Barker et al. (2014)_JSS_accepted
advertisement
_JSS_accepted")
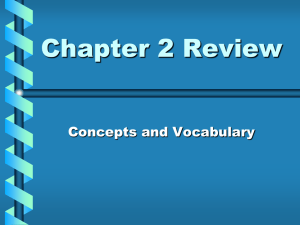
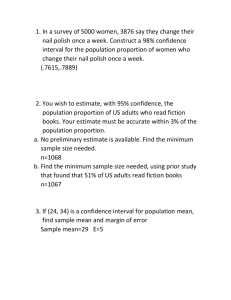
1 The influence of 2 weeks of low volume high-intensity interval training on health outcomes in adolescent boys Running title: High-intensity interval training and health outcomes in adolescent boys Key words: Trainability, youth, aerobic fitness, lipid oxidation, blood pressure, BMI. 2 ABSTRACT The present study aimed to establish whether 2 weeks of high intensity interval training would have a beneficial effect on aerobic fitness, fat oxidation, blood pressure and body mass index (BMI) in healthy adolescent boys. Ten adolescent boys (15.1 ± 0.3 y, 1.3 ± 0.2 years post peak height velocity) completed six sessions of Wingate-style high-intensity interval training over a 2 week period. The first session consisted of four sprints with training progressed to seven sprints in the final session. High-intensity interval training had a beneficial effect on maximal O2 uptake (mean change, 90% confidence intervals: 0.19 L·min-1, ±0.19), the O2 uptake at the gas exchange threshold (0.09 L·min-1, ±0.13) and on the O2 cost of sub-maximal exercise (-0.04 L·min-1, ±0.04). A beneficial effect on the contribution of lipid (0.06 g·min-1, ±0.06) and carbohydrate (-0.23 g·min-1, ±0.14) oxidation was observed during sub-maximal exercise, but not for the maximal rate of fat oxidation (0.04 g·min-1, ±0.08). Systolic blood pressure (1 mmHg, ±4) and BMI (0.1 kg·m2, ±0.1) were not altered following training. These data demonstrate that meaningful changes in health outcomes are possible in healthy adolescent boys after just 6 sessions of high-intensity interval training over a 2 week period. 3 INTRODUCTION Physical activity and aerobic fitness are independent predictors of cardio-metabolic health in young people (Andersen et al., 2006; Ekelund et al., 2007). Consequently, the health benefits of regular physical activity are of importance to the public health agenda for researchers, educators and policy makers. Children and adolescents are recommended to undertake at least 60 min of daily moderate to vigorous exercise (Janssen & Leblanc, 2010). Studies employing objective assessment of physical activity however, demonstrate a marked decline in physical activity from childhood and during adolescence (Sherar, Esliger, Baxter-Jones, & Tremblay, 2007), and that few children and adolescents meet the recommended daily dose of physical activity (Metcalf, Voss, Hosking, Jeffery, & Wilkin, 2008; Riddoch et al., 2007). The efficacy of alternative forms of physical activity therefore needs to be considered in young people. Recent adult studies have shown low volume, high-intensity interval training to offer either similar or superior benefits to cardio-metabolic health outcomes compared to traditional continuous exercise (Gibala, Little, Macdonald, & Hawley, 2012). For example, just 2-6 weeks of high-intensity interval training in adults can enhance maximal oxygen uptake (𝑉̇ O2max) (Burgomaster et al., 2008; Macpherson, Hazell, Olver, Paterson, & Lemon, 2011; Whyte, Gill, & Cathcart, 2010), insulin-sensitivity (Babraj et al., 2009; Whyte, et al., 2010), lipid oxidation at rest (Whyte, et al., 2010) and during exercise (Burgomaster, et al., 2008), systolic blood pressure (Whyte, et al., 2010) and body composition (Macpherson, et al., 2011; Whyte, et al., 2010). In contrast, research studying the efficacy of high-intensity interval training on health related outcomes in children and adolescents is sparse. There is evidence showing 7- 4 8 weeks of high-intensity interval training improves 𝑉̇ O2max in healthy children (Baquet et al., 2010; McManus, Cheng, Leung, Yung, & Macfarlane, 2005). Furthermore, a recent study found 7 weeks of high-intensity interval training to improve physical performance (20 m shuttle run test, agility, 10 m sprint) and cardio-metabolic health (systolic blood pressure, body mass index [BMI]) outcomes in healthy adolescents (Buchan et al., 2011). To our knowledge however, no study has examined whether improvements in cardio-metabolic health outcomes are possible using high-intensity interval training over a 2 week period in youth, as has recently been demonstrated in adults (Babraj, et al., 2009; Whyte, et al., 2010). The purpose of the present study was to test the hypothesis that 2-weeks of highintensity interval training would improve aerobic fitness (e.g. 𝑉̇ O2max) and lipid oxidation during sub-maximal exercise, and reduce resting systolic blood pressure and BMI in healthy male adolescents. METHOD Participants Ten male 14-16 year old adolescents volunteered to take part in this study. The participants were 15.1 ± 0.3 years old and 1.3 ± 0.2 years post estimated peak height velocity. All participants and their parent(s)/guardian(s) provided informed assent and consent respectively, to partake in the project, which was approved by the institutional ethics committee. The participants were healthy, recreationally active, and showed no contraindications to perform maximal exercise. In addition to their weekly Physical Education classes, the participants were involved in 6.6 ± 3.0 hours 5 of organised sports participation on a weekly basis (e.g. cycling, running, sailing, cricket and swimming). Experimental protocol In line with related adolescent (Sperlich et al., 2011) or adult studies (Burgomaster, et al., 2008; Gibala et al., 2006; Jacobs et al., 2013; Whyte, et al., 2010) investigating high-intensity interval training, a control group was not employed in the current study for two reasons: 1) changes in the outcomes variables due to growth and maturation would be minimal over a 2 week period; 2) the participants refrained from participating in their usual weekly organised sports activities during the study, thus allowing the effect of the high-intensity interval training programme on the outcome variables to be observed. All participants visited the laboratory on 10 separate occasions over a 3 week period, with at least 24 hours rest provided between each visit. Visits 1 and 2 consisted of the pre-training outcome measures. Subsequently, participants returned to the laboratory for six sessions of highintensity interval training (visits 3-8), before completing the post-training measures (visits 9 and 10). For all visits the participants arrived at the laboratory in a rested state and were requested to refrain from consuming food and caffeine for at least 2 hours prior to testing. All exercise tests were performed using a mechanically braked cycle ergometer (Monark 827e/814e, Monark exercise AB, Sweden). The participants were habituated to the test procedures and protocols during visits 1 and 2. This included cycling on the ergometer at a set cadence with gas exchange measures, and attempting a number of short sprints (~ 5-10 s) in preparation for the high-intensity interval training programme. 6 Visits 1-2: Pre-training measures On visit 1, body mass (Seca 899, GmBH & co, Germany), seated height and stature (Harpenden Portable Stadiometer, Holtain, Wales) were measured to the nearest 0.1 kg and 0.1 cm respectively. Somatic maturity was estimated using sex specific equations to predict age from peak height velocity to within ±1 y accuracy (Mirwald, Baxter-Jones, Bailey, & Beunen, 2002): Maturity Offset (years) = -9.236 + 0.0002708·Leg Length and Sitting Height interaction -0.001663·Age and Leg Length interaction + 0.007216·Age and Sitting Height interaction + 0.02292·Weight by Height ratio R2 = 0.89, Standard Error of the Estimate = 0.59 years A combined ramp and supra-maximal exercise test to exhaustion was employed to determine 𝑉̇ O2max and the gas exchange threshold (Barker, Williams, Jones, & Armstrong, 2011). A step-incremental test to exhaustion was undertaken whereby power output increased at a rate of 21 W·min-1. Participants cycled at a cadence of 70 rev·min-1 and exhaustion was defined as a drop in cadence below 65 rev·min-1 for 5 consecutive seconds. Following a 15 min recovery, participants performed a supramaximal exercise bout to exhaustion at a power output corresponding to 105% of the peak power achieved during the incremental test. The highest 15 s averaged 𝑉̇ O2 during the ramp or supra-maximal test was taken as 𝑉̇ O2max. The 𝑉̇ O2 at the gas exchange threshold was identified as a disproportionate increase in expired carbon dioxide (𝑉̇ CO2) relative to 𝑉̇ O2 and the ventilatory equivalents for 𝑉̇ O2 and 𝑉̇ CO2 (Wasserman, Hansen, Sue, Stringer, & Whipp, 2005). 7 Participants returned to the laboratory ~ 48 hours after visit 1, for the meaurment of blood pressure using a portable mercury sphygmomanometer (Dekamet, Accoson, Essex, England) following 10 min of rest in the supine position. The median of three measures was taken as the participant’s blood pressure. Subsequently, the participants undertook a submaximal step-incremental exercise test to determine the relationship between 𝑉̇ O2, heart rate and substrate utilisation during steady state exercise. The exercise protocol started at 35W and increased in 3 min stages to ensure 7-10 stages were completed prior to achieving ~ 80% of the participant’s 𝑉̇ O2max (Zakrzewski & Tolfrey, 2011). Prior to visit 2, participants were provided with a food diary to record all the food and drink consumed during the day and were requested to replicate this for the post-training measures. The food diaries were assessed for total energy and macronutrient intake (CompEat Pro, Nutrition Systems, UK). Visits 3-8: High-intensity interval training programme Training commenced 2-3 days following completion of the pre-training measures. In line with the protocol originally described by Burgomaster et al. (2005), each participant performed a total of six high-intensity interval training sessions over a 2 week period. The first training session included four repeated 30 s sprints (e.g. Wingate anaerobic test), but this was progressed to include seven sprints on the final training session. Each high-intensity interval training session was preceded by a 5 min warm-up. Participants performed unloaded cycling at 100 revolutions per minute and were given a 5 s countdown prior to applying a resistance equivalent to 7.5% body mass (Barker & Armstrong, 2011). Participants were instructed to sprint ‘all out’ for 30 s and provided with 4 min of unloaded recovery at 70 revolutions per 8 minute between each sprint. Participants had at least 24 hours rest between each training session and completed three sessions each week. Power output was recorded in 1 s intervals, and used to determine peak power, mean power and fatigue index for each sprint. Heart rate was recorded throughout each training session. Participants received strong verbal encouragement during the training and completed this in pairs. Visits 9-10: Post-training measures Post-testing measures were undertaken 2-3 days following completion of the highintensity interval training programme and followed the same procedures as outlined for visits 1-2. The participants were provided with a copy of their food diary and asked to replicate this prior to the substrate utilisation test. Experimental measures Pulmonary gas exchange and ventilation were determined at 15 s averages using a commercially available system (Cortex Metalyzer II; Cortex Medical, Leipzig, Germany) that was calibrated prior to each test. Heart rate was recorded using short range radio telemetry (Polar Vantage NV, Polar Electro, Kempele, Finland). Energy expenditure and absolute and relative contributions of fat and carbohydrate oxidation during the sub-maximal incremental exercise test was estimated from the mean 𝑉̇ O2 and respiratory exchange ratio (RER) over the final 30 s of each 3 min stage using established equations (Frayn, 1983). Protein oxidation was assumed to be negligible, and an RER >1 was taken to represent 100% carbohydrate oxidation. As estimating lipid and carbohydrate oxidation via indirect calorimetry is valid up to ~ 9 85% 𝑉̇ O2max (Romijn, Coyle, Hibbert, & Wolfe, 1992), data that exceeded 80% 𝑉̇ O2max were not analysed. The maximal rate of fat oxidation and the point at which this occurred relative to 𝑉̇ O2max (FatMax) was visually identified by two independent investigators blinded to the participant and pre/post training measure. The visual method was employed as it has been shown to be consistent with non-linear curve fitting techniques (Zakrzewski & Tolfrey, 2011). Statistical analyses In line with recent statistical recommendations (Hopkins, Marshall, Batterham, & Hanin, 2009), we used 90% confidence interval to calculate probabilistic magnitude based inferences for the effect of high-intensity interval training on the outcome variables. Using a published spreadsheet (Hopkins, 2007), the mean difference for the outcome variable pre and post high-intensity interval training were calculated with a 90% confidence interval to represent the uncertainty of the true effect. In the absence of data concerning the smallest worthwhile change in the physiological outcomes reported in the current study, Cohen’s (1988) standardised effect size (ES) of 0.2 was employed, as recommended by Batterham and Hopkins (2006). Based on the smallest worthwhile change, the spreadsheet calculated the probability that the observed effect, captured using the 90% confidence interval, was either beneficial (positive, higher, faster), trivial or harmful (negative, lower, slower). The following probability thresholds were used to inform these decisions: <0.5%, most unlikely; 0.5-5%, very unlikely; 5-25%, unlikely; 25-75%, possibly; 75-95%, likely; 9599.5%, very likely; >99.5%, most likely (Batterham & Hopkins, 2006; Hopkins, et al., 2009). If a ‘possibly’ effect was observed, the percentage contribution of the majority of the distribution is provided. An effect was deemed to be trivial when the 10 majority (>50%) of the 90% confidence interval lay between beneficial and harmful. Conversely, an effect was deemed unclear when the likelihood of a beneficial and harmful effect was >5%. Descriptive statistics were calculated using SPSS (version 19.0, Chicago, USA) and presented as mean ± SD. RESULTS HIT training All participants completed the six high-intensity interval training sessions with no adverse effects resulting in a 100% adherence to the programme. Figure 1 illustrates the changes in peak power, mean power and the fatigue index over the initial four 30 s sprints during the first and final training session. Peak power output was meaningfully higher in the final compared to the first high-intensity interval training session for sprints 1 (very likely), 2 (very likely), 3 (most likely) and 4 (likely). There were no meaningful changes in the mean power output between the highintensity interval training sessions for all sprints (unclear), but the fatigue index was meaningfully elevated in sprints 1 (likely) and 3 (likely) during the final training session. The participants attained a peak heart rate equivalent to ~ 90-95% maximum during the high-intensity interval training sessions. ****Figure 1 near here**** Anthropometry, blood pressure and aerobic fitness The effect of high-intensity interval training on the physical and aerobic fitness variables are presented in Table 1. High-intensity interval training had no meaningful effect on body mass or BMI (ES=0.03). Changes in systolic (ES=0.07) and diastolic (ES=0.13) blood pressure were unclear. The high-intensity interval training 11 programme had a possibly beneficial effect on 𝑉̇ O2max whether expressed in absolute (73% beneficial, ES=0.30) or relative to body mass (71% beneficial, ES=0.30). In addition, high-intensity interval training had a very likely beneficial effect on time to exhaustion during the incremental cycle test (ES=3.99), which corresponded into a beneficial effect on peak power, with four participants completing one additional stage. Finally, high-intensity interval training had a possibly beneficial effect on the gas exchange threshold when expressed in absolute terms (56% beneficial, ES=0.23), but an unclear effect when expressed relative to 𝑉̇ O2max (ES=-0.05). ****Table 1 near here**** Sub-maximal substrate oxidation The energy intake for the participants on the day of the substrate oxidation test both pre and post high-intensity interval training was 689 ± 293 kcal, with a macronutrient contribution of 57 ± 8% carbohydrate , 28 ± 10% fat and 15 ± 7% protein. The steady-state physiological responses during the three initial stages of the sub-maximal test are presented in Table 2. The high-intensity interval training programme had a beneficial effect on sub-maximal 𝑉̇ O2 (69% beneficial, ES=-0.28), energy expenditure (ES=-0.55), RER (ES=-0.61) and on the absolute oxidation of lipid (ES=0.52) and carbohydrate (ES=-0.76). Consequently, there was a likely beneficial effect on the percentage contribution of carbohydrate (pre: 72.9 ± 11.3 vs. post: 62.7 ± 18.2%; change, 90% CL: -10.2%, ±8.4, ES=-0.62) and lipid (pre: 27.1 ± 11.3 vs. post: 37.3 ± 18.2%; change, 90% CL: 10.2%, ±8.4, ES=0.62) oxidation to the total energy expenditure during sub-maximal exercise (Figure 2). While an unclear effect was observed on the maximal rate of fat oxidation (pre: 0.28 ± 0.10 vs. post: 0.32 ± 0.14 g·min-1; change 90% CL: 0.04 g·min-1, ±0.08, ES=0.34), FatMax 12 was likely reduced (pre: 48.5 ± 14.3 vs. post: 39.5 ± 11.4 % 𝑉̇ O2max; change 90% CL: -9.0, ±9.4, ES=-0.64). On average, the participants were able to complete 1.2 ± 1.5 (range -1 to 3) additional stages for the assessment of lipid metabolism following high-intensity interval training. ****Table 2 near here**** ****Figure 2 near here**** DISCUSSION The novel findings from the current study are that 2 weeks of low volume, highintensity interval training in healthy adolescent boys: 1) had a beneficial effect on parameters of aerobic function (e.g. 𝑉̇ O2max); 2) increased the contribution of fat oxidation during sub-maximal steady state exercise; 3) had no effect on the maximal rate of fat oxidation and reduced FatMax, and 4) had no effect on blood pressure or BMI. This study therefore demonstrates for the first time that just six sessions of high-intensity interval training over a 2 week period can have a beneficial effect on a number of health related outcomes in adolescent boys. In agreement with the original description of the high-intensity interval training programme employed in the current study (Burgomaster, et al., 2005), the adolescent boys completed all 6 sprints with no adverse side effects and resulted in an increase in the peak, but not mean power output, and an increase in the fatigue index, from the first to the last training session. Interestingly, this data contrasts cross sectional evidence showing trained children and adolescents to exhibit an elevated peak power, mean power and reduced fatigue index compared to untrained counterparts (McNarry, Welsman, & Jones, 2011), whereas training studies have found increases 13 in peak and mean power output but not the fatigue index (Bogdanis, Ziagos, Anastasiadis, & Maridaki, 2007; Souissi et al., 2012). The boys achieved ~ 90-95% of their maximal heart rate during each high-intensity interval training session which is indicative of the large aerobic energy contribution that has been reported during exercise of this type (Bogdanis, Nevill, Boobis, & Lakomy, 1996; Hebestreit, Mimura, & Bar-Or, 1993). In the presence of this aerobic stimulus, recent studies on healthy adults have shown that 𝑉̇ O2max (Burgomaster, et al., 2008; Burgomaster, et al., 2005; McKay, Paterson, & Kowalchuk, 2009) or the gas exchange threshold (McKay, et al., 2009) is not improved after ~10-14 days of high-intensity interval training, but is after ~ 20-24 days. Our study extends this evidence base, as a possibly beneficial effect on 𝑉̇ O2max (~ 5% increase) and 𝑉̇ O2 at the gas exchange threshold (~ 5% increase) was observed after just 14 days of highintensity interval training in healthy adolescent boys. While this magnitude of the improvement in 𝑉̇ O2max following 2-weeks of high-intensity interval training is only marginally greater than the day to day reproducibility of measuring 𝑉̇ O2max in youth (~ 4%, Welsman, Bywater, Farr, Welford, & Armstrong, 2005), this is either greater (Williams, Armstrong, & Powell, 2000) or similar (Baquet, et al., 2010) to studies using a running high-intensity interval training programme over 7-8 weeks in 8-11 year old boys. In contrast, using an 8 week high-intensity interval training protocol consisting of seven 30 s maximal sprints at a power output corresponding to 𝑉̇ O2max, McManus et al. (2005) reported a ~ 11% and 18% improvement in 𝑉̇ O2max and the gas exchange threshold, respectively. Therefore, while the improvement in 𝑉̇ O2max and the gas exchange threshold in the current study after just 2 weeks of highintensity interval training is in line with traditional aerobic endurance programmes 14 lasting ~ 8-12 weeks in youth (Armstrong & Barker, 2011; Baquet, van Praagh, & Berthoin, 2003), further improvements may be possible using Wingate-based highintensity interval training over a longer time frame. Interestingly, we observed a reduction in the O2 cost to perform sub-maximal exercise, and thus a reduction in energy expenditure, in the present study which has not been identified in adult studies employing high-intensity interval training over a 2-4 week period (Burgomaster, et al., 2005; Gibala, et al., 2006; McKay, et al., 2009). This finding is surprising as longer training interventions are typically required to improve this parameter of aerobic function in adults (Jones & Carter, 2000), and previous high-intensity interval training and traditional aerobic endurance training programmes in youth that improve 𝑉̇ O2max do not impact exercise economy (Baquet et al., 2002; Rowland & Boyajian, 1995). While our finding of a reduced O2 cost of exercise following high-intensity interval training warrants further investigation, coupled with the increase in 𝑉̇ O2max one would predict an improved exercise tolerance, which was observed in the incremental test to exhaustion in the current study. This is in agreement with a recent study on adolescent soccer players where 5 weeks of high-intensity interval training improved both 𝑉̇ O2max and 1000 m running performance (Sperlich, et al., 2011). Unfortunately, we cannot provide mechanistic insight into the improvements in aerobic function (𝑉̇ O2max, gas exchange threshold and exercise economy) in the current study. However, a recent study on untrained adults employing a similar 2 week high-intensity interval training programme to current study observed improvements in 𝑉̇ O2max and exercise performance alongside an increase in muscle 15 oxidative capacity (cytochrome c oxidase activity) and muscle O2 extraction (Jacobs, et al., 2013). Interestingly, changes in ‘central’ factors such as maximal cardiac output, total haemoglobin and blood plasma volume were unaffected by 6 session of high-intensity interval training (Jacobs, et al., 2013), suggesting ‘peripheral’ adaptations may be responsible for the findings in the current study. This notion is corroborated by other adult work showing markers of mitochondrial biogenesis and muscle buffering capacity to be enhanced following a short programme of highintensity interval training (Gibala, et al., 2012). Studies in adults have shown that 2 weeks of high-intensity interval training increases the capacity for lipid oxidation both at the muscle and whole body level during sub-maximal exercise (Burgomaster, et al., 2008). This finding not only has implications for performance, possibly through sparing muscle glycogen utilisation (Burgomaster, et al., 2008), but also health, as a reduced capacity to oxidise lipid has been implicated in the storage of intramuscular lipids (Kim, Hickner, Cortright, Dohm, & Houmard, 2000) and body fat (Pagliassotti, Gayles, & Hill, 1997), and in the development of insulin resistance (Corpeleijn, Saris, & Blaak, 2009). In the current study we found high-intensity interval training to have a likely beneficial effect on lipid oxidation (absolute and relative contribution) during sub-maximal exercise, and a concomitant reduction in carbohydrate oxidation. Surprisingly, the increase in lipid oxidation following high-intensity interval training did not translate into an increase in the maximal rate of fat oxidation, which occurred at a lower percentage of 𝑉̇ O2max post-training. However, on average the participants were able to complete an additional 1.2 ± 1.5 stages during the sub-maximal test, indicating an increased capacity to oxidise fat at higher power outputs following high-intensity 16 interval training. While we are not aware of a previous study exploring the effect of high-intensity interval training on lipid oxidation in healthy youth, our data agree with a study showing sub-maximal lipid oxidation to be increased following 4 weeks of aerobic endurance training in healthy children (Duncan & Howley, 1998). Interestingly, studies on obese children have shown 2 months of continuous highintensity exercise training to reduce lipid oxidation (Brandou et al., 2005), whereas training at an intensity corresponding to the maximal rate of fat oxidation increased submaximal lipid oxidation and FatMax (Brandou, Dumortier, Garandeau, Mercier, & Brun, 2003), suggesting high-intensity interval training may not be beneficial for increasing lipid oxidation in obese youth. Buchan et al. (2011) have recently demonstrated that after 7 weeks of high-intensity interval training, both systolic blood pressure and BMI are reduced in healthy adolescents. Although similar benefits have been reported in sedentary, overweight/obese men following 2 weeks of high-intensity interval training (Whyte, et al., 2010), we found no meaningful changes in blood pressure or BMI following 2 weeks of high-intensity interval training. This suggests that a longer programme of high-intensity interval training may be needed to improve these outcomes, at least in healthy, normal weight and normotensive youths. This conclusion is supported by a recent review which concluded that a minimum of 12 weeks of high-intensity interval training may be needed to reduce BMI and systolic blood pressure in adults (Kessler, Sisson, & Short, 2012). A limitation of the current study is the lack of a control group that would provide comparative data for adolescents not undertaking the high-intensity interval training 17 programme. However, the lack of a control group is consistent with previous adolescent (Sperlich, et al., 2011) or adult (Burgomaster, et al., 2008; Gibala, et al., 2006; Jacobs, et al., 2013; Whyte, et al., 2010) high-intensity interval training studies. Furthermore, we also did not compare the efficacy of high-intensity interval training to moderate intensity exercise, which would enable a direct comparison against current physical activity recommendations. Finally, we were unable to determine the substrate oxidation under fasting conditions, but controlled for this by having each participant monitor and replicate their diet on the day of the submaximal substrate oxidation test. CONCLUSIONS The present study presents novel data showing that meaningful changes in health outcomes are possible after just 6 sessions of high-intensity interval training, equivalent to 16 min 30 s of high-intensity exercise, over a 2 week period. Specifically, beneficial effects were observed on parameters of aerobic function and lipid oxidation, but not for blood pressure and BMI. These findings therefore build upon recent evidence showing that either a single bout of high-intensity exercise (Burns, Oo, & Tran, 2012) or 7-8 weeks of low volume high-intensity interval training (Buchan, et al., 2011; McManus, et al., 2005) have a beneficial effect on health outcomes in youth. Given that children appear to prefer moderate intensity exercise interspersed with bouts of high-intensity sprints compared to moderate intensity exercise alone (Crisp, Fournier, Licari, Braham, & Guelfi, 2012), and that the majority of young people fail to achieve current physical activity recommendations, further work is needed to address the feasibility and efficacy of 18 using low volume high-intensity interval training to improve health outcomes in youth. ACKNOWLEDGEMENTS We thank the staff and participants at Sidmouth Community College and the staff at Sidmouth Leisure Centre for their participation in this project. REFERENCES Andersen, L. B., Harro, M., Sardinha, L. B., Froberg, K., Ekelund, U., Brage, S., & Anderssen, S. A. (2006). Physical activity and clustered cardiovascular risk in children: a cross-sectional study (The European Youth Heart Study). Lancet, 368, 299-304. Armstrong, N., & Barker, A. R. (2011). Endurance training and elite young athletes. Medicine and Sport Science, 56, 59-83. Babraj, J. A., Vollaard, N. B., Keast, C., Guppy, F. M., Cottrell, G., & Timmons, J. A. (2009). Extremely short duration high intensity interval training substantially improves insulin action in young healthy males. BMC Endocrine Disorders, 9, 3. Baquet, G., Berthoin, S., Dupont, G., Blondel, N., Fabre, C., & van Praagh, E. (2002). Effects of high intensity intermittent training on peak VO(2) in prepubertal children. International Journal of Sports Medicine, 23, 439-444. Baquet, G., Gamelin, F. X., Mucci, P., Thevenet, D., Van Praagh, E., & Berthoin, S. (2010). Continuous vs. interval aerobic training in 8- to 11-year-old children. Journal of Strength and Conditioning Research, 24, 1381-1388. Baquet, G., van Praagh, E., & Berthoin, S. (2003). Endurance training and aerobic fitness in young people. Sports Medicine, 33, 1127-1143. Barker, A. R., & Armstrong, N. (2011). Exercise testing elite young athletes. Medicine and Sport Science, 56, 106-125. Barker, A. R., Williams, C. A., Jones, A. M., & Armstrong, N. (2011). Establishing maximal oxygen uptake in young people during a ramp cycle test to exhaustion. British Journal of Sports Medicine, 45, 498-503. Batterham, A. M., & Hopkins, W. G. (2006). Making meaningful inferences about magnitudes. International Journal of Sports Physiology and Performance, 1, 50-57. 19 Bogdanis, G. C., Nevill, M. E., Boobis, L. H., & Lakomy, H. K. (1996). Contribution of phosphocreatine and aerobic metabolism to energy supply during repeated sprint exercise. Journal of Applied Physiology, 80, 876-884. Bogdanis, G. C., Ziagos, V., Anastasiadis, M., & Maridaki, M. (2007). Effects of two different short-term training programs on the physical and technical abilities of adolescent basketball players. Journal of Science and Medicine in Sport, 10, 79-88. Brandou, F., Dumortier, M., Garandeau, P., Mercier, J., & Brun, J. F. (2003). Effects of a two-month rehabilitation program on substrate utilization during exercise in obese adolescents. Diabetes and Metababolism, 29, 20-27. Brandou, F., Savy-Pacaux, A. M., Marie, J., Bauloz, M., Maret-Fleuret, I., Borrocoso, S., . . . Brun, J. F. (2005). Impact of high- and low-intensity targeted exercise training on the type of substrate utilization in obese boys submitted to a hypocaloric diet. Diabetes and Metabolism, 31, 327-335. Buchan, D. S., Ollis, S., Young, J. D., Thomas, N. E., Cooper, S. M., Tong, T. K., . . . Baker, J. S. (2011). The effects of time and intensity of exercise on novel and established markers of CVD in adolescent youth. American Journal of Human Biology, 23, 517-526. Burgomaster, K. A., Howarth, K. R., Phillips, S. M., Rakobowchuk, M., Macdonald, M. J., McGee, S. L., & Gibala, M. J. (2008). Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. Journal of Physiology, 586, 151-160. Burgomaster, K. A., Hughes, S. C., Heigenhauser, G. J., Bradwell, S. N., & Gibala, M. J. (2005). Six sessions of sprint interval training increases muscle oxidative potential and cycle endurance capacity in humans. Journal of Applied Physiology, 98, 1985-1990. Burns, S. F., Oo, H. H., & Tran, A. T. (2012). Effect of sprint interval exercise on postexercise metabolism and blood pressure in adolescents. International Journal of Sport, Nutrition, Exercise and Metabolism, 22(1), 47-54. Cohen, J. (1988). Statistical Power Analysis for the Behavioural Sciences (2nd ed.). Mahwah, NJ: Lawrence Erlbaum. Corpeleijn, E., Saris, W. H., & Blaak, E. E. (2009). Metabolic flexibility in the development of insulin resistance and type 2 diabetes: effects of lifestyle. Obesity Reviews, 10, 178-193. Crisp, N. A., Fournier, P. A., Licari, M. K., Braham, R., & Guelfi, K. J. (2012). Adding sprints to continuous exercise at the intensity that maximises fat oxidation: Implications for acute energy balance and enjoyment. Metabolism, 61, 1280-1288. 20 Duncan, G. E., & Howley, E. T. (1998). Metabolic and perceptual responses to short-term cycle training in children. Pediatric Exercise Science, 10, 110122. Ekelund, U., Anderssen, S. A., Froberg, K., Sardinha, L. B., Andersen, L. B., & Brage, S. (2007). Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: the European youth heart study. Diabetologia, 50, 1832-1840. Frayn, K. N. (1983). Calculation of substrate oxidation rates in vivo from gaseous exchange. Journal of Applied Physiology, 55, 628-634. Gibala, M. J., Little, J. P., Macdonald, M. J., & Hawley, J. A. (2012). Physiological adaptations to low-volume, high-intensity interval training in health and disease. Journal of Physiology, 590, 1077-1084. Gibala, M. J., Little, J. P., van Essen, M., Wilkin, G. P., Burgomaster, K. A., Safdar, A., . . . Tarnopolsky, M. A. (2006). Short-term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. Journal of Physiology, 575, 901-911. Hebestreit, H., Mimura, K., & Bar-Or, O. (1993). Recovery of muscle power after high-intensity short-term exercise: comparing boys and men. Journal of Applied Physiology, 74, 2875-2880. Hopkins, W. G. (2007). A spreadsheet for deriving a confidence interval, mechanistic inference and clinical inference from a P-value. Sportscience, 11, 16-20. Hopkins, W. G., Marshall, S. W., Batterham, A. M., & Hanin, J. (2009). Progressive statistics for studies in sports medicine and exercise science. Medicine and Science in Sports and Exercise, 41, 3-13. Jacobs, R. A., Flück, D., Bonne, T. C., Bürgi, S., Christensen, P. M., Toigo, M., & Lundby, C. (2013). Improvements in exercise performance with highintensity interval training coincide with an increase in skeletal muscle mitochondrial content and function. Journal of Applied Physiology. Available online. doi: 10.1152/japplphysiol.00445.2013 Janssen, I., & Leblanc, A. G. (2010). Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity, 7, 40. Jones, A. M., & Carter, H. (2000). The effect of endurance training on parameters of aerobic fitness. Sports Medicine, 29, 373-386. Kessler, H. S., Sisson, S. B., & Short, K. R. (2012). The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Medicine, 42, 489-509. 21 Kim, J. Y., Hickner, R. C., Cortright, R. L., Dohm, G. L., & Houmard, J. A. (2000). Lipid oxidation is reduced in obese human skeletal muscle. American Journal of Physiology Endocrinology and Metabolism, 279, E1039-1044. Macpherson, R. E., Hazell, T. J., Olver, T. D., Paterson, D. H., & Lemon, P. W. (2011). Run sprint interval training improves aerobic performance but not maximal cardiac output. Medicine and Science in Sports and Exercise, 43, 115-122. McKay, B. R., Paterson, D. H., & Kowalchuk, J. M. (2009). Effect of short-term high-intensity interval training vs. continuous training on O2 uptake kinetics, muscle deoxygenation, and exercise performance. Journal of Applied Physiology, 107, 128-138. McManus, A. M., Cheng, C. H., Leung, M. P., Yung, T. C., & Macfarlane, D. J. (2005). Improving aerobic power in primary school boys: a comparison of continuous and interval training. International Journal of Sports Medicine, 26, 781-786. McNarry, M. A., Welsman, J. R., & Jones, A. M. (2011). The influence of training and maturity status on girls' responses to short-term, high-intensity upperand lower-body exercise. Applied Physiology, Nutrition, and Metabolism, 36, 344-352. Metcalf, B. S., Voss, L. D., Hosking, J., Jeffery, A. N., & Wilkin, T. J. (2008). Physical activity at the government-recommended level and obesity-related health outcomes: a longitudinal study (Early Bird 37). Archives of Disease in Childhood, 93, 772-777. Mirwald, R. L., Baxter-Jones, A. D., Bailey, D. A., & Beunen, G. P. (2002). An assessment of maturity from anthropometric measurements. Medicine and Science in Sports and Exercise, 34, 689-694. Pagliassotti, M. J., Gayles, E. C., & Hill, J. O. (1997). Fat and energy balance. Annals of the New York Academy of Sciences, 827, 431-448. Riddoch, C. J., Mattocks, C., Deere, K., Saunders, J., Kirkby, J., Tilling, K., . . . Ness, A. R. (2007). Objective measurement of levels and patterns of physical activity. Archives of Disease in Childhood, 92, 963-969. Romijn, J. A., Coyle, E. F., Hibbert, J., & Wolfe, R. R. (1992). Comparison of indirect calorimetry and a new breath 13C/12C ratio method during strenuous exercise. American Journal of Physiology Endocrinology and Metabolism, 263, E64-71. Rowland, T. W., & Boyajian, A. (1995). Aerobic response to endurance exercise training in children. Pediatrics, 96, 654-658. Sherar, L. B., Esliger, D. W., Baxter-Jones, A. D., & Tremblay, M. S. (2007). Age and gender differences in youth physical activity: does physical maturity matter? Medicine and Science in Sports and Exercise, 39, 830-835. 22 Souissi, H., Chtourou, H., Chaouachi, A., Dogui, M., Chamari, K., Souissi, N., & Amri, M. (2012). The effect of training at a specific time-of-day on the diurnal variations of short-term exercise performances in 10- to 11-year-old boys. Pediatric Exercise Science, 24, 84-99. Sperlich, B., De Marees, M., Koehler, K., Linville, J., Holmberg, H. C., & Mester, J. (2011). Effects of 5 weeks of high-intensity interval training vs. volume training in 14-year-old soccer players. Journal of Strength and Conditioning Research, 25, 1271-1278. Wasserman, K., Hansen, J., Sue, D., Stringer, W., & Whipp, B. (2005). Principles of Exercise Testing and Interpretation. Including Pathophysiology and Clinical Application (4th ed.). Philiadelphia: Lippincott Williams & Wilkins. Welsman, J., Bywater, K., Farr, C., Welford, D., & Armstrong, N. (2005). Reliability of peak VO(2) and maximal cardiac output assessed using thoracic bioimpedance in children. European Journal of Applied Physiology, 94, 228234. Whyte, L. J., Gill, J. M., & Cathcart, A. J. (2010). Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metabolism, 59, 1421-1428. Williams, C. A., Armstrong, N., & Powell, J. (2000). Aerobic responses of prepubertal boys to two modes of training. British Journal of Sports Medicine, 34, 168-173. Zakrzewski, J., & Tolfrey, K. (2011). Exercise protocols to estimate Fatmax and maximal fat oxidation in children. Pediatric Exercise Science, 23, 122-135. 23 Table 1. The effect of 2-weeks of high-intensity interval training on physical, blood pressure and aerobic fitness outcomes Variable Pre-training Post-training Effect, ±90% CI 0.2, ±0.4 Inference Body mass 66.3 ± 11.9 66.5 ± 11.6 Trivial (kg) BMI 21.5 ± 2.6 21.6 ± 2.4 0.1, ±0.1 Trivial (kg·m2) SBP 115 ± 10 116 ± 12 1, ±4 Unclear (mmHg) DBP 65 ± 10 67 ± 15 2, ±6 Unclear (mmHg) 3.49 ± 0.60 3.68 ± 0.53 0.19, ±0.19 Possibly beneficial 𝑉̇ O2max -1 (L·min ) 53.5 ± 8.3 56.2 ± 8.2 2.7, ±2.9 Possibly beneficial 𝑉̇ O2max -1 -1 (mL·kg ·min ) TTE 11.0 ± 0.7 11.9 ± 0.5 0.9, ±0.7 Very likely (min) beneficial Peak power 253 ± 39 259 ± 34 6, ±13 Possibly beneficial (W) GET 1.86 ± 0.34 1.95 ± 0.35 0.09, ±0.13 Possibly beneficial -1 (L·min ) GET 53 ± 6 53 ± 7 0, ±2 Unclear ̇ (%𝑉 O2max) Pre- and post-training data are expressed as mean ± SD. BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; TTE, time to exhaustion; GET, gas exchange threshold. Effect, represents the magnitude of the change by subtracting post-training from pretraining. 90% confidence interval (CI), represents the uncertainty of the observed effect. Inference, represents the probabilistic inference that the magnitude of the observed effect is different from the smallest worthwhile change using Cohen’s standardized effect of 0.2 (see methods for details). 24 Table 2. The effect of high-intensity interval training on the steady-state physiological responses during the initial three stages during the sub-maximal exercise test Variable Pre-training Post-training Possibly beneficial 35.8 ± 4.4 Effect, ±90% CI -0.04, ±0.04 -3.3, ±2.37 𝑉̇ O2 (L·min-1) 𝑉̇ O2 (%𝑉̇ O2) Heart rate (beats·min-1) RER 1.34 ± 0.12 1.30 ± 0.14 39.1 ± 5.3 Inference 116 ± 10 111 ± 5 -4, ±7 Unclear 0.91 ± 0.04 0.88 ± 0.06 Likely beneficial -0.03, Likely beneficial ±0.03 EE 6.86 ± 0.56 6.48 ± 0.68 -0.37, Very likely (kcal·min-1) ±0.18 beneficial Fat oxidation 0.21 ± 0.07 0.26 ± 0.12 0.06, Likely beneficial (g·min-1) ±0.06 CHO oxidation 1.27 ± 0.22 1.04 ± 0.33 -0.23, Very likely -1 (g·min ) ±0.14 beneficial Pre- and post-training data are expressed as mean ± SD. RER. Respiratory exchange ratio; EE, energy expenditure; CHO, carbohydrate. See table 1 for a description of the statistical outcomes. 25 FIGURE CAPTIONS Figure 1. Changes in peak power (A), mean power (B) and the fatigue index (C) over the sprints 1-4 in the first (open bars) and last (closed bars) high-intensity interval training session. Where * denotes a meaningful difference between the bout. See the text for details. Figure 2. Changes in the percentage contribution of carbohydrate (closed bars) and lipid (open bars) to total energy expenditure during sub-maximal exercise pre and post high-intensity interval training. See text for details.