Multiple substance COSHH form
advertisement

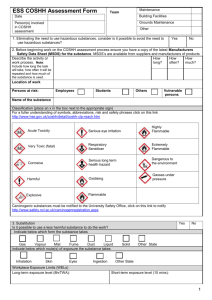
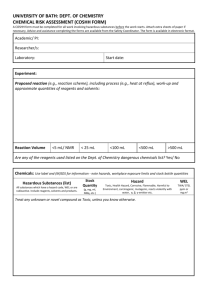
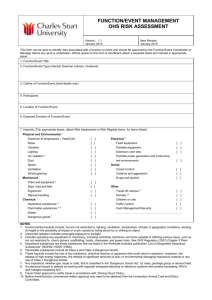
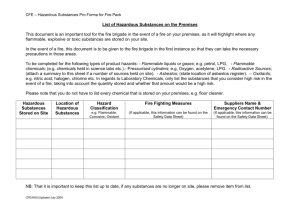
COSHH RISK ASSESSMENT FORM For multiple substances Activity and hazard properties College: School/Department: Location of activity: Description of activity: Substance name CAS Number Quantity (grams/litres) Hazards associated Workplace exposure limit Please attach MSDS for each substance to the hard copy of this sheet Can any of these products be substituted with less hazardous ones? Yes No If yes give reason for not doing so: Are any of the substances being decanted from a larger container? If yes what size is the other container? How are the substances used? (e.g. diluted, applied, dissolved) Persons at Staff Students risk How often Multiple Daily are the times daily substances used? How long are people exposed to the substances when used?(mins) When are In contact In contact the with eyes with skin substances hazardous? Yes No Visitors Contractors Public Weekly Monthly Rarely Inhaled Ingested Injected What is the level of risk is posed by exposure Low Medium High Control measures General precautions Engineering controls Training/briefing requirements Do the control measure reduce the risk to an acceptable level? Are there any further control measures required? Required PPE Other: Other: Type: Type: Type: Area exposed Skin Type: Type: Type: Type: Type: First aid procedure Risk to health First aid procedure Eyes Inhalation Ingestion Waste and spillage procedures Storage requirements Spillage procedure Ecological controls Disposal procedure Fire controls Water Powder Foam CO2 Additional comments Assessor: Date completed: Manager’s signature: Date: Review date: Wet Chemical