3c. Hep AE Service Development Protocol
advertisement

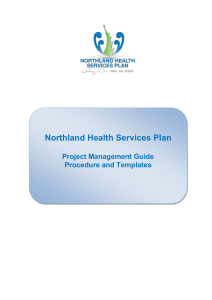
Exploring the socio-demographic characteristics associated with frequent attendance at Accident and Emergency departments in Lambeth. Summary Rising levels of Accident & Emergency attendances is a national problem with up to 20% of visits resulting in advice or guidance only, at an annual cost to the NHS of approximately £136 million. Research has shown that socio-demographic factors such as deprivation, ethnicity, and population morbidity and mortality are associated with high use of A&E. This is a particular challenge in Lambeth, the 14th most deprived of England’s 354 Boroughs, with a high proportion of residents from Black and Ethnic Minority (BEM) groups, multiple languages, and a lower life expectancy than the national average. However, many GPs in Lambeth feel that, in addition to the above factors, there are groups of patients with particularly high use of A&E services. Identification of such ‘clusters’ of characteristics requires patient-level data from both primary care and hospital A&E. The local collaboration of GP practices, Public Health, and researchers in Lambeth, the Lambeth Datanet (LDN), with it’s collection of detailed socio-demographic characteristics (ethnicity, language, religion) embedded within the GP clinical record, brings a unique opportunity to undertake this. This project will link GP clinical data (LDN), GP consultation data, and Hospital Episode Statistics (HES) A&E data at individual patient level in a secure NHS environment, the Clinical Data Linkage Service (CDLS) at the South London and Maudsley (SLaM) NHS Trust. After linkage the data, with all patient identifiers removed, will be made available to analysts, who will undertake cluster analysis. As the presence of Long-term conditions (LTCs) and practice characteristics will both influence the rate of A&E attendance, these will be controlled for in the analysis. A health economic analysis will also be performed. This project will inform service commissioning and redesign to develop cost-effective care tailored to patient need. 1 Background The role of Accident and Emergency Departments is to assess and treat patients with serious injuries or illnesses (1). It has been estimated that up to 20% of A&E visits (approximately 2 million annually) result in advice or guidance only (2). Each A&E attendance costs the NHS an average of £111: an emergency ambulance call costs an additional £455. In comparison, a GP attendance costs £32 (3). The annual cost of ‘unnecessary’ attendances in England has been estimated at £136 million (4). Research has shown that several socio-demographic and clinical factors are associated with high frequency of attendance at A&E departments i.e. socio-economic deprivation (5-9), ethnicity (5, 7, 10, 11), population morbidity and mortality (5-10), population rates of unhealthy behaviours e.g. smoking (6, 8, 10, 12) and urban / rural status (7, 8). The age profile of the population is important. Several studies have found statistically significant associations between A&E attendances and different age groups, although findings have been conflicting; with some reports and studies showing higher rates in children and young adults (9, 13-15) and others showing higher rates in older people (5), although there is evidence that this high rate of attendance may simply reflect higher need, with older people actually using emergency services more appropriately than those in younger age groups (16). Primary care factors seem to be important; quality of care as indicated by practice score on the Quality Outcomes Framework (6, 10, 12, 17), access to primary care services and/or GPs (5-8), and size of practice (9). A recent study has also shown that patient understanding of how to access non-A&E sources of out of hours care is also significant (9). Lambeth is the 14th most deprived of England’s 354 Boroughs, with a high proportion of residents from Black and Ethnic Minority (BEM) groups (18). Multiple languages are spoken; with nearly 50% of the population speaking languages other than English, with many being unable to converse in English (19). Lambeth has a lower life expectancy than the national average, with the gap being explained by premature deaths in Cardiovascular disease, Cancer and Respiratory Disorders, and infection (particularly HIV). The combination of high prevalence of long-term conditions, socio-economic 2 deprivation and multiple languages provides challenges in providing care tailored to patient need, and a high rate of attendance at A&E. The studies described above have explored population and practice characteristics by exploring associations with A&E attendance rates, with characteristics explored separately (univariable analyses) and with multiple characteristics explored together (multivariable analyses) using national or local data at general practice, trust, regional or national level. Whilst such studies can help in allocation of health service resources to match patient demand, they do not address the fact that individuals, families and communities will have ‘clusters’ of characteristics, and that there may be some clusters of characteristics that explain an additional proportion of the variation. If such clusters of characteristics do explain an additional proportion of the variation in A&E attendance, they could form the basis of new approaches to service redesign, exploring with communities how the NHS could provide them with more cost-effective care options for conditions not requiring A&E attendance on clinical grounds. Analysis to identify such clusters, however, requires data to be available at individual patient level. Data to be used in this project Lambeth Datanet. Lambeth has the data required to such an analysis. Since 2000, a broad profile of patient characteristics (ethnicity, language preference, religious affiliation, country of birth) have been collected and entered into GP clinical records throughout Lambeth practices, forming the Lambeth Datanet (LDN). This covers 49 of the 50 General Medical Practices in Lambeth; the one excluded practice having an incompatible clinical information system. LDN enables the linkage of patient profile and clinical data, which are then extracted for analysis. GP consultation data. These data will be extraction directly from the GP clinical systems in Lambeth practices. Quality and Outcomes Framework data The Quality and Outcomes Framework (QOF) is a system of performance indicators for primary care services. The system was introduced in 2004 as a way of measuring the quality of provision of primary care services, and for providing a mechanism to reimburse GPs, according to the quality of the services provided (20). The framework 3 has evolved since it’s inception and now consists of indicators across four domains: clinical, public health, quality and productivity, and the patient experience (17), National Accident and Emergency data. The national Hospital Episode Statistics (HES) data are collected centrally by the NHS at individual patient level. Data include all episodes of attendance at any A&E department in England since 2007. In this project, these sets of data will be linked. LDN, GP consultation and HES data will be linked using a pseudonym. The pseudonym is a 1-way encrypted NHS number generated before transfer of data to the secure data linkage site, the Slam Clinical data Linkage Service (CDLS); a national exemplar for secure storage and linkage of patient data. QOF data will be added by CDLS using the General Practice identifier of the General Practice with which the patient is registered. Aims of this project. The primary aim of this project is to use an LDN-HES linked dataset to explore weather there are ‘clusters’ of socio-demographic factors statistically significantly associated with a higher rate of A&E attendance, controlling for patient morbidity and General Practice characteristics. Secondary aims are (a) to explore any differential impacts of mental health LTCs (SMI, dementia and depression) vs. physical LTC on A&E attendance rate and (b) to explore the health economic implications of the study findings. Method Data flow and generation of dataset for analysis The proposed data flow is shown in figure 1. 4 Figure 1: Project data flow12. Step 1 and 2 Step 2 QMS QMS: LDN data extraction incl NHS number (NHSN) & practice ID CCG: Consultation data extraction incl NHSN QMS: NHS pseudonym created for each patient record (NHSP) in LDN & consult datasets + practice ID Step 3 and 4 NHSN encryption algorithm LDN data + NHSP, Consult data + NHSP, practice information Step 5 Health and Social Care Information Centre (HSCIC) QMS CDLS HSCIC A&E NHSP + A&E Data LDN NHSP LDN NHSN CDLS LDN NHSP Step 6 1 A&E NHSN A&E data inclu ding LSOA Step 6 HSCIC LDN NHSP 2 CDLS A&E data CDLS CDLS LDN NHSP 1 LDN data + practice data + IMD (from LSOA) LDN A&E Project data Specific Anonym For explanation of abbreviations used see page 11. Exact details of data flow may be subject to change following CAG advice and approval (through s251). 2 5 Details of Data Flow Step 1: Lambeth Datanet (LDN) data for all Lambeth patients registered with 49 of the 50 Lambeth practices, including NHS number but no other Patient Identifiable Information (PII) are extracted from GP practices by QMS Contract Focus (QMSCF), a private IT company contracted by Lambeth CCG to extract LDN data for Public Health and clinical care improvement audits. Annual GP consultation rates plus NHS number are extracted by the CCG. QMSCF apply the same 1-way encryption algorithm to the NHS number in both the LDN and GP consultation data creating a unique patient level pseudonym (NHSP). Step 2: LDN data and consultation data (including NHSP) are transferred to the South London and Maudsley (SLaM) Clinical Data Linkage Service (CDLS). There is no transfer of any PII other than the NHSP. Other data included at patient level in this transfer are practice national identifier code, demographic data and clinical data. Practice national identifier code is required as practice characteristics are a predictor of A&E usage, so must be controlled for in the analysis. GP practice list size in Lambeth ranges from 3,060 to 18,698 (median 6,888), meaning the risk of patient identification brought by inclusion of the practice identifier is low. Demographic data are ethnicity (16+1 format), religion, language, and country of birth. Clinical data are whether or not patients are on Quality and Outcome Framework (QOF) registers; Coronary Heart Disease, Stroke/TIA, Diabetes, CKD, Hypertension, Atrial Fibrillation, Heart Failure, Peripheral arterial disease, asthma, hypothyroidism, Chronic Obstructive Pulmonary Disease, Cancer, epilepsy, osteoporosis, rheumatoid arthritis, palliative care, depression, Serious Mental Illness (SMI), dementia, Learning Disability (LD), number of medications issued in previous year and practice data e.g. list size, number of GPs, Practice Quality and Outcome scores for clinical, public health, quality and productivity, patient experience domains. Step 3: CDLS will send NHSP (only) to HSCIC. Step 4: QMSCF will send the NHS number encryption algorithm (including SALT) to HSCIC. Step 5: HSCIC transform the NHS numbers of patients within the A&E data set, using the encryption algorithm provided by QMSCF. This creates a patient level pseudonym (NHSP) in an identical format to that created for the LDN NHS numbers. All A&E records containing the same pseudonym (NHSP) provided by CDLS are then extracted. 6 Step 6: HSCIC send A&E data with NHSP to CDLS. A&E data are: Arrival mode (ambulance, other), Attendance category (first, follow-up (planned, unplanned)), Attendance disposal (discharged home, admitted, died), department type (A and E, walk-in centre), Source of referral (e.g. self-referral, GP), Arrival date, Arrival time, Clinical diagnosis (A&E diagnosis, includes not classifiable and nothing abnormal detected), Clinical investigation (e.g. blood tests, X rays), A&E treatment (e.g. dressing, sutures, none), Dominant procedure (the procedure with the greatest impact on resources), Country of residence, CCG of residence, Lower Super Output Area (LSOA), Provider code (3 & 5 digit) (identifies the Trust or PCT ), PCT of responsibility, GP Practice, Age on arrival. No Patent Identifiable Information other than NHSP will be transferred to CDLS by HSCIC. Step 7: CDLS will host A&E data and LDN clinical data, the records of which are linked using the NHSP (pseudonymised NHS number) as a common unique identifier. CDLS will add Index of Multiple Deprivation (IMD) scores using patient LSOA. Step 8: CDLS will control and manage access to linked data in accordance with a security protocol agreed with Lambeth CCG. Step 9: CDLS will replace all NHSP with a project specific anonym before transferring any data extract outside of CDLS. Method of analysis Stage 1. Multilevel modelling will be undertaken to explore which variables predict high rates of attendance at A&E. The variables included will be (a) practice characteristics (b) presence of one or more Long-term Conditions (LTC) and (c) patient socio-demographic characteristics. Stage 2: Cluster analyses will be used to explore whether there are any clusters of sociodemographic variables that are associated with high rates of attendance at A&E. Stage 3: It can be hypothesised that physical, mental health LTC and LD might have differing associations with the rate of A&E attendance. A sub-analysis will explore this. The physical LTCs to be explored are Coronary Heart Disease, Stroke/TIA, Diabetes, CKD, Hypertension, Atrial Fibrillation, Heart Failure, Peripheral arterial disease, asthma, hypothyroidism, Chronic Obstructive Pulmonary Disease, Cancer, epilepsy, osteoporosis, rheumatoid arthritis, palliative care. The mental health LTCs to be explored are depression, Serious Mental Illness (SMI), and dementia. 7 Stage 4: Health service cost data will be calculated using the national tariff, and the health economic associations of any associations found will be described. Analysis team Dr Gill Rowlands, Clinical Senior Lecturer, King’s College London Mr David Whitney, Lambeth Datanet data manager and analyst, King’s College London Prof Paul McCrone, Health Economist, Institute of Psychiatry, King’s College London. Information Governance and Ethics The research team will apply to the Lambeth CCG Information Governance Committee for approval for the project. In addition, s251 approval will be requested from the HSCIC. Lambeth CCG, CDLS and the research team will develop an agreement on data storage and access3. A written contract will be developed between CDLS and the Lambeth CCG Data Controller, making explicit the legal Terms and Conditions. As the data released to the research team will be anonymised and this is a service development project, ethics approval is not required. The research team will get written confirmation of this from the National Research Ethics Committee. Project outcome(s) 1. A detailed understanding of the socio-demographic factors associated with high and very high rates of attendance at A&E departments by Lambeth patients. 2. Identification of any ‘clusters’ of socio-demographic factors that are statistically significantly associated with a higher rate of A&E attendance. Upon request, SLaM ICT will also provide a work space within the SLaM firewall for research users to hold data extracts and work on data analysis. This would ensure overarching SLAM ICT Security and IG framework is applied to secondary data (linked datasets compiled by and extract from CDLS) as well as dataset stored within CDLS. In this case, all users will require SLAM network accounts and ICT Service Desk support (e.g. disk space, software licences, remote access capability etc.) 3 8 Future work arising from this project If this project does show clusters of socio-demographic characteristics associated with high use of A&E services, this could form the basis for a social marketing approach to gain a better understanding of the drivers of high frequency of attendance at A&E and/or low frequency of using alternative, more cost-effective, options for emergency care for those not requiring A&E attendance on clinical grounds. This approach has been successfully used to optimise health promotion campaigns by tailoring messages to the needs and characteristics of segments of the population with identifiable characteristics (21), and could be applied to inform service redesign for emergency services in Lambeth. 9 Abbreviations Abbreviation A&E CCG CDLS HES LDN LSOA PII QMS QOF Full name Accident and Emergency Departments Clinical Commissionin g Groups Clinical Data Linkage Service Hospital episode statistics data Lambeth Datanet Lower Super Output Area Patient Identifiable Information Quality Medical Solutions Quality and Outcomes Framework S251 SLaM South London and Maudsley GP Practice data notes Official groups including GPs and managers who purchase hospital services on behalf of the patients Data linkage service based in SLaM with experience in secure clinical data management and linkage Data on every contact every patient has with English hospitals. The record of every patient registered with a GP in Lambeth. Includes personal details (age, sex, ethnicity, language, religion) and clinical data. Area in which patient lives, at the level of 15,000 per LSOA details such as name, address, date of birth, NHS number that enables identification of individuals current provider for Lambeth CCG for clinical data extraction Payment by results scheme for GPs This is a process to allow linkage of two or more sources of patient data. Approval is obtained by submission of a request to the CAG. S251 approval is not automatically required for data linkage for service development work; however the project team has been advised that, given the nature of the proposed project, the HSCIC will require s251 approval before releasing the HES data Specialist Mental Health NHS trust Data held by CCG on practice: list size, number of GPs, sex of GPs, languages spoken by GPs 10 References 1. Emergency and urgent care services: A&E: NHS Choices; [8 August 2013]. Available from: http://www.nhs.uk/NHSEngland/AboutNHSservices/Emergencyandurgentcareservices /Pages/AE.aspx. 2. Emergency admissions to hospital: managing the demand. London: National Audit Office, 2013 31 October. Report No. 3. Williams N. Delivering value for the NHS: NHS Direct; 2009 [8 August 2013]. Available from: http://www.northwest.nhs.uk/document_uploads/Emergency Care Review September Event/Working together - delivering value.pdf. 4. Reducing needless A&E visits could save NHS millions: The Co-operative group; [8 August 2013]. Available from: http://www.cooperative.coop/corporate/Press/Press-releases/Pharmacy/Reducing-needless-AEvisits-could-save-NHS-millions/. 5. Bankart MJG, Baker R, Rashid A, Habiba M, Banerjee J, Hsu R, et al. Characteristics of general practices associated with emergency admission rates to hospital: a crosssectional study. Emerg Med J 2011;28(7):558–63. 6. Calderon-Larranaga A, Carney L, Soljak M, Bottle A, Partridge M, Bell D, et al. Association of population and primary healthcare factors with hospital admission rates for chronic obstructive pulmonary disease in England: national cross-sectional study. Thorax. 2011;66:191-6. 7. Purdy S. Avoiding hospital admissions. What does the research evidence say? London: King's Fund, 2010. 8. Purdy S, Griffin T, Salisbury C, Sharp D. Emergency admissions for coronary heart disease: a cross sectional study of general practice, population and hospital factors in England. Public Health. 2011;125(1):46-54. 9. Scantlebury R. Socio-Economic Deprivation and Accident and Emergency Attendance Rates - Characteristics of Primary Care which can Mitigate this Relationship: King’s College London; 2013. 10. Dusheiko M, Doran T, Gravelle H, Fullwood C, Roland M. Does higher quality of diabetes management in family practice reduce unplanned hospital admissions? Health Serv Res. 2011;46(1 ):27–46. 11. Saxena S, George J, Barber J, Fitzpatrick J, Majeed A. Association of population and practice factors with potentially avoidable admission rates for chronic diseases in London: cross sectional analysis. J R Soc Med. 2006;99:81–9. 12. Soljak M, Calderon-Larrañaga A, Sharma P, Cecil E, Bell D, Abi-Aad G, et al. Does higher quality primary health care reduce stroke admissions? A national cross-sectional study. Br J Gen Pract. 2011;61(593):e801–7. 13. Shah SM, Cook DG. Socio-economic determinants of casualty and NHS Direct use. Journal of Public Health. 2008;30:75-81. 14. Hospital Episode Statistics: Accident and Emergency Attendances in England (Experimental Statistics) 2011-12 2013. 15. Hendry SJ, Beattie TF, Heaney D. Minor illness and injury: factors influencing attendance at a paediatric accident and emergency department. Archives of Disease in Childhood. 2005;90:629-33. 16. Gruneir A, Silver MJ, Rochon PA. Emergency department use by older adults: a literature review on trends, appropriateness, and consequences of unmet health care needs. Medical Care Research and Review. 2011;68:131-55. 17. Quality and Outcomes Framework guidance for GMS contract 2013/14. Mar 2013. 18. State of the Borough. London: Lambeth First, 2011. 11 19. Annual Public Health Report 2008 - 2009. Health inequalities in Lambeth Review of progress. London: NHS Lambeth, 2009. 20. Ashworth M, Armstrong D. The relationship between general practice characteristics and quality of care: a national survey of quality indicators used in the UK Quality and Outcomes Framework, 2004-5. BMC Family Practice. 2006;7:68. 21. Smith A, Humphreys S, Heslington L, La Placa V, McVey D, MacGregor E. The Healthy Foundations Lifestyle segmentation. Research report no. 2: The qualitative analysis of the motivation segments. . Department of Health (England): 2011. 12