Achieve Psychological Services

A S
Professional
Psychological Services
Phone: 8678 0946
Offices at: Marayong, St Marys
Parramatta, Wetherill Park
Email: project@professionalpsychologicalservices.com.au
ABN: 84 549 651 536
Achieve a Better Quality of Life Project
Referral Form
Client Information
First Name
Last Name
DOB
Address Line 1
Gender
Address Line 2
Postcode Contact Number
Referrer Details (if applicable)
Name
Relationship to client Service
Contact Number Email
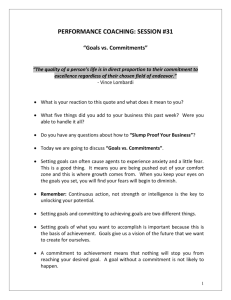
“Achieving A Better Quality of Life”
Services/Health Professionals Client Supported by (if different to referrer)
Name
Relationship to client Service
Email Contact Number
Name
Relationship to client
Contact Number
Service
Mental Health History
Diagnosis
Date of diagnosis
Brief summary of mental health history/current presentation
“Achieving A Better Quality of Life”
Physical Health History
Do you/client experience or have a history of any of the physical health concerns listed:
Diabetes
Epilepsy
Asthma
Blood pressure issues
Dental/hearing/eyesight issues
Mobility issues
Weight concerns
Traumatic brain injury
Cognitive deficits
Past physical trauma
Blood disorder
Other
Allergies
Please provide any necessary details of above concerns:
“Achieving A Better Quality of Life”
Overview
Do you/client have a history or currently experience any of the concerns listed below. Please answer these questions as accurately as possible.
Suicidal ideation
Suicide attempts
Self harm ideation
Self harm
Physical/verbal aggression
Psychosis/mania
Substance use
Please provide any necessary details of above concerns:
“Achieving A Better Quality of Life”
Consent
I _________________________ give my consent for the health professionals and referrer nominated in this form to be contacted during the referral process.
__________________________ ______________________________ _____________
Client’s Name Signature of Client or Legal Guardian Date
__________________________ ______________________________ _____________
Witness Name Signature of Client Date
Please attach paper to back of form if more space needed for any questions
“Achieving A Better Quality of Life”