that any rotating movements while standing, and sitting on his motorcycle hurt the most. The patient is able to get around without assistance, but does say he has started to limp while walking. He says that he is able to walk for about 20 minutes before he is forced to rest, and let the pain subside. He believes he manages fine for now, but is worried it will continue to get worse. He states that his PCP told him that he was referring him to Orthopedics because conservative treatment has failed, and his x-ray findings of the left hip were abnormal. The patient denies any other symptoms of the hip, back, or leg including: bruising, numbness, tingling, or paralysis. He denies any other joint pain, swelling, redness or stiffness. He denies any other muscle pain, weakness, or limitations in range of motion. PMH: The patient has a history of Type 1 Chiari Malformation (congenital, but adultonset) in which he developed hydrocephalous and had a ventriculo-peritoneal shunt placed. He was diagnosed with this 3 years ago, and the shunt treatment has worked well. The patient denies any history of anemia, CAD, HTN, DM, CVA, RA, STDs, cancer, bone or cartilage disease, or any other congenital diseases. Immunizations: Up to date Injuries: 5th metacarpal fracture (Boxer’s Fx.) February 2001 Surgeries: Ventriculo-peritoneal shunt placement in July 2009 Hospitalizations: For the shunt placement mentioned above, 2 day duration Medications: Aleve 400mg BID x’s 6 months, Prednisone 20mg daily x’s 3 years (suppression for shunt placement) Herbs/Vitamins: Echinacea 400mg daily x’s 1 year Allergies: NKDA, No food or environmental allergies known of Family History: Father, 58 years old, history of DM Type 2, DJD and Obesity Mother, 57 years old, alive and well Paternal Grandfather, Deceased at 64 from MI Paternal Grandmother, 77 years old, alive and well Maternal Grandfather, 79 years old, alive and well Maternal Grandmother, Deceased at 71 from Alzheimer’s disease Social History: Patient has been happily married to ***** **** for the last 15 years, and they have two boys ages 14 and 12 that are doing well. He says that they are both monogamous and enjoy an active, happy sexual life. They live in a threebedroom home that runs from well water. He reports no financial problems, and thinks his lifestyle is non-stressful. He works as a full time mechanic, which he loves to do, but his current left hip pain is hindering his work performance. Patient denies any history of tobacco or drug use. Patient says he is a social drinker, and will drink 3-4 beers on special occasions. Patient says he has a good, well-balanced diet. Patient claims he use to exercise daily, but stopped about ten years ago because he didn’t have as much time. R.O.S.: General: Patient denies any fevers, weight loss/gain, fatigue, weakness, appetite loss, chills, difficult sleeping or night sweats. Skin: Patient denies any rashes, itching, bruising, dryness, redness or lesions. Patient denies any other changes to hair, skin or nails. Respiratory: Patient denies any chest pain, dyspnea, cough, sputum production, hemoptysis, or history of infection of TB. Cardiac: Patient denies any chest pain, dyspnea on exertion, palpitations, murmurs or congenital abnormalities/complications. Musculoskeletal: (In HPI) O: Vital Signs: Temperature- 98.7 F (Ear), Heart Rate- 80bpm, Respiration Rate14bpm, Blood Pressure- 132/86 (L arm, Sitting), Height- 71in, Weight- 168lbs General: Patient appears as stated age, well developed, and in no acute distress. The patient is mild mannered, well spoken, and has no difficulty with any speech or social interaction. The patient is appropriately dressed and appears to have good hygiene. There are no abnormal olfactory or extracorpeal clues noted. Skin: There are no rashes, eruptions, bruising, redness, swelling, dryness or lesions. The hair is in appropriate distribution, smooth, and well kept. The nails reveal no clubbing, merckes lines, beaus lines, thickening, pallor, or pitting. Chest/Lungs: Inspection reveals no scars, lesions, masses, accessory muscle use or asymmetrical chest wall movements. Patient has no pain upon palpation, 1:2 AP/lateral ratio, and symmetrical respiratory excursion. Auscultation reveals clear, unlabored breath sounds in all lung fields and no adventitious sounds such as rales, ronchi, or wheezes. Cardiac: Inspection of precordium reveals no lifts, heaves or visible PMI. Palpation reveals no lifts, heaves, or thrills. Auscultation reveals regular rate and rhythm, S1, S2 and no murmurs, clicks, gallops or rubs. Musculoskeletal: Inspection of the left hip reveals no bruising, redness, swelling or lesions. The patient has no pain upon palpation over the greater trochanter or medially towards the groin. The patient is able to flex the hip to ~100, and extend the hip to 0. He is able to actively internally and externally rotate the hip, but notes the 8/10 pain mentioned in the HPI. Passive range of motion reveals normal musculature tone, no clicking or popping, and no crepitus. Hip flexion, extension, abduction, and adduction strength is equal bilaterally at +5. The patient has a positive Faber and log roll test with a negative straight leg raise test. Patient’s gait reveals a significant limp that attempts to compensate for left hip pathology. The rest of the patient’s musculoskeletal examination at the shoulders, neck, back, right hip, knees, and ankles reveal full active range of motion, and 5/5 strength bilaterally with no pain, swelling, or redness at the joints. Neurologic: Patient had normal sharp v. dull, and light touch sensation on the lower extremities bilaterally. Patient had normal 2-point distinction on the feet bilaterally. Patient had normal proprioception and vibratory sense of the great toe bilaterally. Pulses: Pulses at the brachial, femoral, and dorsalis pedis are equal bilaterally at +2 intensity. Patient had capillary refill in the great toes at <2 seconds bilaterally. Radiographs: Patient’s AP and lateral view x-rays were reviewed during the visit by Dr. Thomas R. Bowen MD. In his expert opinion the patient’s radiographs revealed significant osteonecrosis of the subchondral femoral heads bilaterally. There is minor collapse of the left femoral head with areas of bone on bone contact on the lateral aspect of the acetabulum. A: Diagnosis: Avascular necrosis of the femoral heads bilaterally (collapse of the left femoral head which is symptomatic) secondary to chronic steroid suppression Differential Diagnosis: DJD, Osteoporosis, Osteitis deformans (Paget’s Disease) P: Pending Labs: CBC w/ differential, BMP, Bone specific ALP Pending Imaging: MRI w/ contrast of both femoral heads (Pending normal BUN/Cr ratio evaluated from BMP), DEXA scan Treatment: Diclofenac 75mg BID Patient Education: Patient is educated on the pathology of avascular necrosis, and the progression of the disease. He is told that it is commonly precipitated by chronic steroid use, and in his case he had a good reason to be on them for his ventriculoperitoneal shunt. We talked about the likelihood that no matter what the confirmatory diagnosis is that he will need a left total hip arthroplasty. He was educated that due to the severity of bone and articular degeneration in his left hip he would likely not gain function without pain again, and it would most likely continue to progress. Also, with his right hip, even though now asymptomatic, he could develop the same complications because there are already significant imaging findings characteristic for AVN. The patient is educated on possible treatments for his right, asymptomatic hip including core decompression and FVFG, which would both require a surgical procedure as well. The patient asked if he should discontinue his steroids now, but was advised not to until his neurologist was consulted and made the decision. Patient was given handouts explaining total hip arthroplasty, core decompression, and FVFG. He is told to read up on all the procedures and think about what he wants to do if the pending labs and imaging confirm AVN and the need for surgical intervention. Referrals/Consults: Patients PCP (Dr. John Fanelli MD) and Neurologist (Dr. Wayne Simcox MD) will be consulted about new AVN findings. Provider Notes: Need to talk to Dr. Simcox about the patient’s chronic steroid use and the need for continued use. If Dr. Simcox believes that the patient can discontinue the chronic steroid suppression we can do so immediately. My initial thoughts is that this will not be an option, and we will have to continue to monitor the pathology of the major joints effected by AVN secondary to chronic steroid use including the shoulder, knee, ankle, and mandibular joints. If the ALP test comes back as abnormal there is a need to look in to the possible diagnosis of Paget’s disease. Follow Up: Patient will follow up to review laboratory and imaging results in 2 weeks. Patient is told that if the pain gets significantly worse within the next two weeks he should call the office. Elijah Hanna PA-S (7/14/12)