Paper for Eco - JScholarship

Easy and Inexpensive Needle Remover
Mary K. O’Grady
Abstract— There is evidence for the need of a more economic needle remover to reduce the volume of sharps waste in third world countries and lead to safer practices with sharps disposal.
I have developed a low cost device that can attach to globally disseminated safety boxes and remove needles from syringes reducing the volume of sharps and encouraging safe disposal practices. My plans for dissemination of this technology include applying for grant money from NCIIA and The Global Fund for the manufacturing and packaging of the device for dissemination through the World Health
Organization (WHO) to hospitals and clinics with safety boxes to adhere the device and instruct healthcare workers how to use it.
I.
INTRODUCTION
E VERY
year 16 billion injections are given, half of which are deemed ‘unsafe’ [1,2]. Each year 2 million of 35 million Healthcare Workers globally experience percutaneous exposure to infectious diseases [3]. Nearly 40% of Hepatitis B and C cases in Healthcare Workers are due to needle stick injuries as well as 4.4% of HIV/AIDS in Health-Care Workers [3]. This accounts for
160,000 cases of HIV, 4.7 million cases of
Hepatits C, and 16 million cases of Hepatitis B
[2].
A.
Validation of Medical Need
The following statements validate the need for a new economic technology to reduce sharps waste in a safe and economic manner.
‘Being stuck during needle recapping after use and during injection are the most common and
Manuscript received May 10, 2010. M. O’Grady is a student in the
Department of Biomedical Engineering at the Johns Hopkins University,
Baltimore, MD 21218 USA. (phone: 410-948-6991; email: mogrady3@jhu.edu). most serious needle-stick injuries as this has the potential for HBV, HCV and HIV infection.’ -
Dentist from North Jordan [4]
‘Safe syringe waste disposal systems, which are the focus of this guide, are needed to eliminate the second and third sources of risk. In primary health facilities, there is an urgent need for better waste disposal systems, especially in countries where resources are scarce and the infrastructure to handle waste does not exist.’
-John Lloyd [5]
‘For optimum safety of healthcare providers and patients alike, a simple, quick, and single handed approach to sharps waste in close proximity to where injections are given is absolutely key. Risk of accidental needle sticks increases greatly the more you have to manipulate and the farther you must carry an infected needle. A simple, economic, and versatile intervention for preventing infections is a holy grail for modern medicine.’Lisa Nagy
RN, BSN [6]
‘ Best practices in health care recommend the segregation of needles/sharps at point of use’-
WHO [7]
B. Inadequacy of Current Devices
There are three sources of risk from unsafe injections:
1. Patient-to-patient transmission of infection due to the reuse of syringes.
2. Patient-to-health worker transmission due to needle-stick.
3. Patient-to-community transmission due to unsatisfactory final disposal. [5]
While Auto-disable (AD) needles have been introduced as a standard to address the first risk by making it impossible to reuse the needle, many
AD needles still have exposed needles that can
prick Health-Care Workers. The AD needles that do account for this and work by retracting the needle and breaking it inside are more expensive and lead to a higher volume of waste, which is expensive to dispose of.
The Uniject made by BD has a reduced volume of waste by design. These needles are prefilled with medication and pressing a small plastic button attached to the needle releases the medication. Although the disposed waste is smaller overall the whole unit must be refrigerated instead of a vial of medication. Since 10 Unijects require more space than a ten-dose vaccine vial hospitals and clinics with limited cold room storage may be less likely to incorporate this design into their health care system [8].
Fig. 1. Uniject, a small autodisable needle made by BD.
(Nelson, Carib)
Other solutions besides retractable syringes, which can lead to pricks if not retracted correctly, include protective covers for the needle (BD’s Eclipse Cover or Safety Glide) and manual retraction with a protective shield.
Neither of these solutions prevents the leakage of contaminated fluids however. In addition weaknesses of these
Fig. 2. BD’s Eclipse
Cover is a syringe with a protective cap. http://www.bd.com/safety/pr oducts/injection/
Fig. 3. BD’s Safety
Glide is a syringe with a protective cover. http://www.bd.com/safety/prod ucts/injection
/ syringes include difficulty of low angle injections due to the cap or slide cover and catching of the cap on clothing of the nurse of patient. Needles that simply render the syringe plunger inoperable protect from reuse, but do not protect from pricks.
While the risk for eliminating reuse of needles has led to single use syringes. The international retail price for a single use syringe and needle set ranges from 3 US cents (sterile hypodermic syringe 2 ml) to 6 US cents (auto-disable syringe
0.5 ml)[9]. Companies have doubled the cost of syringes by making them auto-disable and even then some of these needles still have unprotected contaminated needles that need to be removed.
In order to eliminate the second and third sources of risk safe syringe waste disposal systems are needed. There is a need for better waste disposal systems in primary health facilities, especially in countries where resources are scarce and the infrastructure to handle waste does not exist [5]. Current practices for disposing of safety boxes, which contain needles and syringes include: incinerating, burning and burying.
Burning is not safe, requires supervision, and leads to environmental hazards from the smoke and emissions and burying is even less safe, requires digging, and has an even higher environmental cost. While incinerating safety boxes is the safest method it is also very expensive, but reducing the volume of waste could decrease costs [5].
A current solution to reducing the volume of waste is to use needle removers to separate the needle from the syringe. Not only does this reduce the bulkiness of the system and increase
Fig. 4. A Needle
Remover
(Lloyd, John) the number of syringes that can fit in a safety box, if the needle is separated from the syringe, the box with the syringes does not need to be puncture-proof and is
not a danger to people transporting the waste.
Needles themselves take up very little room when separated from the syringe and hundreds can be put into puncture-proof boxes for safe transport and disposal. Sharps waste is reduced 20-60% overall if the needle is removed [5].
The only problem left then, is that these removers needle are expensive. Ranging from $9-$70/device, and these devices
Fig. 5. BD Safety Clip is need to be located a type of needle remover http://www.glucosemeters
in every room
4u.com/needlewhere a needle removal.htm may be used [5].
Most of these devices also require two hands to be operated and take up precious time of health care workers to operate.
Still in development, but much more promising is the Antivirus. A polypropylene plastic cap that permanently attaches to the top of soda cans and has a built in system that safely dislocates the needle and drops it into the can. Cans can hold
150 to 400 needles depending on their depth, and cost $1.60 to $2 a piece. The cap itself costs only
$0.83. This cap may be exactly what is needed in third world countries since it is cheap and resourceful. Although the cap that snaps onto the can is permanently attached to the can and the cap is designed so that needles cannot come out the top the final stage of waste disposal has not been made clear. I believe that these cans would still need to be incinerated since if a soda can is crushed the needles will most likely poke through.
If this is the case then the can itself and the plastic top are adding to the waste because they will not turn to ash as easily as cardboard and the metal scraps would need to be swept out of the incinerator with the sterile metal needle scraps. I am also not sure that this device works with needles that twist onto syringes. In the demonstration video on their website
(http://www.yellowone.dk) they only showed the removal process for a push-in needle on a syringe.
Finally, the question remains whether hospitals will forgo using the safety boxes they are given to start using these caps on cans and whether the cans will be properly disposed of if used. For hospitals unwilling to switch out their safety boxes for soda cans I am proposing a new solution. are said to be plentiful especially in developing countries where clean water is hard to come by
[7]. Using a can eliminates the need for the "safety boxes" currently used by the World Health
Organization and UNICEF which are essentially cardboard containers, which hold 100 needles and
II.
M
ETHODS
A.
Design
In examining what is necessary for an effective method to reduce sharps waste in third world countries I have come up with the following criteria. The needle remover must be economical, specifically less than $0.83/200 needles. To make it economical the device should be easy to manufacture, light weight, and easy to package and ship. The device should also be easy to use.
There are a limited number of trained healthcare workers in many developing countries. They will not want to take the time to learn to use a complicated device. The device should be able to remove needles using only one hand if possible to allow healthcare workers the freedom of their other hand. The ideal device would be designed to attach to the safety boxes already distributed by
A
B the WHO and could be easily integrated into current distribution systems either on the boxes or with the boxes. For regions that may not receive these boxes from the WHO the device should eb able to integrate with most any puncture proof container. Finally, the device should be aesthetically pleasing so that in has the potential for being adopted by hospitals in regions that may be better-off socio-economically but are still looking for economic solutions.
B.
Prototype
I have developed an easy and inexpensive needle remover that can be stuck onto the top of the commonly used puncture proof boxes for needle disposal directly over the slot. The needle remover can be adhered by using strong glue such as Krazy glue, a sticky tack adhesive or a doublesided tape on the edges. The device also includes holes allowing it to be nailed or screwed onto the top of a puncture proof container.
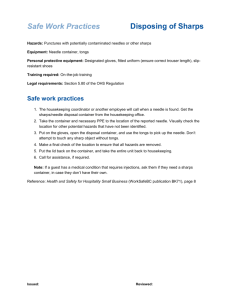
With only one hand the nurse can insert the syringe needle-tip down into the circular hole, slide the syringe toward the narrower end of the slot with the lip of the needle under the plastic rim and pull up on the syringe to remove the syringe from the needle while the needle falls into the box.
For needles that are twisted onto the syringe, small grooves have been added to the edges of the narrow end of the slot, which allow the healthcare worker to wedge the needle in place and twist the syringe off while the needle falls into the box. In both cases the syringe can be disposed of in a separate safety box, which is not dangerous for transport.
Fig. 8.
Method for using needle remover with syringe.
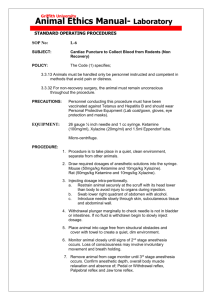
Fig. 7. Needle
Remover A. Top, B.
Side, C. Bottom of device. D. Shows where it would be placed on top of safety box.
C.
Materials
This design consists of only two parts, the plastic piece and the adhesive to attach it to the sharps container. The initial tooling cost for the plastic part if made by Epsilon Industries Inc. would be $3,400 for 4 molds but the cost per piece is only $0.18 [10]. The adhesive if in the form of a mounting tape would be less than $0.015/piece if bought in bulk based on the cost of mounting tape sold at Sears. The cost of this solution would be very low, $0.20 at most with mass manufacturing and depending on the material used.
IV.
D
ISCUSSION
A.
Evaluation of Design
Although I have not been able to get a needle to fall out of the top by turning upside down and shaking a safer model would have a cap over the device or tape over it to ensure that needles do not fall out of the container if an ordinary tin can or cardboard box is being used. The boxes distributed by the WHO already account for this by having a flap that will slide in to close the hole on the inside of the box so the needle remover is not obstructing the flap. See Fig. 10.
III.
R
ESULTS
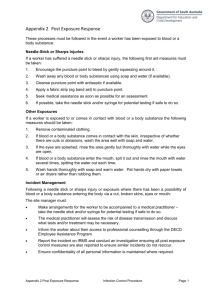
The prototypes of my needle remover were made using rapid prototyping and the needle remover works for both push-in needles and twiston needles. A variety of adhesives such as Krazy glue and sticky tac were also used to adhere the prototypes to puncture proof containers such as thick cardboard boxes and tin cans. The operation currently requires two hands since the boxes and cans are not mounted to anything and are not heavy enough by themselves to not shift when using. The length of 48mm was chosen after looking at the specification of the safety boxes distributed by the WHO in order to cover the opening on the box and leave room for adhesive contact. The final design is shown below in Fig. 9.
Fig. 9. Drawing of Solution with
Measurements in mm.
Fig. 10. Needle remover is adhered to box over original hole. When box is full, flap is pushed in and covers hole from the inside keeping needles from falling out.
B.
Plan for Dissemination
After contacting Gretchen Gall, Project
Coordinator of Engineers Without Borders-USA
(EWB-USA) I was advised to contact health organizations working in developing countries in order to disseminate the device. EWB does not disseminate technology, but rather uses the technology and materials in the country to make devices or solve problems. I also contacted
Adriane Pallat Berman, MPH, Senior Program
Associate for PATH who informed me that while they do not disseminate technologies they may be able to link me with interested manufacturers and stakeholders. She suggested following the WHO’s
Product Quality Standard (PQS) process to have it distributed by the WHO.
That being said there are now at least two ways
that this device could be spread to developing countries. Since the device could be carved from wood and adhered with tree sap or local glue, a program such as EWB could introduce the design and the method of carving it to locals who could then make it for clinics and hospitals to attach to safety boxes.
However, since it may be difficult for locals to make a business making this device the best method would be to distribute the device with the boxes. Not all of the boxes distributed by WHO come from the same company, but they do have to meet the PQS specifications [11]. This makes difficult to convince all of these separate companies to add the device to their box especially since the boxes need to be packed flat to meet specifications [11].
If the device was to be distributed separate from the boxes it should still be through the WHO. By following the WHO guidelines for ‘Needle Cutters for Health Waste Management’ and by working with the people of the WHO, I could ensure that my device is distributed to the clinics and hospitals with safety boxes and adhere the device and instruct healthcare workers how to use it [12].
R
EFERENCES
[1] World Health Organization (2004). Proposed agenda to evaluate the risks and benefits associated with using needle-removing devices.
Switzerland.
[2] Kermode, Michelle. Unsafe Injections in Low-Income Country
Health Settings: Need for Injection Safety Promotion to Prevent the
Spread of Blood-Borne Viruses.
Health Promotion International
(Journal). http://heapro.oxfordjounrals.org/cgi/content/full/19/1/95
[3] World Health Organization. Occupational Health: Needlestick
Injuries. http://www.who.int/occupational_health/topics/needinjuries/en/index.
html
[4] Khader, Y., S. Burgan, and Z. Amarin. "Self-Reported Needle-Stick
Injuries among Dentists in North Jordan." Eastern Mediterranean
Health Journal 15.1 (2009): 185-9. Print.
[5] Lloyd, John. Designing Safe Syringe Disposal Systems for
Immunization Services . Eds. Anne McArthur and Joanne Simpson.
October ed. Children’s Vaccine Program at PATH, 2003. Print.
[6] Nagy, Lisa. Justification for Needle Remover . Ed. Mary O'Grady.
Justification and need for an economic needle remover Vol. , 2010.
Interview. May 10,2010.
[7] Pham, Han. "Antivirus Product Design."Web. Apr. 7, 2010
<http://www.yellowone.dk>.
[8] Nelson, Carib, Dr Anton Widjaya, and Scott Wittet. Using Uniject™ to Increase the Safety and Effectiveness of Hepatitis B Immunization.
September ed. 6 Vol. Seattle, WA: Children’s Vaccine Program at
PATH, 2002. PATH. Web. Mar. 29, 2010.
[9] GUIDING PRINCIPLES TO ENSURE INJECTION DEVICE
SECURITY. Department of Essential Health Technologies World
Health Organization, 2004. SAFE INJECTION GLOBAL
NETWORK (SIGN) SECRETARIAT. Web. Apr. 7, 2010.
[10] Naramor, Matt. Quote for Needle Remover . Ed. Mary O'Grady. quote of manufacturing Vol. Chino, CA: Epsilon Industries Inc., 2010. Print
[11] World Health Organization. Safety Box for the Disposal of used
Sharp, PQS Performance Specification . WHO/PQS/E10/SB01.1 Vol.
World Health Organization, 2007. Print.
[12] World Health Organization. Needle cutter for health waste management, PQS Performance Specification .
WHO/PQS/E10/NC01.1 Vol. World Health Organization, 2008. Print.
V.
C
ONCLUSION
Even with the basic design of the device completed there is still a lot of work to be done before this product is used globally. Modifications can be made to the design to make the use more intuitive for twisting off needles from some syringes. Further research on the various types of needles distributed to these countries should be done to make sure that it would remove the most common needles. In addition, collaboration with
PATH members will be necessary to choose a region to begin dissemination and conduct a trial study to ensure its effectiveness and ease of integration into healthcare systems.
IGURE
R
EFERENCES
[13] Nelson, Carib, Dr Anton Widjaya, and Scott Wittet. Using Uniject™ to Increase the Safety and Effectiveness of Hepatitis B Immunization.
September ed. 6 Vol. Seattle, WA: Children’s Vaccine Program at
PATH, 2002. PATH. Web. Mar. 29, 2010.
[14] "BD, Healthcare Worker Safety, Products." 2010.Web. Becton,
Dickinson and Company. Apr. 5, 2010
< http://www.bd.com/safety/products/injection/ >.
[15] "BD, Healthcare Worker Safety, Products." 2010.Web. Becton,
Dickinson and Company. Apr. 5, 2010
< http://www.bd.com/safety/products/injection/ >.
[16] Lloyd, John. Designing Safe Syringe Disposal Systems for
Immunization Services . Eds. Anne McArthur and Joanne Simpson.
October ed. Children’s Vaccine Program at PATH, 2003. Print.
[17] "BD Safe Clip Needle Removal Device." BD.
2010.Web.
< http://www.glucosemeters4u.com/needle-removal.htm
>.
[18] Pham, Han. "Antivirus Product Design."Web. Apr. 7, 2010
< http://www.yellowone.dk
>.
F
A
CKNOWLEDGMENT
M. O’Grady would like to thank Heather Benz for her help in the formatting of this paper.