microbiology ch 42 [9-4
advertisement

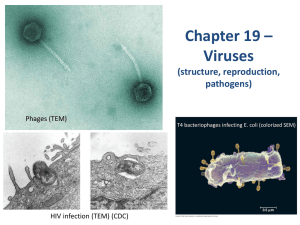
Micro Chapter 42 Key Concepts Pathogens: beta and gamma herpes viruses – large enveloped ds DNA viruses distinguished by genomic organization and pathogenesis in humans o Beta herpes viruses include CMV, HHV-6, and HHV-7 o Gamma herpes viruses include EBV and rhadinovirus HHV-8 (Kaposi sarcoma herpes virus) Encounter: most individuals acquire infection by young adulthood; ubiquitous in human populations Entry: virus attaches to cells by low-affinity interactions w/cell-surface GAGs, followed by high-affinity interactions between viral envelop glycoprotein and receptor on cell surface to induce uptake Replication: viral gene expression mediated by virus-encoded enzymes; viruses assemble in nucleus and acquire tegument and envelope layers by sequential passage through nuclear and plasma membranes o Release occurs by exocytosis or cell lysis o After primary infection, virus establishes life-long latency (CMV in myeloid cells; EBV in B cells) w/intermittent virus shedding from mucosal surfaces Spread: occurs from primary site of inoculation to multiple organs via bloodstream Damage: CMV rarely associated w/clinical symptoms in normal individuals but can be opportunistic pathogen in immunocompromised hosts, including developing fetus o Primary infection w/EBV usually asymptomatic in young children but can be associated w/mononucleosis syndrome during adolescence In immunocompromised persons, can cause lymphoproliferative syndromes (PTLD, which may progress to malignant lymphoma) Associated w/cancers, such as lymphoma, nasopharyngeal carcinoma, and other epithelialderived neoplasms Diagnosis: CMV detected in biopsy tissue or blood samples by isolating replicating virus or detecting either viral nucleic acids w/PCR or viral antigens w/immunoassays o EBV mononucleosis diagnosed using heterophile antibody tests (monospot) or specific EBV serologies Diagnosis usually made by detecting viral nucleic acids Treatment: antiviral treatment of mono doesn’t alter course of illness o Opportunistic infections w/CMV can be treated w/antiviral agents (ganciclovir), reduction of immunosuppression, or both Prevention: no vaccines for either; affected patients not isolated because of ubiquity of infection Cytomegalovirus and Epstein-Barr Virus Infection occurs following exposure of mucosal surfaces to infectious virus; both viruses can be isolated from secretions collected from oropharynx and genital tract Early in life, CMV readily transmitted in breast milk; virus acquisition during adolescence more common and results from intimate exposure to oropharyngeal secretions or sexual contact o CMV readily crosses placenta and infects developing fetus, giving rise to congenital CMV infection o Congenital CMV can lead to severe disease and permanent neurological damage, including hearing loss Breastfeeding not important route of EBV transmission o In populations w/limited exposure to EBV during childhood, infection in adolescence and young adulthood can result in symptom complex and lab features that define acute infectious mononucleosis Primary infection w/either CMV or EBV rarely results in symptomatic disease in infants and children o Small proportion of mono associated w/primary CMV infection Infection w/either virus can follow blood transfusion or transplantation of allograft from infected donor o Infection following blood transfusion can result in symptomatic disease Both viruses utilize 2 modes of entry – different viral envelope glycoproteins required for each form of entry; acid-dependent or acid-independent mechanisms predominate, depending on target cell o Interaction w/receptor/coreceptor and fusion at PM o Interaction w/receptor/coreceptor at PM followed by internalization, acid-dependent fusion, and release of nucleocapsid and tegument proteins from endocytic vesicles CMV fusion requires gB, gH, and gL, and in epithelial cells additional component consisting of glycoproteins encoded by UL128 to 131 open reading frames o Loss of glycoproteins limits epithelial cell entry by CMV but not entry into other cell types (fibroblasts) EBV infection of B cells initiated by attachment of envelope glycoprotein gp350/220 to CD21 (CR2) o After endocytosis, viral glycoproteins gB, gH, and gL and lymphocryptovirus-specific glycoprotein gp42 participate in fusion of viral envelope and endocytic membrane o Entry of EBV into epithelial cells occurs at neutral pH and doesn’t require endocytosis; fusion requires only gB, gH, and gL; virions lacking gp42 infect epithelial cells more efficiently than those with gp42 CMV and EBV replicate nucleic acids in nucleus of infected cells o Orderly expression of viral genes during lytic virus infection characterized by sequential expression of immediate-early, early, and late viral genes required for production of progeny virus o Nucleocapsids containing infectious DNA translocated to nucleus by microtubular transport o Transcriptional program initiated by interactions between proteins contained in virion tegument and cellular factors that activate expression of viral immediate-early genes; virion tegument proteins also disarm certain host cell-intrinsic antiviral responses o Expression of viral immediate-early genes leads to sequential expression of viral genes required for viral nucleic acid synthesis (viral DNA-dependent DNA polymerase) and viral genes that encode virion structural proteins Also encode proteins that limit apoptosis and innate immune response to viral infection; insure host cell survival long enough for production of progeny virus o Assembly of virions includes nucleocapsid formation, viral DNA packaging, and envelopment conserved in all herpes viruses; assembly involves both nuclear and cytoplasmic steps In nucleus, nucleocapsid shell constructed around scaffold generated by virion capsid protein, resulting in formation of icosahedral nucleocapsid that provides site for viral DNA packaging o Viral DNA synthesized as long chains of genome-length DNA copies (concatemers) and cleaved into unitlength genomes during packaging and capsid maturation Newly replicated viral DNA encapsidated in nucleus o Nucleocapsids exit nucleus by sequential budding through inner and outer leaflets of nuclear membrane, acquire tegument layer of protein in cytoplasm, and eventually become enveloped in secretory pathway o Progeny virions egress from infected cells w/lipid-containing envelope of viral glycoproteins o Virus of infectious virus occurs either through process of regulated exocytosis or following death of infected cell o Envelope glycoproteins elicit protective antiviral antibodies that neutralize infectious virions Persistent and Latent Infections Latent viral infections characterized by restricted viral gene expression and lack of progeny virus production o CMV can persist as latent infection in CD34+ myeloid progenitor cells and, following migration to organs such as liver, undifferentiated but lineage-committed cells undergo terminal differentiation leading to reactivation of latent infection o Latency-associated transcripts expressed during latency Latent infection by EBV associated w/persistence of viral genome in absence of lytic infection and expression of specific viral genes o In initial phases, viral genes (Epstein-Barr nuclear antigen-1) expressed to insure maintenance and partitioning of viral genome as replicating episome during expansion of infected cells o Expression of latent membrane proteins (LMP1 and LMP2a) provides growth signals to infected cells that drive cellular proliferation o Minimal number of viral genes and small RNAs expressed in long-lived nondividing B cells (reservoir) o Reactivation from latency occurs sporadically; B lymphocytes undergoing reactivation can release infectious virus that can infect epithelial cells, leading to periodic shedding of EBV during lifetime of host Reactivation most readily observed in patients w/defects in virus-specific T-lymphocyte responses and those undergoing cytotoxic or immunosuppressive therapy o miRNAs that function in posttranscriptional gene regulation serve as major regulatory mechanism in development, homeostasis, and stress responses, including viral infections miRNAs have critical roles in virus replication (interference w/cellular antiviral responses and establishment and maintenance of latent infection) miRNAs inhibit expression of immediate-early genes in CMV-infected cells miRNAs inhibit EBV DNA polymerase during lytic infection Induce host cell miRNAs, some of which downregulate cellular antiviral responses Cellular miRNAs upregulated in B-cell malignancies induced by EBV Viruses disseminate within infected host as cell-associated virus o CMV infects wide variety of cells (epithelial and endothelial cells, blood mononuclear cells, neural progenitor cells, and supporting cells of CNS) o EBV infects B lymphocytes and epithelial cells Host Responses Cellular effectors including NK cells and virus-specific cytotoxic CD8+ T cells limit replication of CMV and EBV during primary infection and provides surveillance during viral latency to limit reactivation o Loss of responses leads to reactivation, virus dissemination, end-organ infection, and disease o Biologics used to block inflammatory responses (anti-TNF antibodies for treatment of rheumatologic diseases) associated w/severe CMV and EBV infections CMV proteins encoded by genes downregulate and degrade MHC class I and MHC class II proteins and modulate NK cell receptors and function o Several virus-encoded activities present intrinsic cellular responses to infection (DNA degradation, interferon induction, and apoptosis) o Encodes number of functional cytokines (IL-8 and IL-10) and chemokine receptors that modulate inflammatory response to favor virus persistence in host EBV protects itself by expression antiapoptotic functions, induction of immunomodulatory pathways, and inhibition of antigen presentation by MHC molecules Clinical Syndromes Acute mononucleosis syndrome – low-grade fever, fatigue, pharyngitis, cervical lymphadenopathy, splenomegaly, and peripheral blood monocytosis w/atypical or reactive lymphocytes o Heterophile-negative mononucleosis points to CMV not EBV Clinical symptoms associated w/CMV and EBV self-limited, little value in antiviral therapy (host immune system already reacting when symptoms show) Atypical lymphocytes seen in infectious mono are activated CD8+ T lymphocytes directed against viral antigens on infected cells; critical to control of viral infection; host response responsible for many clinical manifestations Infants w/congenital CMV exhibit significant multiorgan disease secondary to unrestricted virus replication and direct viral cytotoxic effect on target organs o Can have CNS involvement, hepatitis, and hematologic abnormalities o CNS disease includes encephalomalacia, hydrocephalus, retinitis, and damage to auditory system leading to hearing loss o Liver and bone marrow involvement self-limited, but structural damage to CNS can result in long-term sequelae o Sensorineural hearing loss most common sequelae of infection; most common cause of nonfamilial hearing loss in U.S. and Northern Europe; development of hearing loss can be delayed until 3-4 years old o Strong association w/CMV infection and development of coronary artery disease CMV and EBV Infections in Immunocompromised Hosts Infection w/CMV or EBV in immunocompromised individual can result in organ dysfunction and death Acute CMV infections in transplant recipients present as mono-like syndrome (fever, hematologic abnormalities, lymphadenopathy, and hepatitis); in many cases, self-limited o CMV infections in more severely immunocompromised allograft recipients can progress to organ and life-threatening disease including hepatitis, colitis, and pneumonia o Level of morbidity and mortality depends on level of immunosuppression (CD8+ T response) o In transplant patients, chronic productive infection associated w/increased risk of chronic graft dysfunction secondary to exaggerated wound healing responses o Infection in renal allograft recipients leads to tubular dysfunction secondary to fibrosis and scarring o Hematopoietic allograft recipients – disease early or late after transplantation; late disease associated w/more severe graft-versus-host disease and increased morbidity/mortality EBV infection in transplant recipients can occur as consequence of primary acquisition from donor organ or blood products in previously uninfected individual or as result of reactivation of existing latent infection o Following reactivation, lytic EBV can induce lymphoproliferation, leading to syndrome posttransplant lymphoproliferative disease (PTLD) o In most benign form, virus produces acute mono-like syndrome w/lymphoid proliferation o Untreated, evolves into oligoclonal neoplasm that can develop into lymphoma Viral Oncogenesis EBV associated w/Hodgkin lymphoma, Burkitt lymphoma, nasopharyngeal carcinoma, and gastric carcinoma o Cytotoxic T cells directed at EBV LMPs induce clinical remission in some patients w/EBV-positive Hodgkin disease o Chronic malaria can lead to immunosuppression in EBV-infected children, which leads to chronic B-cell stimulation w/increased opportunity for chromosomal translocations that result in aberrant joining of genes encoding immunoglobulin heavy chain and c-Myc oncogene Translocation results in constitutive expression of c-Myc and resultant unregulated cellular proliferation and inhibition of apoptosis o EBV LMPs drive cellular proliferation while limiting apoptosis (oncogenetic) CMV detected in colon carcinoma, prostate carcinoma, cervical carcinoma, and glioblastoma; never etiologically linked to human malignancy Diagnosis, Treatment, and Prevention Diagnosed by isolation of virus in tissue culture, detection of viral antigens or viral nucleic acids in clinical specimens, and assessment of serological responses Isolation of CMV from urine, saliva, blood, and tissue specimens can be done o PCR-based assays (qualitative and quantitative) are standard approaches for identification of CMV in clinical specimens o Hisopathologic detection of large inclusions (owl eye inclusions) in tissue specimens definitive pathological evidence of CMV infection o Antigenemia assay useful for diagnosing in immunocompromised patients; uses immunofluorescence to detect abundant CMV antigen in circulating mononuclear and PMN WBCs; detection of antigens in peripheral blood leukocytes indicates actively replicating CMV Results used to initiate and monitor antiviral therapy in immunocompromised EBV – PCR highly sensitive and specific test for detection o Detection of noncoding nuclear RNAs expressed during EBV infection (EBERs) by in situ hybridization has reasonable sensitivity Acquisition of serologic reactivity (seroconversion) standard approach for detection of primary infection of both CMV and EBV o Detection of IgM antibodies for either CMV or EBV suggests recently acquired infection in immunocompetent hosts o Detection of IgG antibodies specific for either CMV or EBV in single serum specimen provides no info about duration of infection EBV has peculiar pattern of antibody reactivity for structural and nonstructural virus-encoded proteins that allows determination of acute versus longstanding infection by simple serology Serology of little value in diagnosing CMV or EBV in immunocompromised o Relatively high incidence of preexisting infection o Underlying immune dysfunction can lead to inconsistent serologic responses In acute mono, EBV infection induces production of non-EBV-specific antibodies; anomalous antibodies (heterophile antibodies) include some that recognize antigens found in RBCs of heterologous species (i.e., cows) o Serologic reactivity forms basis of heterophile antibody (monospot) test Because viral polymerase enzymes structurally and biochemically distinct from host cell polymerases, they are targets for antiviral drug development for immunosuppressed patients o Ganciclovir and foscarnet inhibit CMV replication; both routinely used in prevention and treatment Ganciclovir – nucleoside analog phosphorylated by virus-encoded phosphotransferase UL97; phosphorylated form of drug blocks virus replication by inhibiting viral DNA-dependent DNA polymerase and arresting elongation of newly synthesized viral DNA Foscarnet – inhibits viral DNA polymerase o Resistance to ganciclovir and foscarnet can quickly develop Ganciclovir and related nucleoside analog acyclovir have activity aginst EBV; treatment can limit virus replication, but treatment of PTLD in EBV-infected transplant recipients w/these has minimal efficacy because viral genes responsible for lymphoproliferation expressed in absence of viral DNA replication o Passive infusion of EBV-specific antibodies or ex vivo-expanded EBV-specific T lymphocytes o Epithelial malignancies associated w/EBV don’t respond to treatment w/currently available antiviral agents because viral replication not prerequisite for oncogenesis Prophylactic and preemptive antiviral therapy of CMV and EBV used to limit disease manifestations; neither approach prevents infection o Prophylaxis w/antivirals used in transplant centers o Preemptive therapy relies on monitoring virologic status of patient; therapy initiated when lab evidence of increasing viral loads Prophylaxis more commonly associated w/late disease in hematopoietic allograft recipients because viral replication inhibited during period when allograft generating adaptive immune responses to CMV, which lowers magnitude of antiviral immune response o When prophylaxis discontinued, virus begins to replicate in absence of T lymphocyte responses, and disease can ensue Passive transfer of antiviral antibodies in IV immunoglobulin modifies disease in CMV-infected kidney and liver transplant recipients; very expensive, but routine in some centers Transfer of ex vivo-expanded virus-specific T lymphocytes protects hematopoietic allograft recipients from severe CMV infections Transfer of EBV-specific T lymphocytes diminishes disease associated w/EBV infection in hematopoietic and solid organ allograft recipients