Pathway for the treatment of skin that is damaged and excoriated by
advertisement

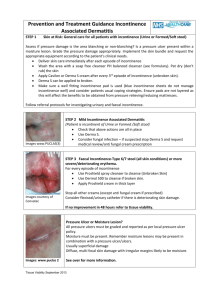
Pathway for the treatment of skin that is damaged and excoriated by moisture First Line management should be good skin care with Emollients i.e Hydromol. This pathway is to be used as a step up after primary emollient therapy has been proved to be ineffective. These guidelines are secondary to establishing and addressing the cause of the incontinence / excoriation Do not use soap to cleanse skin in this area, use Hydromol as a soap substitute. Continence pads must be worn on the body, not laid underneath the patient. Do not use blue incontinence sheets for moisture prevention. The creams below are indicated for use with continence products and do not block the pad absorbability. Skin Type Clinical intervention Product Patient has incontinence or has an excessive sweating problem. Healthy, intact skin but patient has been assessed as ‘at risk’ of skin damage secondary to moisture. No erythema. Prevention : Maintain skin hygiene and emollients Replace pads when indicated. Establish & address the cause of the incontinence. Only consider barrier product if patient has been assessed as at risk. MEDI DERMA S barrier cream 2g Sachet (x20) Tube 90g Skin is moist with diffuse erythema. There is Superficial skin damage present. This is not associated with pressure. 1st line -Cleanse using hydromol as a soap substitute after every episode of incontinence. Medi derma S barrier film 1ml & 3ml foam applicators Large surface areas and painful moisture lesions use Medi derma S spray 50mls (see guidance ) If this fails to work: 2nd line -apply barrier preparation after every 3rd wash Manage cause of skin breakdown. If unable to manage incontinence seek advice and support from bladder &bowel service Refer to TV to aid management of skin. Pathway for the treatment of skin that is damaged and excoriated by moisture by moisture/tissue Viability/Jan’16/V4 Peri wound skin is white waterlogged /macerated due to poor management of exudate Spreading erythema. Extensive excoriation. Up to 50% of affected skin is broken. Oozing / bleeding may be present. High bacterial load is usually present. There may be fungal involvement. Deeper ulceration which has not been managed by above treatments OR complex patient and wound factors which cannot be resolved and has the potential to deteriorate. Address underlying causes such as oedema or infection Check appropriate absorbent pad is being used (for mod to high levels of exudate this should be Sorbion S ) Consider frequency of dressing changes Apply barrier film at every dressing change after the limb has been washed Medi derma S Barrier film Foam applicators 1ml and 3ml sizes Skin has been assessed as excoriated due to urine /faeces Skin is in an inflammatory stage or has a high bacterial load but not infected Medihoney barrier cream Sachets –2g Tube -50g (Indicated for treatment of mild fungal infection). N.B.If peri wound skin is excoriated due to high bacterial load then consider Medihoney barrier cream If gross fungal infection consider antifungals. Do as above Exclude any issue with pressure damage Proshield Plus PIP-359-8760 Ensure you use the Proshield foam and spray cleanser (pip-359-87520) for the removal of proshield plus (Proshield is on the restricted formulary please contact TV for support). Pathway for the treatment of skin that is damaged and excoriated by moisture by moisture/tissue Viability/Jan’16/V4