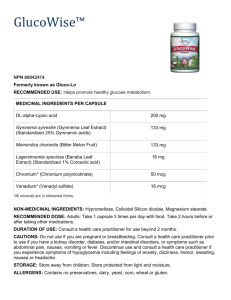
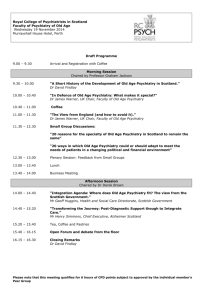
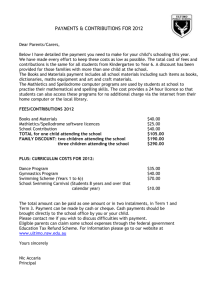
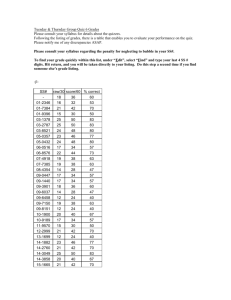
WIH C/L Resident Guide 2015
advertisement

WOMEN & INFANTS HOSPITAL Psychiatry Consultation/Liaison Rotation Guide C/L Rotation Guide Rotation Goals & Objectives Psychiatry Call Manual Day Hospital Rotation Guide WBH Clinical Services WIH Phone Numbers Cerner EMR Guide Psychiatry Note Templates Common Abbreviations Resources for Medications & Referral Options Updated 10/7/15 pages 2-3 page 4 pages 5-9 page 10 pages 11-12 page 13 page 14 pages 15-17 page 18 pages 19 1 Rotation Guide for Women & Infants Psychiatry Consult Service Welcome to your PGY-2 psychiatry consultation-liaison rotation at Women & Infants Hospital! We are excited to have you join us, and hope you will enjoy learning about women’s mental health during your time with us. The manual provides a lot of valuable information about your experience here, so please be sure to review it prior to the start of your rotation. Before the Rotation: 1-2 weeks before rotation, call 274-1122 x41925 OR e-mail fniang@wihri.org, to contact Fran Niang for the necessary documentation for your rotation and to get a computer log-on and Cerner access. You will get a welcome email several weeks prior to the start of your rotation reminding you of this. Please also be sure to read this guide in its entirety prior to your first day of the rotation. General Info Computer: Cerner is the electronic medical record. See Cerner guide below for more details. There are templates for the consult note and follow up note if you choose to use them. Food: ABP on the ground floor, and cafeteria in the basement. ABP and RIH cafeteria through the tunnels. 2 Dudley Street also has a café on the first floor. Locations: Consult office located in the Department of Medicine Suite on the third floor of the main hospital. Code to enter office area is 1884* the DOM suite is down the corridor to the left. WBH (outpatient) in 1st floor Coop building (2 Dudley Street) Day hospital 1st floor Coop building (2 Dudley Street) Phone Numbers: see WIH phone numbers list on page 13 Codes: Triage Entry Code: 0101 Social Work Office entry code: 4321 (consult office key kept next to printer) (make sure we still have access to this office) 3rd floor code: 1884* Amion code for W&I: wihri (www.amion.com) Consult Service Basics Attendings: Carmen Colomer, MD Pager: 401-582-4581 Email: ccolomer@wihri.org Cell: 617-459-1210 Laura Hollar-Wilt, MD Pager: 401-582-4410 Email: lhollarwilt@wihri.org Cell: 717-903-6786 Neha Hudepohl, MD Pager: 401-582-9416 Email: nhudepohl@whiri.org Cell: 513-659-8559 Updated 10/7/15 2 HT Kao, MD Pager: 401-582-7461 Jessica Pineda, MD Pager: 401-582-4532 Email: jpineda@wihri.org Cell: 513-532-4889 Women’s Mental Health Fellow: Nina Gonzales, MD (2015-16) Pager: 401-582-2157 Email: ngonzales@wihri.org C/L Social Worker: Erin Hunt, LICSW Pager: 401-582-0312 Email: ehunt@wihri.org Cell: 505-795-6263 Cell: 401-440-1277 Showtime: On your first day, 8AM @ Department of Medicine Suite on 3rd floor of main hospital. You will meet with Fran Niang initially to complete housekeeping requirements followed by a brief orientation and tour of the main hospital with the C/L Social Worker at 9am. Subsequently, your day will begin at 8am unless otherwise specified by the team. What to expect: You will be expected to carry the consult pager and will most likely be the first point of contact for all consult calls. Expect to initially evaluate most consults either on your own or with the C/L SW as appropriate. It is important to talk with nursing staff/social work and obtain collateral information whenever indicated. You will write your initial consult evaluation (save but do not sign without reviewing with attending.) You will present patients to your attending during “table rounds” and you and your attending will round on patients together during “bedside rounds”. You will also be expected to see follow ups whenever needed and to communicate psychiatry recommendations to the primary teams. Expect to be available to see consults until 5PM unless it is a didactics/clinic day. Also, please try to see all follow ups before 12:30PM. Service Schedule: Plan to check in with the C/L team at 8am unless otherwise specified. You will spend your mornings seeing new and follow-up consults. If there are no new or pressing follow-ups , plan to spend your morning in the Day Hospital. Check in with the Day Hospital attending and let her know if there are pending consult follow-ups so you can best plan your time. On your didactic/clinic days, you will check in with your attending at 11am prior to leaving. On your full days, plan to round with your team at 2pm unless otherwise specified. Generally, the daytime team will accept new consults until about 4pm, and later if there is an emergency. Consults called later than that will either be saved until the next day, or if absolutely necessary, seen by the on- call physician. This decision will be determined by the attending. C/L Team Structure: The WIH C/L Team is comprised of an attending physician, resident, and psychiatric social worker. The C/L Social Worker serves as an anchor for the team by triaging cases, assisting with coordination of behavioral treatment, and evaluating patients as needed. At times there may also be a women’s mental health fellow on the team. Updated 10/7/15 3 Consult Rotation Goals & Objectives To demonstrate understanding of the unique needs of the perinatal population, including diagnostic assessment and treatment modalities. To develop a framework for approaching clinical decision making in the pregnant and breastfeeding patient. To develop an initial understanding of basic attachment patterns and disrupted attachment, as well as the implication of maternal mental illness on child development. To acquire expertise in liaison work in the setting of a specialty hospital. To expand knowledge on the application of non-pharmacologic evidence-based interventions for perinatal mental illness. To review details about perinatal mental illnesses, including postpartum depression, postpartum psychosis, perinatal-onset OCD, trauma-related illnesses, and psychiatric disorders in the gynecologic-oncology population. Updated 10/7/15 4 Call Manual for Women & Infants Hospital As the only psychiatry consultation service at a specialty women’s hospital, we provide a significant amount of expertise in dealing with psychiatrically ill patients at Women & Infants Hospital. Both our academic and community referral sources rely on our expertise in the care of their patients. To that end, we strive to be readily available both during the workday and after hours to help care for these patients. General Information: Weekday call: Begins Monday at 5PM and ends Friday at 8AM (weeknight call is 5pm-8am nightly during the week). Weekend call: Begins Friday at 5PM and ends Monday at 8AM. During your PGY-2 rotation, you will take 1 week of call (usually Monday at 5pm – Monday at 8am). Prior to coming on call you must be sure that your Cerner password is active. Please check with the chief resident for WIH (Brian Theyel MD) regarding your Cerner login/password. Most of you should already have this access from your C/L rotation in the past. If you had access in the past but need to update your password, contact Butler computer support at 921-1000 or the WIH Helpdesk at 274-1122 ext. 48777. You should check your Cerner access while at Butler Hospital (under the CNErgy Cerner icon) in advance of your call. You are expected to refresh or familiarize yourself with this system prior to being on call. You must be free of other call responsibilities including other moonlighting and jeopardy call. While you are on call you will be supervised by an attending. You will receive a call schedule distributed in advance by the chief resident as well as an email reminder at the start of your call. You can also check AMION (www.amion.com password = wihri) for the backup attending information. It is your responsibility to know when you are on call and who your backup attending is. You will be emailed any relevant consult sign-out to your Brown email accounts, but will be sent via encrypted email with “PHI” in the subject line.Please be sure to provide relevant information regarding the consult service in sign out to the primary team via secure email. Weeknight and Weekend Call: Consult requests can be reviewed with your backup attending prior to coming into the hospital, unless it is a clear emergency. Many, but not all, consults may be seen or evaluated by a social worker prior to you being called, unless it is a psychiatric emergency. Due to the untimed nature of obstetrics, patients may not come to the attention of either SW or psychiatry until over the weekend. Because these patients are likely to be discharged home over the weekend it is our policy to evaluate consults called in on the weekends. Often social work will have seen these patients first, but sometimes the primary team will call the psychiatry team directly especially if there is a question related to medications or safety. As a general rule, all consults must be seen and completed within 24 hours of consultation request. If you are called on a consult that can be pushed until the primary team returns (the following morning), please email or page the psychiatry resident or attending covering consults for the next morning by Updated 10/7/15 5 8:00AM with the information including patient name, room number, DOB, and any other pertinent information Consultation Requests: There are important psychiatric emergencies that necessitate having to come in. When in doubt, we err on the side of coming in to evaluate patients. The following list constitutes what our service generally considers to be emergent: Acute onset of delirium in patients who are not responsive to the initiation of the Delirium Care Plan Acutely agitated, behaviorally dysregulated, or actively suicidal/homicidal patients on the medical or obstetrical floors Patients where there is a high index of suspicion for post-partum psychosis. These patients must be evaluated rapidly! Substance abuse patients in active withdrawal that cannot be managed by current protocols at WIH Capacity assessments where there is a high degree of risk for death or injury to patient or fetus, or a significant change in care or assessment due to refusal of recommended care, or desire to leave AMA. Patients in Triage Any other patient for which the primary team is requesting an urgent consult. Transfer Protocols for Women & Infants: Pa ent evaluated in triage by primary psych team or on call resident – decision is made for inpa ent treatment Once pa ent medically cleared… Fax clinical informa on, demographics, & med list to Butler PAS @ 401-455-6532. Call Butler PAS @ 401-455-6346 within 30 minutes to discuss bed availability & transfer No fy WIH Staff to facilitate MD:MD & nurse:nurse Obtain Precer fica on from insurance & no fy PAS Transfer Policy –Triage Updated 6/23/14 If pa ent is too agitated to be managed by WIH staff, WIH staff to transfer to a secure facility/D-POD RIH. Call D-POD resident @ 401-444-3640. Follow steps as detailed below If Bed @ Butler not available Contact D-POD resident to inquire if space is available-401-444-3640. . If no room, call other facili es & WIH to hold pt un l a bed is found. Follow protocols for transfer as requested by accep ng facility. Pa ent to be kept at WIH un l bed available. D pod able to accept pa ent Call D-POD resident. If pt accepted, call RIH Access @ 401-444-3000 to provide demographics for pre-registra on. Fax clinical informa on & med list to 401-444-9866. Facilitate nurse:nurse @ 401-444-3640. No fy WIH staff to facilitate ambulance transfer No fy WIH staff to arrange ambulance transport & provide paperwork to send with pa ent Updated 10/7/15 6 Pt evaluated by primary psychiatry team or on call resident – decision is made for inpa ent admission Once pa ent is medically cleared… Fax clinical informa on, demographics, & med list to Butler PAS @ 401-455-6532. Call Butler PAS @ 401-455-6346 within 30 minutes to discuss bed availability & transfer. Pa ent cannot be transferred to a lower level of care (LOC) Eg. RIH ER/D-POD Transfer Policy—WIH Main Floors Updated 6/23/14 If pa ent is agitated Manage agita on with primary providers, psychiatry C/L team, & security No fy WIH staff to facilitate MD:MD & Nurse:Nurse Obtain Precert & No fy PAS No fy WIH staff to coordinate ambulance transport & provide paperwork to send with pt Updated 10/7/15 When pt stabilized Follow protocol for IP admission, if deemed necessary 7 Calls for other reasons: The backup attending covers any calls from outpatient attendings on weeknights and weekends. If you are called on an outpatient in Women’s Behavioral Health, have the answering service call your backup attending. If you are called about an active Day Hospital patient or a Project Link patient, then refer the caller to the therapist on call for these respective programs (can be found in AMION). The answering service should also have a list of who is on call for these programs. Emergency Slots: One emergency slot is available for patients over the weekends that need immediate follow-up evaluation and/or care. This slot is primarily available to pregnant or postpartum women. The slots are scheduled on Mondays at 8:30AM (Or Tuesdays at 8:30AM if there is a holiday on Monday). These are 60-90 minute slots with a psychiatric clinician who will have backup from a psychiatrist if it is clinically warranted. The patient should be directed to Women’s Behavioral Health at 2 Dudley Street, First floor and given the number (401) 453-7955. As the on-call psychiatry resident, you will be responsible for managing the use of this emergency appointment. Remember, there is only 1 slot and once filled, it is no longer available. The social workers should contact you if they have a patient they would like to refer to that slot, but it is ultimately your decision how that slot is utilized. Please notify the following individuals about a patient booked in an emergency slot. Please provide the patient’s name, DOB, contact phone number as well as a brief description of the clinical circumstances. Margaret Howard (mhoward@wihri.org) Judy Randall (jlrandall@wihri.org) Erin Hunt (ehunt@wihri.org) Please use a secure email address to send this information. Consult Documentation: Women and Infants Hospital has an electronic medical records system (Cerner) and all consult notes are to be written in Cerner. Prior to coming on call you must be sure you have your Cerner access active. Please check with the WIH Chief Resident Brian Theyel MD regarding your Cerner login/password if you are uncertain of it. Consultation notes are within the “Clinical Notes” section and should be documented in the same fashion as a standard psychiatric consultation note or H&P. Please see the Consult Note Templates below for further details. Please contact either the WIH Chief Resident or your supervising attending if you have any questions about documenting in Cerner. We encourage you not to wait until the start date of call to do this. Please add any new consults seen/called to the “WIH BH Consults” list in Cerner (see Cerner guide for more details). Attending Contact Information: Carmen Colomer, MD Pager: 401-582-4581 Email: ccolomer@wihri.org Cell: 617-459-1210 Thamara Davis, MD Updated 10/7/15 8 Pager: 401-582-0144 Cell: 401-663-5590 Email: thamara.davis.md@gmail.com or familyinstitute@gmail.com Laura Hollar-Wilt, MD Pager: 401-582-4410 Email: lhollarwilt@wihri.org Cell: 717-903-6786 Margaret Howard, PhD Pager: 401-582-4618 Email- mhoward@wihri.org Cell: 401-368-2180 Neha Hudepohl, MD Pager: 401-582-9416 Email: nhudepohl@whiri.org Cell: 513-659-8559 HT Kao, MD Pager: 401-582-7461 Jessica Pineda, MD Pager: 401-582-4532 Email: jpineda@wihri.org Cell: 513-532-4889 Lawrence Price, MD Home: 401-245-9246 Email: lprice@butler.org Cell: 401-523-4315 On Call Telephone Tree: Call your listed backup attending I I (If unavailable after 15 minutes, try backup attending again – consider alternate number) After 2 tries or 30 minutes I V Call Neha Hudepohl MD, Medical Director, Women’s Behavioral Health AND/OR Margaret Howard PhD, Division Director, Women’s Behavioral Health I (If unavailable after 2 tries or 30 minutes) I I V Call Lawrence Price MD Chief of Psychiatry, Women & Infants Hospital Updated 10/7/15 9 Rotation Guide for Women & Infants Day Hospital While you are on service at Women & Infants, the psychiatry consultation/liaison service is your primary clinical responsibility; however, you will often have free time during the mornings and can participate in clinical care at the Day Hospital. This is a unique experience and will help expose you to women’s mental health and perinatal psychiatry in a partial hospital setting using the concept of a mother-baby unit. While participating in the Day Hospital, you will attend groups, rounds and participate in individual patient care. Residents have found this to be a very valuable experience and a great introduction to the care of pregnant and postpartum women. Location: 2 Dudley Street, Co-Op Care Center, First floor . There is signage pointing you in the right direction. Phone: 401-274-1122 ext. 42870 Schedule: 8:30-9:00AM First Rounds – discuss new admissions, potential discharges, and other patientrelated issues for Day Hospital patients 9:00-10:15AM Morning IPT Group 10:15-10:30AM Brief Rounds 10:45-11:30AM Morning Skills Group/Individual sessions with patients 11:45AM-12:15PM Lunch 12:15-12:45PM Relaxation Group 1:00-2:15PM Afternoon Skills Group 2:15-2:30PM Wrap Up What to expect: You will attend group whenever possible, participate in rounds and be asked to see patients for individual sessions for either psychotherapy or a medication evaluation. At times, you will also be asked to evaluate newly admitted patients on their first day and present to the psychiatrist. When possible, you may also be involved in intake appointments (evaluating patients prior to admission to the Day Hospital). Showtime: First rounds begin at 8:30AM, but remember that consults are your first priority. Documentation: At this time, the Day Hospital uses paper charting. Initial evaluations (the “7 page” form), interim evaluations (the “4 page” form), and progress notes are available from the secretary. When medication changes are made or at the initial or discharge evaluation, a medication reconciliation must be completed in Cerner (see Cerner guide). Updated 10/7/15 10 Women’s Behavioral Health Clinical Services Division Director: Margaret Howard, PhD Medical Director: Neha Hudepohl MD Associate Division Manager: Judy Randall Psychiatry Inpatient Consultation/Liaison Service: Pager # 582-4404 Social Worker: Erin Hunt, LICSW Attending Psychiatrists: Carmen Colomer, MD Laura Hollar-Wilt, MD Neha Hudepohl, MD Women’s Behavioral Health (outpatient): Ann Back Price PCNS, IAAP Laura Chalk CNM, PCNS Carmen Colomer, MD Shannon Erisman, PhD Aimee Grause, PCNS Jane Hesser, LICSW Laura Hollar-Wilt, MD Margaret Howard, PhD Neha Hudepohl, MD Erin Hunt, LICSW Jessica Pineda, MD Alpha Roca, LCDP (case manager) Kristen Wedel, LCSW Main # 453-7955 Day Hospital (partial hospitalization program): Main # 274-1122 x42870 Clinical Director: Shannon Erisman, PhD Attending Psychiatrists: Carmen Colomer, MD Laura Hollar-Wilt, MD Neha Hudepohl, MD Clinical Staff: Ann Back Price PCNS, IAAP Laura Chalk, CNM, PCNS Aimee Grause, PCNS Kristen Wedel, LCSW Brown Clinical Psychology Resident Case manager: Alpha Roca, LCDP Partial hospitalization program for pregnant and postpartum women with mood and anxiety disorders focused on IPT/attachment issues and women are encouraged to bring their babies. Admit up to 1 year PP. Research: Research Psychologist: Cynthia Battle PhD Women’s Mental Health Fellowship: Program Director: Neha Hudepohl, MD Updated 10/7/15 11 Associate Program Director: Margaret Howard, PhD Research Director: Cynthia Battle, PhD Fellow 2015-16: Nina Gonzales, MD Fellowship Coordinator: Fran Niang Updated 10/7/15 12 Important WIH Phone Numbers **must dial 4 before 4-digit extension** Main #WIH Main # WIH Shuttle Computer Help 274-1100 (for operator) 274-1122 (automated when you know your extension) x41635 x48777 CL work room 3rd floor Social work main desk Day Hospital Women’s Behavioral Health Francois Niang Judy Randall x42360 x41360 x42870, x42878 453-7955, backline x42788, x42755 x41925 x42710 Admissions Ambulatory Surgery LDR PACU Triage ACU (4 North & South) 4 East 4 West 5 East 5 East Nursery 6 East 6 East Nursery 6 West 6 West Nursery NICU 2 North & South NICU 3 North & South WPCC East WPCC West MFM Gyn Onc work room x41422 x41423 x41300 x41400 x41500 x41520 x41750 x43400 x41512 x41812 x41810 x41801 x41507 x41506 x41503 x41502 x43200 x43300 x42785 x42793 x42354 x41279 Updated 10/7/15 13 Cerner (EMR) Guide The “List” To get the WBH Consult Patient list: -log on, click on Patient List on the tool bar - click on button that looks like a wrench in upper left corner, it is called “list maintenance” -click “new,” then click “care team” -scroll down to team called “WIH BH Consults,” press finish -it should be in your “available list” column, click the right handed arrow to move it to “active list,” press ok Add patient to the list: -within your WBH Consult Patient List screen, click on icon that is a person with a sparkle aka “Add a patient” -look patient up by name, MR or location -select the active encounter for current admission, and hit “Add” The Chart—Double-click on the patient; this will take you to the summary screen. There is a tab on the left side of the screen called “Menu – Inpatient” that if you click on it will give you the following tabs: -Summary screen: is exactly that, a summary, has current meds, vitals, recent labs, allergies -Patient info: Click on Visit list -- you can see if they have ever seen Women’s Behavioral Health or the Day program. If so, call Tina x2870 and have her fax the intake/discharge summary -Results Review: labs/x-rays/nursing assessments (includes agitation, CIWA, etc). On the central blue stripe that has a clinical date range listed, right click to change the dates so you can see the whole hospital stay or look for labs that were done before the admission -Clinical notes: All notes written on the patient. Double click to open each folder. First, Right click on the central blue stripe that has a clinical date range listed, change the initial day to 1/1/2003, which is when the hospital went electronic OR just change the year of the date listed to 2000. -Consultation notes have social work consults and psychiatric consults -Emergency Department notes have why they were admitted -Progress notes for what is going on here and now. THIS INCLUDES F/UP CONSULT NOTES. -History and Physical sometimes they have this separate entry, tons of info -PowerOrders: then click on consults, so you can see who ordered the consult and why -eMar : electronic MAR, helpful to see what meds they actually got and when Writing Notes— -click into “Clinical Notes” tab from the Menu – inpatient menu -click on the button in upper left that looks like a paper with a sparkle aka “add” -in the new screen that pops up, in the “type” drop down box, right click and click on “document type list” then click on “complete” -then in “type” drop down box, scroll to “psychiatric consult” or “psychiatric progress note” -click on button in upper left that looks like a stamp aka “template” -click on the type of template you want, and then click insert -now just type the info you want into the note! Updated 10/7/15 14 Psychiatry Initial Consult Note Template Initial Psychiatric Consultation (Date) Reason for Consultation: (Please also list who is requesting the consult—generated by SW, primary team, specialty service) Chief Complaint: “ “ Identifying Information: -include age, demographics, G/P status if pregnant/postpartum, age of gestation if pregnant, reason for hospitalization HPI: -note that you reviewed the chart -that you saw the patient, where and who was present -planning to breastfeed? -pregnancy planned? Reaction to pregnancy? Partner’s reaction? How did pregnancy go? -psychiatric review of systems (depression, mania, psychosis, anxiety disorders) Past Psychiatric History: Any inpatient, partial, IOP treatment? Any outpatient treatment? Previous suicide attempts? Previous medication trials? Should we include Past Reproductive History? Substance Abuse History: Include pertinent negatives – nicotine, caffeine, alcohol, cannabis, other drugs. Ask about taking non-prescribed prescription medications. PMH: Include whether hx of TBI, seizures, asthma, headaches, relevant past surgical history Medications: Copy and paste active inpatient meds from Summary tab in Cerner Allergies: Include reaction Family History: Include any Fhx suicide Social History: refer to social work note for complete history. Living situation? History of interpersonal violence? Education level? Employment or source of income? Relationship with FOB if relevant? Other children in the home, previous DCYF involvement? Developmental history? O: Vital Signs: Most recent set of vitals - Copy and paste from Summary tab in Cerner MSE: Appearance: Eye Contact/Behavior: Speech: Mood: Updated 10/7/15 15 Affect: Thought Process: Thought Content: evidence of delusions/paranoia, any intrusive thoughts? SI/HI: any SI/HI/thoughts of dying/harming infant thoughts etc? Perceptual: Orientation: Cognitive exam: include MOCA/MMSE if relevant Insight/Judgment: Labs: last 100 results reviewed/any abnormalities noted OR labs reviewed from past 3 months/12 months/etc. Impression/Recommendations: “This is a …. “ Diagnosis: Psychiatric Diagnosis: Medical Diagnosis: Psychosocial Stressors: Recommendations: -agree with social work involvement for __________ (support, liaison for housing, etc) -no acute/imminent safety concerns (unless there are…then comment) -other recommendations including medications, follow up, etc. Thank you for the consult. Our team will/will not continue to follow while in the hospital. Impression/recommendations communicated to PRIMARY ATTENDING. (your name, PGY-?) Psychiatry Follow Up Consult Note Template Psychiatry Consult Service Follow Up Note (date) Events overnight: -include nursing reports S: -patient’s report Medications: Copy and paste active inpatient meds from Summary tab in Cerner O: -add vital signs if relevant MSE: Appearance: Eye Contact/Behavior: Speech: Mood: Updated 10/7/15 16 Affect: Thought Process: Thought Content: evidence of delusions/paranoia, any intrusive thoughts? SI/HI: any SI/HI/thoughts of dying/harming infant thoughts etc? Perceptual: Orientation: Cognitive exam: include MOCA/MMSE if relevant Insight/Judgment: -add labs if relevant Impression/Recommendations: “This is a …. “ Diagnosis: Psychiatric Diagnosis: Medical Diagnosis: Psychosocial Stressors: Recommendations: -agree with social work involvement for __________ (support, liaison for housing, etc) -no acute/imminent safety concerns (unless there are…then comment) -any changes/updates to plan or plan to continue previous recommendations -follow up plans Thank you for the consult. Please call with further questions OR Our team will continue to follow while in the hospital. Impression/recommendations communicated to PRIMARY ATTENDING. (your name, PGY-?) Updated 10/7/15 17 Commonly Used Abbreviations ACU = antenatal care unit AMS = acute monitoring service AVD = assisted vaginal delivery BPP = biophysical profile CSR = C-section recovery CTX = contractions, ceftriaxone EBL = estimated blood loss EDD = estimated date of delivery FHT = fetal heart tones FOB = father of baby G#P# = gravida/para GBS = group B streptococcus GDM = gestational diabetes mellitus GTT = glucose tolerance test IOL = induction of labor IPV = intimate partner violence IUD = intrauterine device IUFD = intrauterine fetal demise LDR = labor & delivery room LEEP = loop electrosurgical excision procedure LMP = last menstrual period MFM = maternal-fetal medicine MOB = mother of baby OCP = oral contraceptive pill PACU = post-anesthesia care unit PCS = primary C-section PEC = pre-eclampsia PIH = pregnancy-induced hypertension POC = products of conception POD # = post-operative day # PPD # = postpartum day # PPTL = postpartum tubal ligation PPROM = preterm premature rupture of membranes PROM = premature rupture of membranes RCS = repeat C-section REI = reproductive endocrinology & infertility SS = social services SS = social services postpartum SVD = spontaneous vaginal delivery TOF = tetralogy of Fallot UDS = urine drug screen US = ultrasound VAVD = vacuum-assisted vaginal delivery VBAC = vaginal birth after cesarean WIH = Women & Infants Hospital WPCC = Women’s Primary Care Clinic NICU = neonatal intensive care unit Updated 10/7/15 18 Resources on Medications in Pregnancy and Breastfeeding Through Care New England: For side effects and risks for all medications in pregnancy and breastfeeding: https://home.carenewengland.org/micromedex2/,DanaInfo=www.thomsonhc.com+librarian (OR link through Micromedex on the Carenet Library page) and do a search for the medication in question. Scroll to the bottom of the results list and click on the "reproductive risk" section. We usually use the "Reprotox" reference of the choices given. Click on that and it will have a recent summary of all known info on the drug in pregnancy and breastfeeding. It also covers some herbs and supplements. When appropriate, you can often print a copy and give it to the patient. For trainees who want access to Reprotox from home or sites without access, you can get a free subscription: www.reprotox.org Free resource for lactation only (LACTmed): http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT Another helpful resource for patient friendly information/printouts on medications is www.mothertobaby.org Other Resources: Toxicology and Teratology: Motherrisk www.motherisk.org/prof/index.jsp Organization of Teratology Information Specialists – OTIS - www.mothertobaby.org Postpartum Psychiatric Disorders: MedEdPPD - www.mededppd.org Professional education, a peer-reviewed site Postpartum Support International – www.postpartum.net Addiction and Pregnancy: National Advocates for Pregnant Women - www.advocatesforpregnantwomen.org Guttmacher Institute - www.guttmacher.org/sections/pregnancy.php Drug Policy Alliance Lindesmith Library - www.drugpolicy.org/library/ Smoking in Pregnancy in Rhode Island: Quitworks RI: A free, evidence-based stop-smoking service developed by the Rhode Island Department of Health. http://quitworksri.org/ or Email: quitworksriinfo@jsi.com Telephone: 1-800-TRY-TO-STOP (1-800-879-8678) Fax: 1-866-560-9113 Updated 10/7/15 19