Application for Participation as an Affiliate Center in the BMT CTN
advertisement

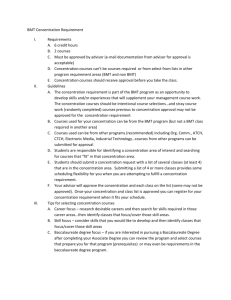
APPLICATION FOR PARTICIPATION AS AN AFFILIATE CENTER IN THE BMT CTN Minimum qualifications are a “Yes” to one of questions # 9, 10, or 11. BMT CTN Protocol #: Protocol Title: Center Name: Center Address:: Date Submitted: Submitted by: Title: Phone: E-mail: PI Name: PI Phone: PI Email: PI Address: CTEP Site Code if known: This protocol is available on the BMT CTN public website at www.bmtctn.net. Please review the protocol thoroughly before completing this application. EMAIL COMPLETED APPLICATIONS TO BMT CTN DCC/EMMES AT bmtctnac@emmes.com 1. What is your projected annual patient accrual for this protocol? 2. Will your center be including pediatric patients? Yes No 3. Please complete the table on the next page to document your transplant center’s activity (note: if you register your transplants with the CIBMTR, you do not need to complete this section but you should check that your registration is up to date). DCC USE ONLY: The center will enroll through: BMT CTN SWOG/CTSU CALGB/CTSU ECOG/CTSU Other_____________ Page 1 of 5 BMT CTN Affiliate Participation Form 12/2015 Twelve Month Period: through Month Auto Year Month HLA-id Sibling Other Relative Year Unrelated BM or PBSC Unrelated Cord Blood AML ALL CML CLL MDS Other Leukemia MPS Follicular NHL Diffuse Large Cell NHL Lymphoblastic NHL Other NHL Hodgkin Disease Multiple Myeloma Neuroblastoma Breast Cancer Other solid tumor Aplastic Anemia Immune Deficiency Inborn Errors of Metabolism Autoimmune Disease Other, specify: 4. If your accrual projections exceed the past 12 month’s transplant activity, please explain. 5. Please list your staff whose job functions are transplant-related research. Title Total FTEs Protocol Nurse Regulatory Coordinator Data Manager Other, specify: Page 2 of 5 BMT CTN Affiliate Participation Form 12/2015 6. Do you have active, IRB-approved protocols at your center that will compete against the current protocol? Yes No If yes, please justify your accrual projections: 7. Please estimate the time frame from approval for participation until first patient enrolled at your center. Consider the time needed for contracting, training and IRB approvals. 8. How many active, IRB-approved transplant research protocols are currently open at your center? 9. Is your center an NMDP participating center? Yes No 10. Is your center FACT accredited? Yes No If no, have you completed an application for FACT accreditation? Yes, . No Date completed 11. Is your center an approved NCI Cooperative Group transplant center? Yes No If yes, which Cooperative Group(s): SWOG Yes No CALGB Yes No ECOG Yes No COG Yes No If yes, please check appropriate box(es) below: Auto Allo Page 3 of 5 BMT CTN Affiliate Participation Form 12/2015 12. Is your center a CIBMTR participating center? Yes No If yes, do you submit data on: Allogeneic Transplants Autologous Transplants Please note: all CIBMTR participating centers must submit a Comprehensive Report Form (CRF) unless otherwise noted for any patient participating in a BMT CTN trial regardless of your center’s status for CIBMTR data. Do you agree to submit Comprehensive Report Form level data to the CIBMTR on all patients enrolled in a BMT CTN trial AND TED level data for all patients transplanted at your center, whether or not they are enrolled in a BMT CTN study, during the period you are actively enrolling patients as an Affiliate Center? Yes No A copy of CIBMTR data collection forms can be found at: http://www.cibmtr.org/DataManagement/DataCollectionForms/index.html 13. Do you have a pharmacy that is able to receive, store and dispense investigational drugs and maintain appropriate documentation? Yes No 14. Does your pharmacy charge a dispensing fee for investigational agents? Yes No If yes, what is the fee for the following? In-patient iv In-patient oral Out-patient iv Out-patient oral _ per dose per dose per prescription per prescription 15. Does your center have the ability to process research specimens and appropriate freezer (-70º C) storage? Yes No 16. Is your Radiotherapist Board-Certified? Yes No Page 4 of 5 BMT CTN Affiliate Participation Form 12/2015 17. Can your radiation department perform fractioned TBI? Yes No 18. Is your radiation facility on-site or off-site? On-site Off-site If off-site, please explain transportation arrangements 19. Has your center previously participated in BMT CTN protocols? Yes No 20. Does your center have high-speed Internet access (> T1 – 1.544 mbps)? Yes No 21. What is your principal Internet access platform? (please mark only one) PC MAC Unix/Linux 22. Do you have Internet Explorer for Internet access? Yes No Page 5 of 5 BMT CTN Affiliate Participation Form 12/2015