Standard 2014 Exit
advertisement

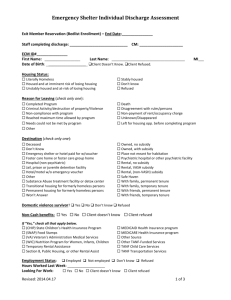
HMIS #: CM Name: Project Entry Date: Santa Cruz County HMIS Standardized Intake: Adult Exit This form is designed to be completed by a service provider while interviewing a client. A separate Standardized Intake form should be completed for each member of the household. Household Information Is client: Single Adult If check Single Adult If checked Adult in Household Adult in Household Child Go to Client Profile Are you the Head of Household (HoH)? Yes No If no, name of HoH: How many adults in household?: How many children in household?: If checked Child If you are in a household, what is your relationship to the HoH? Name of HoH: Self ( head of household) Head of household’s child Head of household’s spouse or partner Other relation to head of household) Other: non-relation member Client Profile First Name Middle Last Name Social Security Number U.S. Military Veteran Form# I500-1-20141001 Yes No Client Doesn’t Know Client Refused 1 of 5 2 Santa Cruz County Standardized Intake HMIS # Reason for Leaving & Destination Reason for Leaving Completed Program Criminal Activity/Violence Death Disagreement with rules/persons Left for housing opportunity Needs could not be met Non-compliance Non-payment of rent Reach max time allowed Other Client Doesn’t Know Client Refused Unkown/Disappeared If Other, Specify: Destination If Other, Specify: Form# I500-1-20141001 Deceased Emergency shelter Foster care or foster care group home Hospital or other non-psychiatric medical facility Hotel or motel paid for w/o emergency shelter voucher Jail, prison or juvenile detention facility Long-term care facility or nursing home Moved from one HOPWA funded project to HOPWA PH Moved from one HOPWA funded project to HOPWA TH Owned by client, no ongoing housing subsidy Owned by client, with ongoing subsidy Permanent housing for formerly homeless persons Place not meant for habitation Psychiatric hospital or other psychiatric facility Rental by client, no ongoing housing subsidy Rental by client, with VASH subsidy Rental by client, with GDP TIP subsidy Rental by client, with other ongoing subsidy Residential project or halfway house with no homeless criteria Safe Haven Staying or living with family, permanent tenure Staying or living with family, temporary tenure Substance abuse treatment facility or detox center Transitional housing for homeless persons Other No exit interview completed Client doesn’t know Client refused Data not collected 2 of 5 3 HMIS # Santa Cruz County Standardized Intake Housing Status Category 1: Homeless Category 2: At imminent risk of losing housing Category 3: Homeless only under other federal statutes Category 4: Fleeing domestic violence At risk of homelessness Stably housed Client Doesn’t Know Client Refused Income and Benefits Information Receiving Income from any source? Yes No Client Doesn’t Know Client Refused Total Monthly Income If not receiving a source below, please put 0 Earned Income $ Alimony or Other Spousal Support $ Child Support $ General Assistance $ Pension or other retirement income $ Private Disability $ Retirement Income from Soc. Sec. $ SSDI $ SSI $ TANF $ Unemployment Insurance $ VA Service Connected Disability $ VA Non-Service Connected Disability $ Workers Compensation $ Other $ , Specify, Receiving Non-cash benefit from any source? Yes Client Doesn’t Know No Client Refused If not receiving a source below, please put 0 Section 8, or other ongoing rent assist.$ Special Supp. Nutrition for WIC $ SNAP (Food Stamps) $ TANF Child Care $ TANF Transportation $ Other TANF-Funded Services $ Temporary Rental Assistance $ Other Source $ , Specify Health Insurance Covered by Health Insurance? Medicaid Medicare State Children’s Health Insurance VA Medical Services Form# I500-1-20141001 Yes Yes Yes Yes No No No No Yes No Client Doesn’t Know Client Refused Employer Provided Health Insurance Heath insurance through COBRA Private Pay health insurance State Health Insurance for Adults Yes Yes Yes Yes No No No No 3 of 5 4 Santa Cruz County Standardized Intake HMIS # Disabilities Disability of Long Duration? Yes Client Doesn’t Know No Client Refused If yes, please complete the following for each disability type Physical Disability Expected to be of long-continued and indefinite duration and substantially impairs ability to live independently? Yes No Client Doesn’t Know Client Refused Documentation of the disability and severity on file? Yes No Client Doesn’t Know Client Refused Currently receiving services/treatment for this disability? Yes No Client Doesn’t Know Client Refused Expected to substantially impair ability to live independently? Yes No Client Doesn’t Know Client Refused Documentation of the disability and severity on file? Yes No Client Doesn’t Know Client Refused Currently receiving services/treatment for this disability? Yes No Client Doesn’t Know Client Refused Expected to substantially impair ability to live independently? Yes No Client Doesn’t Know Client Refused Documentation of the disability and severity on file? Yes No Client Doesn’t Know Client Refused Currently receiving services/treatment for this disability? Yes No Client Doesn’t Know Client Refused Yes No Client Doesn’t Know Client Refused Expected to substantially impair ability to live independently? Yes No Client Doesn’t Know Client Refused Documentation of the disability and severity on file? Yes No Client Doesn’t Know Client Refused Currently receiving services/treatment for this disability? Yes No Client Doesn’t Know Client Refused Developmental Disability Chronic Health Condition HIV/AIDS Form# I500-1-20141001 Yes No Client Doesn’t Know Client Refused Yes No Client Doesn’t Know Client Refused Yes No Client Doesn’t Know Client Refused 4 of 5 5 HMIS # Santa Cruz County Standardized Intake Disabilities, Cont. Mental Health Problem Substance Abuse Yes No Client Doesn’t Know Client Refused No Alcohol Abuse Drug Abuse Alcohol & Drug Abuse Client Doesn’t Know Client Refused Expected to be of long-continued and indefinite duration and substantially impairs ability to live independently? Yes No Client Doesn’t Know Client Refused Documentation of the disability and severity on file? Yes No Client Doesn’t Know Client Refused Currently receiving services/treatment for this disability? Yes No Client Doesn’t Know Client Refused Expected to be of long-continued and indefinite duration and substantially impairs ability to live independently? Yes No Client Doesn’t Know Client Refused Documentation of the disability and severity on file? Yes No Client Doesn’t Know Client Refused Currently receiving services/treatment for this disability? Yes No Client Doesn’t Know Client Refused Employment Currently Employed Yes No Client Doesn’t Know Client Refused Permanent Temporary Seasonal Client Doesn’t Know Client Refused If Employed, hours worked in a week If Employed, Type I (Adult client or Head of Household) certify that the information I have provided here is true/correct to the best of my knowledge. Print Name of Client Signature of Client Date Print Name of Intake Worker Signature of Intake Worker Date Form# I500-1-20141001 5 of 5