Trinity Washington University 125 Michigan Ave. NE Washington
advertisement

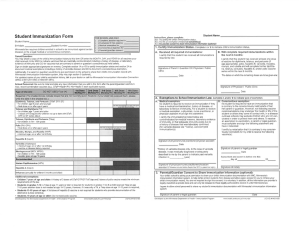
Trinity Washington University 125 Michigan Ave. NE Washington, DC 20017 202-884-9615 Health and Wellness Center Immunization Record This for must be completed by your health care provider in order to register for classes REQUEST FOR MEDICAL OR RELIGIOUS EXEMPTION Religious exemption is allowed if the responsible person objects in good faith and in writing that the immunization violates her religious or ethical beliefs. Medical exemption is allowed if a physician or health care provider deems an immunization medically inadvisable. Students who wish to be exempt due to religious or medical reasons must submit a letter from a medical provider or religious clergy which states the need for exemption. All students, regardless of age, are screened for Tuberculosis (TB) by a risk assessment questionnaire, consistent with guidelines from the Center for Disease Control and the American College Health Association. Not all students will require TB testing. Health Profession students must submit immunization information and TB test results. In addition, students under age 26 years at time of registration are required by D.C. Law 3-20 to provide documentation of vaccination or immunity (lab test, if appropriate) from Diphtheria, Tetanus, Hepatitis B, Measles, Mumps, Rubella and Varicella. Students under 18 years must be vaccinated against polio. Required Immunizations Three (3) doses of DPT in childhood and a booster of Tetanus/Diphtheria (TD) within the last 10 years. Two (2) doses of measles/mumps/rubella (MMR) after 12 months of age, at least 1 month apart Hepatitis B (3 doses) Meningitis Vaccine Varicella Dose 1 and 2 or a History of Chicken Pox Three (3) doses of polio vaccine Recommended Immunizations Hepatitis A PPD (TB skin test) Human Papilloma Virus (HPV) Please have the health care provider complete and sign the reverse side of this form and return to: Trinity Washington University Health and Wellness Center 125 Michigan Ave NE Washington, DC 20017 Fax: 202-844-9614 Email: healthcenter@trinitydc.edu 1 Trinity Washington University Health and Wellness Center 125 Michigan Ave NE Washington, DC 20017 Phone: 202-884-9615 Fax: 202-884-9614 2014-2015 Mandatory Immunization Form To be completed by the Trinity Washington University Student Name: Date of Birth: Cell Phone Number: Email Address: Semester and Year of Entry: TO BE COMPLETED BY A HEALTH CARE PROFESSIONAL A copy of an immunization record is acceptable Tetanus/Diphtheria _____/_____/_________ (Booster in the last 10 years) OR Tetanus/Diphtheria/Pertussis ______/________/_______ (Booster in the last 10 years) MMR#1 ___/____/____ (Must be after 12 months of age) MMR#2 ____/_____/____ (Given at least 30 days after Dose 1 Immunizations that do not follow the above schedule must be accompanied by a lab report showing positive immunity. _____ Hepatitis B #1 ___/___/____ Hepatitis B #2 ___/___/___ (Given at least 30 days after Dose 1) Hepatitis B #3 ___/___/___ (Given 4 months after Dose 2) Or Attached lab report showing positive immunity _______ Varicella # 1 ___/___/___ Varicella #2 ___/___/___ (given at least 30 days after the Dose 1) Or Attached lab report showing positive immunity ________ Polio #1 ___/___/___ Polio #2 ___/___/___ Polio #3 ___/___/___ Or Attached lab report showing positive immunity ________ For students living on campus: Meningococcal ___/___/___ Or Attached Meningitis Waiver. Can be found on the Forms section of the Health and Wellness Center website. You will need TB testing (PPD or QFT or T-SPOT) regardless of BCG vaccination, if you meet any of the following conditions: 1. You are a health professions student. 2. You have signs or symptoms of active tuberculosis as determined by your healthcare provider. 3. You have a chronic medical condition such as diabetes, renal failure, HIV infection, leukemia or lymphoma or other serious condition as determined by your healthcare provider. 4. You were born in, lived in or traveled for more than 6 weeks in any country not on this list: USA, Albania, American Samoa, Andorra, Antigua, Barbuda, Australia, Austria, Barbados, Belgium, Bermuda, Virgin Islands (British and US), Canada, Cayman, Chile, Cook Islands, Costa Rica, Cuba, Cyprus, Czech Republic, Denmark, Dominica, Finland, France, Gaza Strip, Germany, Greece, Grenada, Hungary, Iceland, Ireland, Israel, Italy, Jamaica, Jordan, Lebanon, Luxembourg, Malta, Monaco, Montserrat, Netherlands and Antilles, New Zealand, Norway, Oman, Puerto Rico, St. Kitts and Nevis, St. Lucia, Samoa, San Marino, Saudi Arabia, Slovakia, Slovenia, Spain, Sweden, Switzerland, Trinidad and Tobago, UAE, UK, West Bank. 5. You have worked or resided in settings such as nursing homes, homeless shelters, long-term hospital residential facilities, prisons, or have injected drugs in the past. 6. You have had close contact with someone with infectious tuberculosis I do not meet any of the conditions 1 through 6 above and do not require further TB testing. Name: ____________________________ Signature: _________________________________ Date: ____________ 2 CONTINUED ON NEXT PAGE A PPD-Mantoux or QFT or T-SPOT testing must be done within the past 12 months. PPD placed _______ PPD read ________ Result in mm induration ______ Result: Positive ____ Negative____ QFT or T-SPOT: ______/______/______ Result Positive ____ Negative____ Other _____ In case of a positive PPD or QFT or T-SPOT a chest X-ray is also required. Date of X-ray _______ Result ______________ OR Previous history of a positive PPD, QFT, T-SPOT test: Previous test __________ X-ray __________________ A normal chest X-ray within 12 months is required, unless history of INH therapy is documented. Date of INH treatment ______________. Signature of Healthcare Provider Required: Printed Name: _______________________________________________ Phone: ______________________________ Signature: ____________________________ ______________________ Date: _______________________________ FOR STUDENTS UNDER 18 YEARS OF AGE Parental permission or consent of legal guardian is needed to provide medical or surgical care to minors. The following statement should be signed by parents or guardians of students under 18 years of age to avoid delays in treatment in the event of an illness or accident: I hereby authorize the staff of Trinity Washington University Health and Wellness Center to interview, assess, test and if necessary treat my son or daughter as deemed advisable. Signature: ____________________________________ Date: _____________________ __________________________________________________________________________________________________ Healthcare Provider Signature/Title Date Office Stamp An office stamp must be used to validate this form __________________________________________________________________________________________________ For office use only: Staff verification: ___________ Compliant or Non-compliant Date:____________ Noncompliant: TD/TDap MMR Hep B Varicella Meningococcal Polio 3