CHILD CoC Program_Status and Annual Assessment Form
advertisement

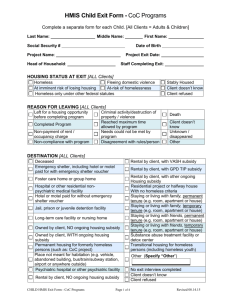
HMIS Child Status & Annual Assessment Form - CoC Programs Annual Assessments are REQUIRED for Adults and Children. Complete a separate form for each Child. [All Clients = Adults & Children] Important: Annual Assessments must be recorded no more than 30 days before or after the anniversary of the client’s Project Entry Date, regardless of the most recent ‘update’ or ‘annual assessment’, if any. Information must be accurate as of the assessment date. *Status Assessments are not required and can be completed at multiple points during project enrollment to track key events (e.g. a change in income and sources)* Last Name: Middle Name: First Name: Social Security # Date of Birth Project Name: Project Assessment Date: Head of Household: Staff Completing Form: PHYSICAL DISABILITY [All Clients] No Client doesn’t know Yes Client refused IF “YES” TO PHYSICAL DISABILITY – SPECIFY Receiving services for physical disability Is the physical disability expected to be of long-continued and indefinite duration and substantially impairs ability to live independently. Documentation of the disability and severity on file No Yes No Client doesn’t know Client refused Client doesn’t know Yes Client refused No Yes No Yes No Yes No Client doesn’t know Client refused Client doesn’t know Client refused Yes No Yes No Client doesn’t know Client refused Client doesn’t know Yes Client refused No Yes DEVELOPMENTAL DISABILITY [All Clients] No Client doesn’t know Yes Client refused IF “YES” TO DEVELOPMENTAL DISABILITY – SPECIFY Receiving services for developmental disability Is the developmental disability expected to substantially impair ability to live independently? Documentation of the disability and severity on file CHRONIC HEALTH CONDITION [All Clients] No Yes Client doesn’t know Client refused IF “YES” TO CHRONIC HEALTH CONDITION – SPECIFY Currently receiving services/treatment for this condition Is the condition expected to be of long-continued and indefinite duration and substantially impairs ability to live independently. Documentation of the disability and severity on file CHILD HMIS Assessment Form - CoC Programs Page 1 of 3 Revised 06.05.15 HMIS Child Status & Annual Assessment Form - CoC Programs HIV-AIDS [All Clients] No Yes Client doesn’t know Client refused IF “YES” TO HIV-AIDS – SPECIFY Currently receiving services/treatment for this condition Is the condition expected to substantially impair ability to live independently? Documentation of the disability and severity on file No Yes No Yes No Client doesn’t know Client refused Client doesn’t know Client refused Yes No Yes No Client doesn’t know Client refused Client doesn’t know Yes Client refused No Yes MENTAL HEALTH PROBLEMS [All Clients] No Yes Client doesn’t know Client refused IF “YES” TO MENTAL HEALTH PROBLEMS – SPECIFY Currently receiving services/treatment for this condition Is the condition expected to be of long-continued and indefinite duration and substantially impairs ability to live independently. Documentation of the disability and severity on file SUBSTANCE ABUSE PROBLEMS [All Clients] No Both alcohol and drug abuse Alcohol abuse Client doesn’t know Drug abuse Client refused IF “YES” TO ALCOHOL ABUSE, DRUG ABUSE OR BOTH – SPECIFY No Currently receiving services/treatment for this condition Yes Is the condition expected to be of long-continued and No indefinite duration and substantially impairs ability to live Yes independently. Documentation of the disability and severity on file No Client doesn’t know Client refused Client doesn’t know Client refused Yes COVERED BY HEALTH INSURANCE [All Clients] No Yes Client doesn’t know Client refused IF “YES” TO HEALTH INSURANCE - HEALTH INSURANCE COVERAGE DETAILS MEDICAID (aka Medi-Cal) Employer Provided MEDICARE Obtained through COBRA SCHIP (Do Not Use) Private Pay Health Insurance VA Medical State Health Insurance for Adults (Do Not Use) CHILD HMIS Assessment Form - CoC Programs Page 2 of 3 Revised 06.05.15 HMIS Child Status & Annual Assessment Form - CoC Programs EMPLOYMENT [All Clients, For Age 16 & Over] Employed: ☐Yes ☐No ☐Don’t know ☐Refused (If yes, Hours worked Last Week: _____) Employment Tenure/Stability: ☐Permanent ☐Temp ☐Seasonal ☐Don’t know ☐Refused If Not Employed, Seeking Employment: ☐Yes ☐No ☐Don’t know ☐Refused EDUCATION [All Clients, For Age 5 & over] Currently Enrolled in School: ☐Yes ☐No ☐Don’t know ☐Refused If Enrolled: Vocational Training or Apprenticeship: ☐Yes ☐No ☐Don’t know ☐Refused Name of school enrolled: ___ __ Is child connected to the HUD homeless liaison: ☐Yes ☐No ☐Don’t know ☐Refused Type of School: ☐Public ☐Parochial or other Private School Highest Educational Level Completed: ☐ ☐ ☐ ☐ ☐ No School Completed Nursery School to 4th Grade 5th or 6th Grade 7th or 8th Grade 9th Grade ☐ ☐ ☐ ☐ ☐ 10th Grade 11th Grade 12th Grade (No Diploma) GED High School Diploma ☐ Postsecondary School ☐ Don’t know ☐ Refused If Not Enrolled: Date of the last enrollment: ___ __ Barrier to Enrolling Child in School: ☐ ☐ ☐ ☐ ☐ ☐ None Residency requirements Availability of school records Birth Certificate Legal Guardianship required Transportation CHILD HMIS Assessment Form - CoC Programs ☐ ☐ ☐ ☐ ☐ ☐ Lack of available preschool program Immunization requirements Physical examination records Other Don’t Know Refused Page 3 of 3 Revised 06.05.15