PEG "Feeding" Tube
advertisement

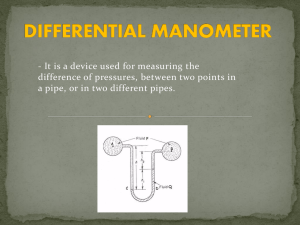
PEG "Feeding" Tube By gi health Percutaneous Endoscopic Gastrostomy (PEG) Most of us don't really appreciate something until it is taken away. It is a natural situation. A good example is swallowing. You never give it a second thought. Why should you? You have been swallowing food and liquids since you were a baby - all without thinking about it. But, then one day, you have a stroke or develop some other terrible problem that interferes with your ability to swallow. Suddenly, swallowing becomes the most important thing in the world. Without it, you can not provide your body with the raw materials it needs to function normally. In a short time, you would either die of dehydration or succumb to malnutrition. Until the problem is corrected, you need some way to bypass the foodpipe so you can be fed without swallowing. A Tube Down the Nose The need for supplemental feeding was recognized as early as ancient Egypt and Greece when nutrient enemas containing milk and wine were given to treat diarrhea. Of course, this didn't work well because the colon can't really aborb much nutrition - only water. In 16th century Venice, tubes were fashioned from animal bladders to pass nutrient solutions down the throat. Eel skin was tried for the same purpose in the 18th century. But it was not until the 19th century, that the use of the nasogastric tube (a thin tube passed through one nostril and down the esophagus to reach the stomach) became widespread. The use of these so-called "NG tubes" revolutionized supplemental feeding to seriously ill patients. Up to 3000 calories a day could be slowly given through an NG tube. Patients with recoverable strokes now could live long enough to regain their swallowing function. However, despite their usefullness, most individuals can not tolerate a tube in their nose for any length of time. Eventually, this causes a sore nose and throat. Nosebleeds are common. Sick and confused patients often will pull the tube out prematurely. There had to be a better way. Surgery - Making a Doorway into the Stomach Over the past 50 years, different surgical techniques have become available to create an opening (fistula) in the wall of the abdomen directly into the stomach "pouch." This allows food and fluid to be delivered directly into the stomach without going down the esophagus at all. These procedures were called surgical gastrostomies and worked well. However, they required general anesthesia in an operating room and an abdominal operation. Critically ill patients who needed nutritional support often could not tolerate the stress of the operation. The complication rate was significant. Again there had to be a better way. Percutaneous Endoscopic Gastrostomy (PEG) In 1980, Dr. Jeffery Ponsky in Cleveland Ohio developed new non-operative technique called Percutaneous Endoscopic Gastrostomy, commonly called "PEG." Percutaneous means "going through the skin. So, this feeding tube bypasses the mouth and esophagus by passing through the skin and muscle of the abdominal wall directly into the stomach. This technique can be done without the need for general anesthesia or a major abdominal incision. It is usually performed by a surgeon with the assistance of a gastroenterologist. Using a gastroscope to guide placement, a tunnel can be created between the skin and the stomach with only a 1/2" incision. PEG is particularly well suited for patients who have an increased risk for surgery. It can be performed in less than 30 minutes, requires minimal sedation rather than general anesthesia, can be accomplished at the bedside, if necessary. PEG has a low complicaton rate and is successful in over 95% of cases. Both patients and nurses prefer PEG over NG tubes. In fact, by 1990, PEG had largely replaced the open surgical gastrostomy procedure which is now seldom performed. How is a PEG performed? Usually, a team approach is used with a general surgeon and gastroenterologist working together. The procedure usually takes less than 30 minutes. After receiving a dose of antibiotic intravenously, the patient is given a dose of sedation. The surgeon disinfects the skin over the abdomen with an antiseptic solution. The gastroenterologist then performs a gastroscopy examination by passing the videogastroscope into the mouth and down the esophagus and into the stomach. After verifying that no serious stomach disease is present, the room lights are dimmed and the stomach inflated with air. As the stomach expands the wall of the stomach is compressed against the inside of the abdominal wall. Where the stomach and the abdominal wall touch, you can actually see the light from the video camera inside the stomach. Usually this spot is located slightly to the left of the abdomen and just below the ribs. This is the site for tube insertion - where the stomach and the abdomen are closest together. Once the site is chosen, the surgeon injects a small amount of local anesthetic and inserts a long thin needle through the numb spot and into the stomach. The gastroenterologist is able to see the tip of the needle enter the stomach from the outside and surrounds it with a wire snare. A soft thin wire is passed into the needle from the outside and is captured by the gastroscope snare. As the scope is withdrawn, the string is pulled out the mouth. At this point, you have a thin wire going into the front of the abdomen into the stomach and upward out the mouth. The tapered tip of the feeding PEG tube is attached to the wire. As the wire is pulled out from the abdomen by the surgeon, the PEG tube is pulled down the the esophagus and the tapered tip comes out the incision from inside the stomach. The inner end of the tube has a soft round "bumper" to keep the tube from coming all the way out. The outer portion of the tube is secured. Antibiotic ointment is applied and the area covered by a bandage. When the procedure is done, you have a hollow feeding tube going into the front of the abdominal wall and into the stomach. The inner bumper keeps the tube from falling out. After the first day, liquid food can be injected several times a day by a syringe (bolus feeding) into the stomach. One can also be fed through the tube using a continuous infusion and pump. What goes into the tube? Liquid nutritional formulas are put into the tube and directly into the stomach - bypassing the disturbed swallowing function. These solutions can provide complete nutrition. Common solutions are Jevity, Ultracal, Osmolite, and Ensure. The doctor and dietitian usually work together to determine which formula is best for each individual, and how much formula will be needed to meet that patient's nutritional needs. In addition, water and medications can be given through the tube. When is a PEG useful? PEG tube placement is used either to put something in the stomach or take something out. The most common use is to provide access to the stomach for long-term nutritional support. Patients in this group often have neurologic disorders such as a stroke or a tumor of the head, neck, or esophagus. Stroke patients with difficulty swallowing treated by PEG feedings had significantly improved outcomes in terms of nutritional status, mortality, and hospital discharge when compared with patients fed via nasogastric tubes. PEG for Decompression Nutritional support is the most common indication for PEG placement. Decompression is the second. In this instance, the PEG tube is connectedd to a suction device to decompress a distended stomach. This is usually performed on patients requiring long-term decompression. These would include those with conditions such as diabetic stomach paralysis (gastroparesis); intestinal pseudo-obstruction; or mechanical obstruction due to malignancy, surgery, or other disease processes. Using a PEG tube istead of a chronic nasogastric tube may improve the quality of life and simplify care in these settings. Who Should Not Have a PEG? PEG placement is not for everybody. It is still a surgical procedure with some risk and best serves those with a reversible problem or long term need for nutritional support. Poor candidates for a PEG would include: The main reason not to put in a PEG tube is the inability of the stomach wall and abdominal wall to come together. Safe PEG placement depends on the doctor being able to inflate the stomach so that it is tight against the inner abdominal wall. Only then can a safe needle puncture through the skin and directly into the stomach pouch be performed. Patients with a terminal illness. It is not appropriate to use a PEG tube in those with a limited life expectancy. They can be treated with a NG tube or thin feeding tube inserted through the nose. Patients with a tight blockage of the esophagus. A PEG obviously can't be done if the gastroscope cannot be passed through the esophagus into the stomach. This might happen in a case of a very narrow esophagus from cancerous invasion. Patient with a blockage of the digestive tract can not be fed through a PEG tube - although a PEG is sometimes used in the circumstance to help deflate a blocked and swollen stomach. Patients with peritonitis - a serious infection within the abdomen sometimes caused by a ruptured organ like the appendix. (This can also result from premature PEG tube removal.) Patients with severe liver failure and massive abdominal fluid collection (ascites) Patients with poor blood clotting either from liver disease, a blood disorder, or due to a "blood thinner" such as Coumadin blood thinners. Clotting disorders must be corrected before PEG placement can be done. Patients with kidney failure on peritoneal dialysis Patients with a deformed stomach usually from a large large hiatal hernia or prior stomch surgery Patients who are morbid obesity - over 100 pounds overweight. Patients with stomach cancer if the cancer is directly in the path of the PEG tube or if the cancer blocks the drain of the stomach (pylorus). When Can Feedings Be Started After PEG Placement? Typically, the patient is kept NPO (no food or drink by mouth) for 24 hours and vital signs are carefully monitored. The patient is also assessed for bleeding and leakage at the PEG site. After this interval, PEG feedings can be initiated. What are the possible dangers? In general, this is a relatively safe procedure. Over the past 20 years, many thousands of PEG placements have been performed in the United States and the rate of major complications has been low, about 3%. Considering that these are usually very ill individuals that is considered to be an acceptable risk. Of course, when a complication does occur, the outcome is usually not good. These are sick weak patients and about one quarter with complication die. Possible complications include heart or lung failure during the procedure, peritonitis infection, bowel perforation, internal bleeding, choking on vomitus, tube dislodgement, and infection at the insertion site. Sometimes the internal bumper will wear away the stomach lining causing a bleeding ulcer. Peritonitis carries a high risk of death and usually occurs when the PEG tube is inadvertanley pulled out by the patient in the first few weeks before it has healed internally. Frequently Asked Questions (FAQ) 1. How do I unblock the tube? Rinsing tubes with water before and after feedings will prevent most blockages. If the formula, water, or medication will not go in, first check that the tube is not kinked. Occasionally, the tube will be blocked by residues from formula or medication. To remove the blockage, place a syringe into the blocked tube. Gently pull back on the plunger to remove the blockage. If the blockage remains, use the syringe to instill water into the tube. The tube may also be milked with the fingers. Place one hand holding the tube securely at the stoma. With the other hand run your thumb and forefinger down the tube to remove the blockage. If both methods fail, call the patient's doctor or health care provider. 2. What if the tube is pulled out? Confused patients may try to remove the tube. It is very important NOT to pull out the tube in the first week after PEG tube placement. Serious complications could occur. But, once the tract has healed, there is not much risk in removal of the tube. The opening in the abdominal wall will probably leak for a few day and then eventually seal itself - much like a pierced ear. If the patient pulls at the tube, do not panic. Cover the opening with a small, light dressing and call the patient's doctor. Patients may be outfitted with bulky mittens (or a one-piece outfit for infants) to prevent removal. 3. What if the stoma looks infected? Once the initial healing takes place infection of the stoma is uncommon. Clean the area several times a day as prescribed. If signs of skin irritation (redness, soreness, pain, swelling, unusual drainage) persist, call the patient's doctor or health care provider. 4. What if there is leakage at the stoma? Leakage may occur because the tube has pulled away from the abdominal wall or because the stoma site is enlarged. If the stoma site has enlarged, the doctor may need to replace the tube. Report to the doctor or health care provider if the leakage does not stop. 5. What if the feeding tube becomes disconnected? If the feeding tube becomes disconnected, estimate the amount of formula lost, reattach the feeding tube, and continue feeding, adding the estimated amount of lost formula. 6. What if the tube is shorter or longer than usual? The length of the tube when originally placed is noted. Ask the patient's doctor or health care provider about marking the tube where it should be located. The tube should have a small amount of "play," but if the tube has become longer or shorter than the original length by more than the number of inches noted, it may be migrating (moving). A shorter tube may be cause blocking or aspiration. A longer tube may cause damage to the stomach lining. Call the patient's doctor or health care provider if there is a significant change in the tube's length. 7. What feeding solution is used? There are many nutritional supplements on the market that can be given through the PEG tube. Ask the patient's doctor or health care provider which one they recommend for that particular patient. One commonly used solution is Jevity Plus, a high-nitrogen and fiber-fortified liquid formula, provides complete, balanced nutrition for patients who can benefit from slightly increased protein and calories. The fiber blend and special sugars help maintain digestive tract health and restore the balance of digestive tract flora. Available in 8-fl-oz cans (aboout 300 calories) and convenient prefilled tube-feeding containers (1,000 and 1,500 milliliters). Another commonly used product is Ensure with fiber. 8. How much feeding solution is given? Every patient and situation is different. Some patients can't eat at all and depend completely on the feeding tube for all of their nutrition. They may receive as much as 8 cans a day (2400 calories). Other just need a little help and require less. Ask the patient's doctor or health care provider how much feeding solution to administer and how often. 9. Can the patient still eat and swallow once the PEG feeding tube is inserted? Again every patient and situation is different. Some patients can't swallow at all because of thoat cancer or a stroke. They can not eat normally. But if the patient can still swallow without choking, there is no reason why food can not be taken by mouth in addition to the lquid supplement give through the PEG tube. Still Popular Twenty Years Later Percutaneous Endoscopic Gastrostomy (PEG) is simple, safe, and cost-effective technique for placement of feeding tubes in the GI tract. It has stood the "test of time." Over the past 20 years, PEG has remained the benchmark against which all other methods of nutritional support must be measured. The consistently high success rates, relative safety, and high patient and nursing satisfaction make it superior to surgical gastrostomy.