NHS Hospital and Community
Health Service in England
workforce statistics – proposed
developments
A consultation on proposed development of the
classification, coverage and output of NHS
workforce publications in England
28 May 2015
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
We are the trusted
national provider of
high-quality information,
data and IT systems for
health and social care.
www.hscic.gov.uk
enquiries@hscic.gov.uk
@hscic
Author:
Bernard Horan
Workforce Analysis Team
Health and Social Care Information Centre
Date of Consultation:
28 May 2015
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
2
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Contents
1)
Introduction
5
2)
Strategic context
5
3)
Purpose
5
4)
Who this document is aimed at
5
5)
When and how to respond
6
6)
Rationale for the review
6
7)
Background
7
8)
General notes
7
9)
Annual workforce census as opposed to monthly staff in post
publications
8
10)
The Proposals
8
11)
Jobs or people?
8
Table 1
9
12)
Bank staff
10
13)
Locums
11
14)
Very Senior Managers and Z Occupation Codes
12
15)
Type of contract
13
16)
Nurse Learners
14
17)
Occupation Code to grade mismatch
15
18)
Staff groups
16
Figure 1
16
19)
Area of Work and Job Role
17
20)
Grades for non-medical staff
19
21)
Updating the Medical Grades
20
22)
Ethnic codes
21
Figure 2
22
23)
Table Structure
23
24)
Tables Provided
25
25)
Bulletin Contents
26
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
3
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
26)
GPs in the Hospital & Community Health Service figures
27
Primary Care staff in the secondary care figures
27
Hospital Practitioners and Clinical Assistants and GPs
28
GPs working in secondary care
29
27)
Should we drop the Role Count?
30
28) Workforce Minimum Data Set (extended ESR Data Warehouse
download)
30
29)
Workforce Minimum Data Set (data from other providers)
31
30)
Organisations which should be included in our statistics
32
31)
Discontinuation of the Health Visitor Minimum Data Set tables
33
32)
England and Wales cross border counting
33
33)
Earnings publications to be published quarterly
34
34)
Have we missed anything?
34
35)
Summary
35
36)
Next steps
35
37)
How to respond
35
38)
Publication of the consultation outcome
36
39)
Responses: Confidentiality and disclaimer
36
Appendix A: Methodology for grade and staff group mismatch
37
Appendix F – NHS Networks details
38
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
4
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
1) Introduction
The Health and Social Care Information Centre (HSCIC) publishes an annual set of reports
on the number of NHS Hospital and Community Health Service (HCHS) and Primary Care
employees in England. The set of annual reports for the HCHS workforce will be referred to
in this document as ‘the annual workforce census’. In addition, we publish monthly staff in
post figures with quarterly supplements for HCHS staff, as well as monthly earnings and
sickness absence figures for HCHS staff.
These are the standard publications for NHS and Primary Care staff in England. The most
recent publications can be accessed via
http://www.hscic.gov.uk/searchcatalogue?productid=17709&topics=1%2fWorkforce%2fStaff
+numbers&sort=Relevance&size=10&page=1#top
In this document the HSCIC is consulting users on possible changes to the way staffing
information for NHS Hospital and Community Health Service (HCHS) in England is defined
and presented in NHS workforce statistics. This consultation is intended to give users of this
information an opportunity to influence the direction of these developments.
2) Strategic context
The HSCIC aims to drive the use of information to improve decision making and deliver
better care, by delivering reliable and timely workforce information to support planning
(workforce, financial and service), performance management, policy development and public
accountability.
The aim of these developments is to provide statistics which produce a clearer picture of
staff providing NHS care and enable an improved range of related analysis.
3) Purpose
The purpose of this document is to consult on what users would like as the most useful set of
statistics produced on hospital and community health care staff in England.
4) Who this document is aimed at
Stakeholders who may use the statistics produced (including members of the public) – to
make them aware of issues and give them the opportunity to participate in the development
and enhancement of appropriate statistics; and
Experts in the NHS and wider health care workforce to ensure that the most effective
scrutiny is applied to all proposals.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
5
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
5) When and how to respond
This consultation will last 11 weeks following its release and will finish on 13 August 2015.
Details on to how to respond to the consultation appear on page 35. However we encourage
anybody who wishes to express an opinion to talk to us and, if beneficial, other stakeholders
if that will help with the development of a response.
We have established a discussion forum on NHS Networks so that people wishing to
respond can discuss and air opinions and issues prior to responding. Details of how to
access this facility are given in Appendix F. This is in addition to any direct discussion with
the HSCIC’s Workforce team that you may like to have.
On completion of the consultation period, views, opinions, and evidence will be considered
and inform the decision as to how this work progresses. The outcome will be posted on the
Workforce area of the HSCIC website in the autumn of 2015 in a document directly
responding to the feedback received during the consultation.
6) Rationale for the review
The NHS is a major employer of people in England. The statistics produced by the HSCIC
are used to answer Parliamentary Questions, queries from the media, pay review bodies and
from many national organisations interested in workforce numbers.
HCHS statistics are currently largely produced using data from the NHS Electronic Staff
Record (ESR) Data Warehouse. The two NHS Trusts not on ESR currently provide a limited
set of data once a year.
The Electronic Staff Record (ESR) is the pay system used by most organisations in the NHS
in England and Wales. The ESR Data Warehouse is a limited set of data downloaded on a
monthly basis from ESR and stored for reporting and analytical purposes. Sometimes they
are both referred to as ESR, but ESR is a live system, the ESR Data Warehouse is a series
of snapshots of the data from the live system.
The monthly workforce publications the HSCIC produces have already responded to
customer feedback, evolving to deliver frequently requested information.
Our annual workforce census publications have changed more slowly, due to both the 12
month gap between publications and the need for consistent output for year on year
comparisons. However, recent developments in processing and publishing monthly NHS
HCHS earnings figures for England have offered new perspectives on the data which impact
on the staff in post publications. These issues necessitate user input and we would like to
take the opportunity to consult as broadly as possible on the NHS workforce output to ensure
that it is a product which meets user needs as closely and conveniently as possible.
In addition, paragraph 5.6 of the General Conditions of the 2014/15 NHS Standard Contract
says:
‘Alongside the Service Conditions of the NHS Standard Contract, SC28 Information
Requirements states a provider must ‘comply with all relevant published NHS
information and data standards, including mandatory returns assessed and published
by HSCIC’.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
6
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
(http://www.england.nhs.uk/nhs-standard-contract/)
To allow Health Education England to understand and plan the workforce delivering NHS
funded care the HSCIC is, at the direction of the Department of Health, supported by Health
Education England and NHS England, extending the collection of health care workforce data
to all providers of NHS Services, including social enterprises, public interest companies,
hospices and the independent health care sector amongst other providers.
This will create a new set of health care workforce data for publication and this consultation
provides an opportunity to advise stakeholders of this development. Further information is
available at:
http://www.hscic.gov.uk/wmds
7) Background
The current NHS workforce census publications do not make full use of the additional
information available within the ESR Data Warehouse.
To a large extent the monthly NHS staff in post workforce publication has taken on this role,
adapting in line with customer requests for data and exploring the potential of the ESR Data
Warehouse in quarterly ‘specials’.
http://www.hscic.gov.uk/searchcatalogue?productid=17709&topics=1%2fWorkforce%2fStaff
+numbers&sort=Relevance&size=10&page=1#top
It may be that users are well served by this arrangement but there are some issues that
need user input which will be discussed, particularly relating to possible changes to
classification of staff.
In addition the HSCIC has responded to the need of workforce planners in Health Education
England (HEE) by liaising with providers of NHS services in all areas of the health care
industry in order to plan a minimum workforce data set which will produce new statistics on
the wider health care workforce in England.
8) General notes
If any reader requires clarification on any technical terms or language used within this
document please get in touch and we will happily provide further clarification.
Many of the subjects below are interlinked.
Where NHS is used in this document refers to the NHS in England.
Wales, Scotland and Northern Ireland produce separate statistics of their own which are not
included within this consultation.
Full Time Equivalent (FTE) is a measure of how ‘full time’ a job is. A job with 1 FTE indicates
that the job is full time. 0.5 FTE indicates half time. A job where the contracted hours are 40
hours a week and the person working in the job works 20 hours a week would result in that
person’s role being classed as 0.5 FTE. Someone working 18 hours in a job where 36 hours
is full time would also be classed as 0.5 FTE in that role.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
7
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
9) Annual workforce census as opposed to
monthly staff in post publications
Recommendations we act on following this consultation will apply to any other relevant
workforce publication we produce.
We currently publish monthly NHS workforce statistics, with expanded quarterly versions.
These figures are referred to as ‘Provisional’ but are now of the same quality as the annual
workforce census figures. Since March 2012, the same September NHS HCHS figures
published in the annual workforce census each March will already have been published in
the previous December’s monthly staff in post publication.
10) The Proposals
The following sections detail the elements of our publications that we specifically want to
draw to the attention of users and would like users to comment on. They are not the only
elements open for comment, we encourage users to take this opportunity to suggest or
discuss any changes they would find useful.
11) Jobs or people?
Our existing staff in post publications for the NHS in England use a field called ‘Contracted
Full Time Equivalent’. If this is greater than zero, it indicates that there is a job being done by
somebody with a set of contracted hours in which case we count them in our staff in post
statistics.
Issues identified
When we developed our NHS Earnings statistics using data from the same source, the ESR
Data Warehouse, we found that if we matched the people who earned money in a month to
the people who we counted in our staff in post figures in the same month, there were more
people apparently working than earning.
The mismatch relates to around 40,000 headcount, or 44,000 roles or 35,000 FTE, over 3%
of all staff currently counted. Further investigation indicated where the mismatch was
occurring as follows:
Around 25,000 unpaid women were still being counted but were on maternity leave.
Discussions with some trusts revealed that they liked to keep the ESR record open for
these women. How trusts maintain their records, which we use for a secondary
purpose, is their choice but the result is that if people have been employed to cover
maternity leave and are being paid through ESR, then such posts are double counted.
Looking back at yearly snapshots of the data there were women who appeared to
have been on maternity leave for up to 5 years. (It may have been that some women
had annual births). A data quality exercise, that asked all trusts whether those absent
for 2 or more years should still be on ESR with contracted hours, did not resolve this
issue.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
8
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Other staff were on career breaks, some were suspended, while some have no
explanation in the data for the mismatch (over 11,000 staff).
We have already included a footnote covering the situation in our published statistics and
there have been suggestions that our figures have always been indications of the contracted
provision at a trust rather than numbers of actual workers.
An indication of the extent of this issue is shown in Table 1:
Table 1
Estimated numbers of records counted in Staff in Post statistics not present in Earnings data
Assignment Status
Head count
Job Count
FTE
Acting Up
21
63
19
Active Assignment
11,264
13,663
11,061
Assignment Costing Deletion
2
15
1
Career Break
2,543
2,679
2,090
Inactive Not Worked
53
128
42
Internal Secondment
13
65
13
Maternity
25,106
25,568
21,262
Out on External Secondment - Paid
11
21
16
Out on External Secondment - Unpaid
494
698
463
Suspend Assignment
18
38
13
Suspend No Pay
504
1,161
425
Suspend With Pay
1
1
1
Widow/Widower
3
4
3
Total
40,033
44,104
35,409
The table shows there are more roles not getting paid but being counted than there are
people. This indicates that some people not being paid have more than one role, but
investigation has shown that there are instances where people are getting paid for working in
one role but have another role where they are not getting paid, sometimes in another
organisation. Occasionally the person has 1 FTE for a paid job and 1 FTE for a dormant role.
Our proposal
There are situations which require such ‘unpaid’ records to be excluded from staff in post
statistics; for example, when supporting investigations where it is necessary to establish
whether there were sufficient staff in place. For this we need to include only those staff who
had been paid in order to provide the numbers of staff actually working that month.
Overall, we feel counting roles where there are indications that there is no one being paid to
perform such roles does not provide an accurate indication of the level of service provided by
NHS staff.
We propose that NHS HCHS workforce numbers should be rebased with 2009 as a starting
year and only staff getting paid should be counted.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
9
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Possible impact
Changing the system to count only paid staff would have an impact on the comparability of
current and past statistics. A limited time series of figures would be reconstructed for
comparability but only for statistics from 2009 onwards.
Additionally, such distinctions could only be made where the data used was from ESR where
the richness of the data allows earnings to be explored. Data from the two non-ESR
providers of NHS workforce data would be accepted without such checking and any other
workforce figures from other providers would not be checked against earnings.
Feedback sought
This is not a clear cut issue and we would appreciate suggestions on how we should deal
with it in all future workforce statistics.
In particular, we would like to hear your views on whether these data findings should be
reflected in the statistics we publish and if you find our proposals to do this are acceptable.
12) Bank staff
Historically, counts of bank nursing and support staff figures were collected once a year and
published in the annual workforce census. These figures were labour intensive to collect and
produce and of poor quality. Their collection and publication was discontinued after 2010.
Issues identified
Whilst researching improvements in the NHS earnings statistics we produce, it was
suggested that the staff records in ESR which did not have contracted hours, but did have
earnings, could be classed as bank staff.
This was consulted on and the quarterly earnings statistics we produce now include total
bank earnings figures.
(http://www.hscic.gov.uk/searchcatalogue?productid=15497&topics=1%2fWorkforce%2fStaff
+earnings&sort=Relevance&size=10&page=1#top)
Our proposal
We propose that we produce a time series of monthly bank ‘staff in post’ figures, potentially
published quarterly, to show seasonal fluctuation. These would be for all staff groups, not
just nurses.
We believe that these additional statistics will enhance the information on service provision
within the English NHS and allow a wide range of supplementary analyses to be carried out.
Possible impact
These figures would only be from NHS organisations using ESR, they would only show bank
staff being paid through ESR, and they would not show agency staff.
Feedback sought
We have included a set of sample tables in Appendix B and would appreciate feedback on
the general idea and the tables we have suggested. In particular, intelligence from people
who work as bank staff or who employ bank staff at trusts will allow us to judge whether the
data available is just a partial picture of the true situation.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
10
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
13) Locums
When we created the monthly staff in post publications to take advantage of the potential of
ESR, we included locum hospital doctors (following a consultation). This data is published
monthly back to September 2009.
Locum data continues to be excluded from the annual workforce census.
We have spoken to trusts about locums and become aware of separate work questioning
how locums should be defined.
Issues identified
There are fields within ESR which we use to identify locum doctors. However work has
shown that many staff we currently class as locums have patterns of employment that can
last years and appear more like fixed term staff or even permanent staff (the categories
counted in our main statistics).
The locum figures we currently publish include data from staff who have contracted hours in
ESR. This suggests that they are not staff called in at short notice for short periods of work –
this model perhaps being how people commonly perceive GP locums to be employed.
We have provided a paper produced for the Workforce Information Review Group (WIRG)
discussing this issue in Appendix G.
Our proposal
We propose that if any doctors currently classed as locums have contracted hours we
reclassify them in the main hospital doctor workforce in all staff in post statistics.
We also suggest that, in a similar way to how we propose to classify bank non-medical staff,
we now class doctors who are paid for work but have no contracted hours in ESR as locums.
These figures would be published in our quarterly bank tables. (Appendix B shows possible
Bank tables.)
Possible impact
The inclusion of existing doctors classed as locums within the main body of doctors would
change the classification of doctors but not have a major impact on the overall numbers
published in our monthly publications as these contain ‘all doctors’ figures which include
locums. However it would affect the doctor numbers published within the annual workforce
census as these have never included any locum numbers.
The other area of impact to our monthly publications would be on turnover statistics. Locum
doctors and doctors in training are not included in the turnover figures. If some of the doctors
currently defined as locums were reclassified into the main body of (non-trainee) doctors,
they would then appear in turnover statistics necessitating the recalculation of existing
figures.
Note: only figures derived from ESR provide details of the new ‘no contracted hours’ locums,
and, as with non-medical bank staff, we have no data on agency staff or locums not paid
through ESR.
Feedback sought
Would this change provide useful information?
Will the suggested changes to locum classification cause users major issues?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
11
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Are there genuine locums with contracted hours on ESR?
If so will their reclassification to the main hospital doctor workforce in all staff in post statistics
create problems?
Is the information that can be derived on locums from the ESR Data Warehouse a significant
representation of the locum workforce or are other sources of locums the major providers? If
there are other sources, please specify what these are.
14) Very Senior Managers and Z Occupation
Codes
Within the Occupation Code manual there are classifications for managers.
In the Administrative Manager grouping these are: Manager (Occupation Codes starting with
G1) and Senior Managers (Occupation Codes starting with G0).
These managers can work across various areas and are included in the tables where
Manager and Senior Manager figures are provided. (Definitions of who should be included in
these coding are provided in the Occupation Code Manual –
http://www.hscic.gov.uk/article/2268/NHS-Occupation-Codes )
Issues identified
Examination of the data has shown that some managers, including those usually classed as
Very Senior Managers (Board level staff such as Chief Executives, Chairpersons, Finance
and Nursing Directors etc.) are appearing under another Occupation Code grouping that is
not usually shown in our publication, those Occupation Codes starting with Z.
We can identify these staff by looking at their Job Role, their (usually) non-AfC grade and
their earnings.
It is likely that they have been included in the Z group because the second note
accompanying the Z code matrix says:
‘2. Code Z2E includes Chairmen and other non-executive board members. Please do
not code these staff to the G matrix.’
Another issue is that there may be other staff with Z Occupation Codes that are of interest to
users. Appendix E contains a list of the Organisation type, Area of Work, Occupation Code
classification, Job role and grade of such staff.
Our proposal
We propose that senior managers with an Occupation Code starting with Z are included in
our published figures. Criteria based on grade and earnings will be used to double check
where such staff appear to be very senior managers.
In addition, other staff that users agree should be included in our figures who currently aren’t
because they have a Z Occupation Code may also be incorporated into published figures.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
12
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Possible impact
Inclusion of very senior managers with Z Occupation Codes will increase staff numbers
within that group and permit more accurate statistics to be published.
Feedback sought
Should Chairpersons be included in the Senior Manager figures we publish – either as a
separate group or within the existing Senior Manager group? (Job roles suggest that at least
60 are already included in the existing group but these are not coded using Z codes.)
Should staff that we believe from the available data to be Managers or Senior Managers but
who have an Occupation Code starting with Z, be re-classified and included in our published
figures?
If so what grade and earnings criteria are appropriate? For example, staff with appropriate
job roles, a grade higher than 8b or with a non AfC grade and earnings higher than £45,000?
If users are interested in information on these staff being more readily available then please
let us know.
15) Type of contract
Within the ESR Data Warehouse the ‘Assignment Type of Contract’ field provides
information on each role’s type of contract, Permanent or Fixed Term Temporary for
example.
We currently include several contract types in our published NHS staff numbers that appear
unusual.
These are:
Honorary
Non-Exec Director/Chair
Prof Exec Committee
Retainer Scheme, and
Widow/Widower
Issues identified
The ‘Non-Exec Director/Chair’ is included despite the Occupation Code for such roles
currently being excluded from our published data. This suggests that some trusts are coding
these staff differently to those that use Z Occupation Codes and relates to the Very Senior
Managers and Z Occupation Codes section above.
If Non-Executive Directors should be excluded, in respondents’ opinions, and Chairpersons
should be included in our figures, there are Job Role values that could be used to achieve
this.
We believe that the ‘Widow/Widower’ category is used as a mechanism to pay the bereaved
spouse of a deceased staff member if that situation becomes necessary, in which case it
seems sensible to exclude this very small number of records from our figures.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
13
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Our proposal
We propose to exclude Honorary, Prof Exec Committee, Retainer Scheme, Non Exec
Directors and Widow/Widower staff from published statistics and act on the response to our
questions above relating to Chairpersons.
Possible impact:
Honorary -380 records
Non-Exec Director/Chair -60 records
Prof Exec Committee -14 records
Retainer Scheme -265 records, and
Widow/Widower -5 records.
Feedback sought
We would appreciate opinions and information on the use and inclusion of ‘Honorary’, ‘Prof
Exec Committee’, ‘Retainer Scheme’ and ‘Widow/Widower’ contract types in our
publications. These staff are currently counted if they have an occupation code we include in
our figures.
16) Nurse Learners
We do not have data on student nurses as a whole; they are mainly university students and
recorded on systems we have no access to. However there is a set of Occupation Codes
covering Nursing, Midwifery and Health Visiting Learners. Currently these staff
(approximately 4,000) are classified within the Support to Doctors and Nurses staff group.
Issues identified
Although this group sounds like a classification of student nurses, there are three levels of
Nurse Learners and only one relates to staff with no nursing registration. Two levels relate to
existing qualified nurses who are training for additional registration, for example in Midwifery,
Health Visiting or District Nursing.
Our proposal
We propose that in the future only the non-registered group (around 1,200 staff with an
Occupation Code starting with P1) continue to be included in the Support to Doctors and
Nurses staff group, but the other two groups (around 2,800 people in Occupation Codes
starting with P2 or P3) that include qualified nurses, should be included in the Qualified
Nurse staff group.
Possible impact
This change would impact on previously published figures. We would address this by
producing amended time series. If these were included there would also need to be a new
definition of the qualified nurses group.
Feedback sought
We would like opinions on whether or not including qualified nurses who are in training in the
Qualified Nurses staff group is a sensible suggestion.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
14
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
17) Occupation Code to grade mismatch
The HSCIC processes raw ESR Data Warehouse data to produce an enhanced set of data
for publication and runs data quality reports to highlight issues within the records in ESR and
report them to Trusts. However there are still anomalies and inconsistencies within the data.
Issues identified
One of these is addressed in the earnings publication which was developed after the monthly
staff in post publications and added more intelligence to guide our assessment and use of
the data.
In the processing of the earnings data – which has shown that the AfC band of a person is a
very accurate field – we look for an alternative classification of any record where the grade
does not match the role. So if the Occupation Code suggests an individual is a nurse, but he
or she is Agenda for Change (AfC) Band 3 with a Job Role listed as Health Care Assistant,
then we replace the nurse Occupation Code for the record with a Health Care Assistant one.
We believe the process should be applied to all other data that we use to produce statistics.
However, there is an issue due to the difference between staff in post and earnings statistics.
For staff in post statistics, we endeavour to count all staff. For earnings statistics, which are
usually averages, we discard records where the data quality appears to be compromised
(e.g. a Band 2 Senior Manager with a Senior Manager Job Role would be dropped).
This does not compromise earnings estimate figures because we are calculating means from
huge numbers of records (around 13.9 million for some figures) and from very high samples
of the available population (always above 95%).
For staff in post, where the sample size is the statistic, dropping any record may be
inappropriate; there may be an issue with the classification of what they do, there still may be
useful data on what they are, which can be used in other statistics. For example, although
we may not know what she does, knowing that the person we don’t think is a Senior
Manager is a Band 2 white female is useful when we want an overall picture of equality in
the NHS.
Our proposal
We propose that we apply the checks on appropriate grade to all workforce statistics and
where we would normally exclude a record from the Earnings statistics for data quality
reasons, we now reclassify the person to ‘Unknown Job Classification’ or ‘Unknown Staff
Group’ in the staff in post statistics (or another ‘Unknown’ classification that people think
works well).
The current Earnings process as it would be applied to staff in post figures is shown in
Appendix A.
Possible impact
Although this should not affect overall staff numbers it will increase the number of staff we
cannot assign to a staff group, however that and the reclassification of staff to more
appropriate staff groups should increase the accuracy of the statistics produced.
Feedback sought
Does our proposal seem acceptable and sensible?
Are there additional clues to staff group within the ESR Data Warehouse that could be
employed to enhance our methodology?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
15
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
18) Staff groups
Figure 1 shows the groupings of staff in the annual workforce census next to the groupings
used in our monthly staff in post and earnings publications.
The annual census figures normally include primary care staff but these have been removed
here to facilitate comparison.
Figure 1
Annua l Ce nsus
Monthly Sta ff in Post a nd Ea rnings
Tota l HCHS m e dica l a nd de nta l sta ff (incl HPCAs)
Tota l HCHS non-m e dica l sta ff
Tota l
Professionally qualified clinical staff
Profe ssiona lly qua lifie d clinica l sta ff
All doctors
2
(1)
All HCHS doctors (incl locum s)
Consultants (including Directors of public health)
Registrars
Other doctors in training and equivalents
Hospital practitioners and clinical assistants (non-dental specialties)
Other medical and dental staff
All HCHS doctors (non locum )
Consultants (including Directors of public health)
2
Registrars
Other doctors in training
Hospital practitioners & clinical assistants
Other medical and dental staff
Tota l qua lifie d nursing sta ff
3
Qualified nursing, midwifery & health visiting staff
Tota l qua lifie d scie ntific, the ra pe utic & te chnica l sta ff
Qualified Allied Health Professions
Qualified Healthcare Scientists
Other qualified scientific, therapeutic & technical staff
Qua lifie d a m bula nce sta ff
4
All HCHS doctors (locum )
Consultants (including Directors of public health) - locum
Registrars - locum
Other doctors in training - locum
Hospital practitioners & clinical assistants - locum
Other medical and dental staff - locum
Tota l HCHS non-m e dica l sta ff
Qua lifie d nursing, m idwife ry & he a lth visiting sta ff
Qualified midwives
Qualified health visitors
Qualified school nurses
Support to clinical staff
Support to doctors & nursing staff
Support to scientific, therapeutic & technical staff
Support to ambulance staff
NHS infrastructure support
Tota l qua lifie d scie ntific, the ra pe utic & te chnica l sta ff
Qualified allied health professions
Qualified therapeutic radiography staff
Qualified diagnostic radiography staff
Qualified speech & language staff
Qualified healthcare scientists
Other qualified scientific, therapeutic & technical staff
Central functions
Hotel, property & estates
Manager & senior manager
Other non-m edical staff or those with unk nown classification
Qua lifie d a m bula nce sta ff
Support to clinica l sta ff
Support to doctors & nursing staff
Support to scientific, therapeutic & technical staff
Support to ambulance staff
NHS infra structure support
Central functions
Hotel, property & estates
Senior managers
Managers
Issues identified
The monthly groupings include locums although that could alter depending on the outcome
of this consultation.
Subsequent tables in both publications offer further splits and groupings of non-medical and
medical staff. As an example some groupings, such as the specialty groupings in Table 1 of
the existing Medical & Dental Census publication detailed statistics, have existed for many
years.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
16
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Detailed medical statistics:
http://www.hscic.gov.uk/catalogue/PUB13740/nhs-staf-2013-med-dent-detl-tab.xlsx
It has been suggested that we should create a categorisation that would identify ‘Frontline
NHS Staff’.
We appreciate that we have not provided clear suggestions of possible staff groupings in this
part of the consultation, this is because we want user input. However, we welcome
discussions with users who would like to discuss how existing groups are defined and what
other groupings are possible. (Please see how to engage with us at the end of this
document.)
Our proposal
Users should consider whether the staff groups currently provided in each of our publications
meet their needs, are clear and consistent enough, and whether there are changes that
would improve the usefulness of the statistics.
Possible impact
This issue requires careful attention and broad consensus. Revised time series can be
constructed if new groupings are agreed upon.
Feedback sought
Are the staff groupings published still relevant and useful?
Would a ‘Frontline NHS staff’ category be useful and which staff groups should be included?
If you like the current groupings and would like them to continue then you need to tell us or
they may be changed based on feedback from others.
We are happy to directly engage in discussions to provide further information regarding
alternative groupings. The NHS Networks forum may also be a good place to discuss and
consider other views on what is useful.
19) Area of Work and Job Role
Currently workforce statistics are categorised by staff groups, with doctors shown by grade
and specialty within their group.
Non-medical staff can be shown by type of job, a broad classification (level) within that job,
and then broadly the area they work in. These details are contained within the Occupation
Code. So a Nurse Occupation Code might denote someone is a Children’s Nurse and work
in the Acute, Elderly & General area or that they are a Health Visitor working in Community
Services.
The Occupation Code is well established and subject to a high degree of governance
concerning definitions and development, which is why it is used as a reliable standard.
Issues identified
There are other classifications available in ESR which offer additional insight to the NHS
workforce. (2 Trusts do not use ESR).
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
17
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
These classifications are Job Role and Area of Work (AoW). (Note: AoW is not the same as
the part of the Occupation Code called ‘Area’.)
For example, at the moment if someone wants to know how many Receptionists are in the
English NHS from our current publications we can only say from the Occupation Code how
many Admin and Clerical staff there are. By using Job Role, we could identify Receptionists.
Combining this with AoW could tell us how many Receptionists worked in an Accident &
Emergency (A&E) area. Current publications do not provide that detail.
We do provide information using AoW and Job Role to customers on request. In particular
the A&E AoW has been of interest recently.
Area of Work is available at three levels:
Primary – in our opinion this doesn’t deliver enough distinction between areas
Secondary – a more detailed, useful level of detail
Tertiary – a very detailed split of AoW
Publishing by the 18 categories of Primary AoW would not give A&E, for example.
One of the problems of publishing by Secondary AoW is that it has at least 160 groups.
Tertiary has at least 308. There are currently around 8,200 combinations of Secondary AoW
and Job Role and around 11,500 combinations of Tertiary AoW and Job Role.
Combining Job Role, AoW, Occupation Code and possibly other fields makes it difficult for
clear static tables to be produced that convey the information a wide variety of users may
require.
Examples of what is available within these two fields of the data are shown in Appendix C.
Our proposal
We believe that there will be interest in seeing published statistics which use AoW and Job
Role and that the HSCIC should begin to include these in published statistics.
Practically we would prefer to publish Secondary level AoW, but Tertiary and Primary levels
would be available on request.
Within the monthly staff in post publications, similar challenges have been dealt with by
using the flexible format of pivot tables within an Excel spreadsheet to allow users to access
an overall table that they can then explore further to focus on their statistics of interest.
Possible impact
Misclassification of Occupation Code and our attempts to rectify them have already been
mentioned. There are not the same broad structures in the Job Role field which allow the
same sort of validation. We can build rules with Occupation Code and grade to validate a
Director of Nursing appearing as a Band 4 but there is no formal classification of a senior
manager group within Job Role which allows simple validation. Such processes could be
developed but would take time and consultation.
Similarly, AoW does not lend itself to simple validation. Maternity within a Mental Health
Trust, for example, may seem unusual but isn’t necessarily impossible.
We do not have a full appreciation of the quality of the data in these fields, but introducing
AoW and Job Role into the publications may help increase the understanding of the data as
a whole.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
18
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Feedback sought
We would appreciate opinions on the use of Area of Work and/or Job Role in future
workforce publications.
The main questions are:
Are they of interest?
If so, what are the main areas of interest?
If so, what level of AoW would be preferred?
20) Grades for non-medical staff
The number of doctors in each grade is a longstanding feature of NHS workforce statistics.
With the introduction of Agenda for Change to provide a standard grade structure for the vast
majority of the NHS workforce and the introduction of ESR shortly afterwards to provide
good quality data we now have the ability to provide information on the grades of nonmedical staff. (The 2 NHS trusts not using ESR currently provide good quality data on staff
grades once a year.)
Grade for non-medical staff has not previously been a feature of either our monthly, quarterly
or annual publications although we have provided this information in response to enquiries
and the ability to provide grade information has been central to the work we have produced
on equality in the NHS. (http://www.hscic.gov.uk/catalogue/PUB13951/nhs-work-stat-oct2013-equal-div.xls - for example.)
Issues identified
From the enquiries that we provide bespoke figures for, we believe that there is demand for
grade information in our statistics. However the requests that we receive usually require
such specifically defined figures that a ‘general’ set of grade tables may not answer them.
Our proposal
We propose to publish numbers in each staff group by grade in each census publication.
It may be possible to include this information in a graphing tool.
Possible impact
Including grade information could make some tables 13 times bigger and any time series
would only go back to around 2009.
Feedback sought
Is there a general demand for grade information?
Do users want regional figures?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
19
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
21) Updating the Medical Grades
The grades we classify doctors as include grades that are now obsolete.
This list shows the current grades:
Consultant (including Director of Public Health)
Associate Specialist
Specialty Doctor
Staff Grade
Registrar Group
Senior House Officer
Foundation Year 2
House Officer and Foundation Year 1
Other Doctors in Training
Hospital Practitioner/ Clinical Assistant
Other Staff
This link to the most recent doctor pay circular from NHS Employers identifies a range of
current and closed grades. (Page 4 onwards.)
http://www.nhsemployers.org/~/media/Employers/Documents/Pay%20and%20reward/Pay%
20and%20Conditions%20Circular%20MD%2012015.pdf
Issues identified
We do not believe our currently published set of grades presents the most useful grade
classifications possible.
Our proposal
We will adjust the doctor and dentist grades to reflect user opinion as fed back from this
consultation.
Possible impact
As this should largely involve re defining existing grades impact should be limited to
recreating time series.
Feedback sought
Could the current doctor grade classifications be improved?
If so please identify the grade classifications that would be most useful, if possible with the
“old” grades that fit into them.
From what date would any reclassifications be appropriate? – Would a translation of historic
grades to the current versions be sensible for all past figures or only from when new grades
came into being?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
20
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
22) Ethnic codes
The data we use to produce publications contains good quality information on the ethnic
composition of the NHS workforce and this is routinely reported on in our existing annual
publication and feeds the equality work we produce.
Issues identified
A minor complication within these data is that there are two classification systems used. The
majority of staff use a more recent system. However, a small minority are classified under an
historic system.
This is not a reflection on the accuracy or quality of the data, it just causes slight
inconvenience when working with the data as the two systems do not match perfectly and
this does not provide as clear a picture as we would like.
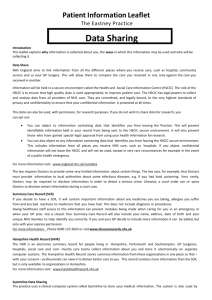
Figure 2 shows the current situation as published for the non-medical workforce.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
21
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Figure 2
Table 9. NHS HCHS: Non-medical staff by ethnic group
England as at 30 September 2013
headcount
Old Ethnic Codes
New Ethnic Codes
Other Unknown1
Other Unknown1
Total ethnic
minority
groups2
All groups
White
Black
Asian
177
317
77
12
21
878,834
12,192
62,198
56,069
3,670
17,041
47,817
14.7%
1,078,425
62
201
45
9
13
415,725
5,879
34,540
31,086
2,414
11,043
19,538
17.0%
520,555
Qualified nursing, midwifery & health visiting staff
33
187
34
7
11
268,776
3,887
24,389
26,662
1,537
9,477
12,944
19.8%
347,944
Total qualified scientific, therapeutic & technical staff
Qualified Allied Health Professions
Qualified healthcare scientists
Other qualified scientific, therapeutic & technical staff
29
12
7
11
14
3
1
10
11
3
3
5
2
2
-
2
1
1
-
129,667
66,913
23,422
39,418
1,842
831
344
669
10,035
3,620
2,723
3,695
4,333
1,490
1,223
1,620
869
265
201
403
1,523
487
452
586
5,782
2,536
1,240
2,012
12.6%
9.1%
17.4%
15.1%
154,109
76,163
29,617
48,429
-
-
-
-
-
17,485
154
120
97
9
46
823
2.4%
18,734
79
64
24
2
2
292,103
4,152
16,683
17,289
652
4,189
13,760
12.8%
348,999
Support to doctors & nursing staff
56
59
18
1
2
227,971
3,232
13,068
14,940
489
3,565
10,743
13.4%
274,144
Support to scientific, therapeutic & technical staff
23
5
6
1
-
51,815
797
3,423
2,219
151
608
2,264
12.2%
61,312
-
-
-
-
-
12,813
127
219
144
15
19
775
3.9%
14,112
37
52
8
1
6
172,915
2,181
11,092
7,816
607
1,822
14,648
12.0%
211,185
11
21
5
3
46
3
3
3
2
1
-
4
2
84,664
58,108
30,299
1,188
708
288
6,057
3,698
1,345
3,676
3,375
774
386
136
86
561
1,128
135
7,577
3,668
3,421
12.3%
13.5%
8.0%
104,130
70,892
36,360
-
-
-
-
-
210
-
-
2
-
-
8
0.9%
220
Total non-medical staff
Professionally qualified clinical staff
Qualified ambulance staff
Support to clinical staff
Support to ambulance staff
NHS infrastructure support
Central functions
Hotel, property & estates
Manager & senior manager
Staff with unknown classification
White
Asian or Black or
Asian
Black
Mixed
British
British Chinese
Notes:
These statistics relate to the contracted positions within English NHS organisations and may include those where the person assigned to the position is temporarily absent, for example on maternity leave.
1. "Unknown" includes unstated and unrecorded ethnic group.
2. Percentages of staff whose ethnic group is known.
Headcount totals are unlikely to equal the sum of components.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
22
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Our proposal
The old ‘White’ category in the left part of the table to be incorporated with the new ‘White’
category on the right part of the table.
The old ‘Black’ category to be incorporated with the new ‘Black or Black British’ category on
the right part of the table.
The old ‘Asian’ to be merged with the new ‘Asian or Asian British’,
the old ‘Unknown’ to be merged with the new ‘Unknown’.
The old ‘Other’ to be merged with the new ‘Other’.
Note: there is no old ‘Mixed’ category and no old ‘Chinese’ category on the left.
Possible impact
We believe that combining the two categorisation systems will not result in any loss of detail
and will produce a more informative table.
Feedback sought
Are there any objections to combining the two ethnicity classifications into a single
classification?
23) Table Structure
Please have a look at the table structure in the national level tables on the first Excel sheet
of the publications at the following links.
Annual workforce census publication:
http://www.hscic.gov.uk/catalogue/PUB16973/nhs-staf-2004-2014-over-tab.xls
Monthly staff in post publication:
http://www.hscic.gov.uk/catalogue/PUB17272/nhs-work-stat-jan-2015-nat-tab.xls
Table 1a from the annual publication and ‘National – Timeseries’ from the monthly
publication show similar statistics; the annual census shows a ten year time series, the other
a monthly time series. (See Figure 2)
Issues identified
Table 1a (annual census) uses four columns to give the staff groups whereas the monthly
publication uses one column. Similarly Table 1a (annual census) also uses a variety of row
widths, the monthly publication one row width.
Both tables leave gaps between row headings and the body of the tables and both leave
gaps in the tables. We have received comments that such tables are hard to sort or create
graphs from without removing the blank rows or altering the columns.
Table 1a (annual) shows headcount only. FTE is on a separate sheet - Table 1b whereas the
monthly publication contains three tables with different measures of the workforce,
headcount, FTE and role count all on one sheet.
The annual census also contains a set of tables which replicate the same information for
headcount and FTE at national and HEE Region level. However the way the annual
workforce census is currently structured means that the tables provided are not all together
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
23
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
in one link. Some statistics are provided under a Medical & Dental link, some Non-medical,
some have combined overall tables (see various links available under Annual workforce
census publication, above).
The monthly publication contains spreadsheets containing 55 tables of staff-in-post
information and an additional 11 tables containing Health Visitor figures and turnover
statistics. A quarterly version of the monthly publication contains at least another 16 tables
including turnover, reason for leaving and redundancy figures.
It is therefore very hard to consult on this mass of tables.
Our proposal
Users should take this opportunity to tell us how we can best present our statistics.
Possible impact
Changes to the traditional layout of our statistics may present frequent users of the figures
with an unfamiliar set of tables. Amendments to tables may increase the consistency and
comparability of tables and may make some tables easier to produce.
Feedback sought
We would appreciate any feedback on how the census and other workforce statistics are
presented and whether the split between the medical and non-medical figures in separate
publications works well.
Is it more convenient to have headcount, FTE and role count in tables on one sheet rather
than three separate sheets?
Would removing the blank rows or standardising the column layout be useful?
It may be that this really isn’t of much concern to you and that in itself is a useful response. If
that is the case in general we will structure the publication to allow the most efficient
production and a simple structure.
The NHS Earnings publications include a graphing tool that uses pivot tables with macros to
create bespoke graphs and statistics, specifically the earnings graphing tool.
http://www.hscic.gov.uk/catalogue/PUB14955/nhs-staff-earn-march-2014-provisional-basicpay-grapher-sept-14.xlsm
This tool uses a set of processed earnings data from the ESR Data Warehouse and allows it
to be queried to automatically create statistics and histograms showing the distribution of
earnings for staff groups and regions.
Would such tools be useful for staff in post figures – perhaps grade distributions by region? If
so what kind of figures would benefit?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
24
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
24) Tables Provided
The tables provided in the annual workforce census reflect the tables produced before ESR
was in place and before Agenda for Change was implemented.
The staff in post tables produced on a monthly basis were created after ESR was in place,
following a consultation, and have since further evolved to reflect user needs. These are
provided again below.
Monthly staff in post publication:
http://www.hscic.gov.uk/searchcatalogue?productid=17709&topics=1%2fWorkforce%2fStaff
+numbers&sort=Relevance&size=10&page=1#top
The annual workforce census tables are available at the following links:
Summary tables (annual workforce census)
http://www.hscic.gov.uk/searchcatalogue?productid=17425&topics=1%2fWorkforce%2fStaff
+numbers&sort=Relevance&size=10&page=1#top
Medical Tables (annual workforce census)
http://www.hscic.gov.uk/searchcatalogue?productid=17382&topics=1%2fWorkforce%2fStaff
+numbers&sort=Relevance&size=10&page=1#top
Non-medical Tables (annual workforce census)
http://www.hscic.gov.uk/searchcatalogue?productid=17386&topics=1%2fWorkforce%2fStaff
+numbers&sort=Relevance&size=10&page=1#top
In the annual workforce census, the national summary tables called 1a (Headcount) and 1b
(FTE) are repeated in every subset of the publications. These contain Primary Care staff not
shown in the monthly figures.
Issues identified
Some of our annual staff census tables have not changed for years, we would like to know if
they are still widely relevant.
Our proposal
We propose that future publications will include tables which have been widely requested by
users.
Possible impact
New tables that use the extra detail that ESR allows may only go back to 2009 rather than
the traditional 10 year time series.
Feedback sought
If you wish us to publish new tables please let us know and if you want to discuss what is
possible please contact us.
We have created the discussion spaces to allow people to debate priorities. (See Appendix
F)
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
25
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
25) Bulletin Contents
Please have a look at the various bulletins provided with the census.
Overall
http://www.hscic.gov.uk/catalogue/PUB16973/nhs-staf-2004-2014-over-rep.pdf
Non-medical
http://www.hscic.gov.uk/catalogue/PUB16933/nhs-staf-2004-2014-over-rep.pdf
Medical
http://www.hscic.gov.uk/catalogue/PUB16931/nhs-staf-2004-2014-over-rep.pdf
Issues identified
We are reviewing the commentary in all our workforce publications to ensure they meet user
needs.
Our proposal
We would like user input to help us focus our written accompaniment to our publications.
Possible impact
Unknown.
Feedback sought
Do you use the information provided in the bulletins we provide with publications?
Would you like to see more information in this part of the publication and if so as tables,
graphs, bullet points or some other method of illustration?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
26
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
26) GPs in the Hospital & Community Health
Service figures
There are three areas where there is overlap between the GP workforce census currently
published at the same time as the (HCHS) annual workforce Census:
Primary Care staff in the secondary care figures
Issues identified
A pilot scheme to collect individual level data from GP practices received some responses
saying that their data was already in ESR. (See the connected Primary Care workforce
consultation http://www.hscic.gov.uk/consultations)
Further investigation has shown that more than a thousand likely Primary Care staff are
included in our published figures. Most of these are shown as working at NHS Trusts, with
very few being shown as being hosted at those trusts on behalf of another organisation.
There is no simple, accurate way of identifying Primary Care staff within ESR data and only
basic methods to find them have been used to find a sample set. Furthermore, even within
this set definitional issues remain. Some staff clearly appear to work at a Primary Care site,
but could be nurses or GPs funded by the secondary care Trust as part of a community
health program. Similarly, there are also people who are paid through the Trust who are
receptionists at Primary Care sites.
Our proposal
We propose to use the Primary Care Workforce Minimum Data Set (PCwMDS) to exclude
staff counted in that collection from HCHS figures. This will avoid double counting and
inappropriate classification of staff.
Possible impact
Primary Care staff would also be excluded from turnover statistics and our Earnings and
Absence publications.
The exclusion would lead to the more accurate classification of staff but will cause an initial
reduction in the HCHS workforce figures. We do not anticipate this would be a major
reduction.
Feedback sought
Is it appropriate to reclassify these staff or are they correctly operating as an arm of
secondary care providers?
Will this reclassification cause issues for users?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
27
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Hospital Practitioners and Clinical Assistants and GPs
The second overlap between the Primary Care workforce and the HCHS workforce is that
traditionally Hospital Practitioners and Clinical Assistants (HPCAs), a type of secondary care
doctor grade, have always been regarded as GPs or Dentists who have a role in a
secondary care setting.
As such, when the HCHS workforce is counted they are, correctly, included in those
numbers. However whenever a figure giving the total number of doctors in the NHS in
England is published (effectively HCHS doctors plus GPs), the headcount numbers of HPCA
doctors (but not HPCA dentists) are excluded. This is to avoid double counting.
Full Time Equivalent numbers are not changed because these are not unique counts.
Issues identified
Matching Primary Care workforce data to corresponding HCHS data shows that not all
medical HPCAs are also counted in the Primary Care census.
Our proposal
We suggest that rather than automatically excluding medical HPCAs from the all doctors
total we exclude only those where we identify an HPCA in the GP workforce by matching
GMC numbers between the two sets of data.
Possible impact
The effect of this change when carried out on September 2013 data would be to add
approximately 250 headcount to the total NHS doctors.
Feedback sought
Is this an appropriate way of handling the data?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
28
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
GPs working in secondary care
The third area where Primary Care workforce and HCHS statistics overlap involves the
second Medical and Dental sheet of the Occupation Code Manual (the guide on how to
classify staff in the NHS).
http://www.hscic.gov.uk/article/2268/NHS-Occupation-Codes
Issues identified
Doctors with an Occupation Code (often referred to as a specialty code for doctors) of ‘800’
are HCHS doctors who are being paid by a trust on ESR whilst they do a placement in a
Primary Care setting as part of their training.
At the moment these doctors are not included in the Primary Care Census but are included
in the HCHS figures.
However doctors with an Occupation Code of ‘921’ are, according to the Occupation Code
manual, Primary Care doctors who are being employed by a secondary care trust. ‘971’
codes are Primary Care dentists similarly employed.
There are many scenarios where the presence of Primary Care staff in a secondary care
setting make sense. However, traditionally, these staff have not been counted in HCHS
figures - the only place where these staff are counted is in the Primary Care census. Any
‘921’ doctor who does not show up in the GP data is taken from ESR records and added to
the GP data.
Our proposal
We propose that doctors with a specialty code of ‘800’ remain in the HCHS figures and that
the ‘921’doctors and ‘971’ dentists are now also counted in all HCHS statistics. This would
include earnings.
Possible impact
Where all doctor totals are provided, they would be treated in the same way as HPCAs are
(i.e. removing the headcount of all those who already show in the GP data).
The suggested action would increase the number and FTE of doctors in HCHS figures and
there would consequently be issues on how these doctors should be classified and at which
grade.
Feedback sought
We would like comments on whether the counting of such doctors and dentists in HCHS
statistics makes sense, and if so what grade they should be or how they should be classified
or described.
They already have grade codes which suggest grades but it may make more sense to
allocate a standard grade to the Occupation Code. As they are thought to be Primary Care
doctors or dentists, it might be odd to think of them as Consultant GPs or Consultant
Dentists, for example.
They could be included within the HPCA group, a grade which already accommodates GPs
and dentists or be referred to as General Medical Practitioners, General Dental Practitioners
or Primary Care Practitioners.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
29
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
27) Should we drop the Role Count?
The annual workforce census publication does not include role count, whereas the monthly
staff in post publications do.
Role count is a measure of workforce numbers. Rather than a person count it is effectively a
job count and if someone is doing two roles in two different trusts, it would count those two
roles at national level where headcount would count one person.
Issues identified
We are unsure how useful role count is, at least as a regular measure alongside headcount
and FTE. However sometimes it is a useful way of understanding issues, for example Table
1 in the Jobs or people? section of this consultation.
Our proposal
We propose that we revert to headcount and FTE only in the monthly publications and
discontinue role count.
Possible impact
This will reduce the size of the publications a little.
Feedback sought
Are there any issues with dropping role count from the monthly staff in post publications?
28) Workforce Minimum Data Set (extended ESR
Data Warehouse download)
To fulfil the requirements of Health Education England, NHS England and the Department of
Health to understand and plan the health care workforce the Health and Social Care
Information Centre is launching additional and enhanced data collections, collectively known
as the workforce Minimum Data Set (wMDS). One of these is the Primary Care wMDS.
Another element of this will be an extended download from the ESR Data Warehouse with
additional fields requested by users of the data. The full list of fields from the ESR element of
the wMDS with descriptions is provided in Appendix D.
Issues identified
This larger data set will provide additional potential to understand the workforce, subject to
the completeness and quality of the data.
Our proposal
We will work to assess the completeness, accuracy and utility of these additional ESR fields
and use them to add value to our published statistics wherever possible.
Feedback sought
It would help us if users of our statistics looked at the available fields and let us know
whether there are additional useful statistics that the data might allow us to provide.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
30
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
29) Workforce Minimum Data Set (data from other
providers)
In addition to the data from existing sources the scope of the HSCIC’s health workforce
publication is being extended to cover organisations providing NHS funded services. This will
collect data from Social Enterprises, Community Interest Companies, Hospices and the
Independent health care sector amongst other providers. These collections will be carried
out every 6 months with the first scheduled for the end of March 2015.
Quarterly collections will be made from the two NHS trusts that do not use ESR with an
extended list of data items.
The list of data fields to be collected with descriptions is provided in Appendix D.
Issues identified
There are issues with identifying and communicating with the appropriate organisations
which will affect the coverage of any statistics produced.
The classification system for staff that is well embedded in NHS organisations is new to the
new data providers.
Some of the organisations are existing providers of workforce information as their data is
within the ESR pay system. These are Social Enterprises, Community Interest Companies
and any non NHS providers using ESR.
The HSCIC has previously received a request from one of these to exclude their data from
our NHS workforce publications with the understanding that the data may be used in the
Workforce Minimum Data Set figures when they are published.
With the creation of a separate set of statistics which can include these organisations they
will be reclassified and their data removed from NHS workforce statistics.
Our proposal
We will endeavour to produce aggregated statistical tables for non-NHS providers that
replicate as closely as possible the figures that we produce for the NHS, as informed by this
consultation, where possible producing overall figures for staff groups for England.
Possible impact
These are the first steps towards another level of health care workforce information and we
will provide the best statistics we can, with appropriate caveats.
The re classification of some organisations currently included in NHS workforce statistics will
have reduce staff in post figures by approximately 21,500 headcount and 17,500 FTE. This
reclassification will also impact on Sickness Absence, Earnings and Turnover statistics
Feedback sought
Are there useful statistics or knowledge that the extension of the collection to the non NHS
sectors would make possible? For example we would in the long term hope to publish an allEngland count of nurses as a matter of course as an extension of what we currently publish.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
31
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
30) Organisations which should be included in
our statistics
Currently there are central organisations with data on ESR that are counted in HSCIC’s
HCHS statistics, for example NHS England and the HSCIC who are no longer NHS
organisations as they are Non Departmental Public Bodies.
Issues identified
Is it appropriate to count such organisation’s staff within HCHS statistics?
If so are there other organisations that are integral to the operation of the NHS, that may or
may not use ESR, but which should also be included, such as the Care Quality Commission,
Nice, Monitor, the NHS Trust Development Authority and Public Health England?
Our proposal
We propose that the statistics continue to include the existing set of organisations. However
we are providing this opportunity for users to provide their own opinions on the exclusion and
inclusion of both existing and additional organisations.
Possible impact
Inclusion of some of these organisations would largely increase administrative staff numbers,
although they also contain other staff types. It is possible that there are more appropriate
platforms for the publication of staff numbers for some of these organisations, for example
Public Health England in Public Health statistical publications.
Feedback sought
Which organisations should be included in HCHS workforce statistics?
A useful list of organisations is given on this site
https://www.gov.uk/government/publications/how-to-contact-department-of-health-armslength-bodies/how-to-contact-department-of-health-arms-length-bodies
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
32
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
31) Discontinuation of the Health Visitor Minimum
Data Set tables
Tables reporting on the Government’s progress towards their targeted increase in the
number of Health Visitors have been added to our monthly staff in post publication since
2012. As the deadline for this target passed in March 2015 we will publish figures up to the
end of June 2015 (which will be published in September 2015) and then discontinue the
publication of these tables.
Our proposal
As the deadline for this target passed in March 2015 we will publish figures up to the end of
June 2015 (which will be published in September 2015) and then discontinue the publication
of these tables.
Possible impact
The figures in these tables will no longer be available, although the majority of the staff in
post figures were already reported in our monthly statistics and the extension of the scope of
our workforce collections through the workforce Minimum Data Set should begin to collect
similar information from the non NHS Health Visitor employers.
Feedback sought
Will the discontinuation of these figures create issues for users?
32) England and Wales cross border counting
A minor issue is how staff working near the Welsh border are counted.
Issues identified
Staff employed by an NHS organisation in England but shown as working in Wales are
excluded from our statistics.
Staff shown as employed in Wales but working in an NHS organisation in England are also
excluded from England’s figures.
Our proposal
We anticipate that the current methodology slightly undercounts staff providing NHS services
in England along the Welsh border. We propose that we ask the Welsh Government to
permit us to use their data to identify any cross border workers and reciprocate the
arrangement.
Possible impact
Possibly a small increase in the staff numbers at some trusts.
Feedback sought
Should both types of staff be excluded?
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
33
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
33) Earnings
quarterly
publications
to
be
published
Recently we increased the frequency of our NHS Earnings publications from quarterly to
monthly.
http://www.hscic.gov.uk/searchcatalogue?topics=1%2fWorkforce%2fStaff+earnings&sort=Da
te&size=10&page=1#top
Issues identified
As the earnings figures are rolling 12 month averages we are not convinced of the benefits
to users of a monthly rather than quarterly publication.
Our proposal
We propose to resume a quarterly pattern for the earnings publication.
Possible impact
A maximum of 2 months’ delay in one set of figures if the frequency changes to quarterly. No
information will be lost through this change.
Feedback sought
Do users require earnings statistics quarterly or would publications 4 months apart or 6
months apart be satisfactory?
34) Have we missed anything?
If you have any thoughts on how we can improve what we currently do or how we can
provide new statistics that would be useful, please tell us.
There are limitations to the data that are not necessarily apparent until further investigation
has been undertaken. It is possible that certain types or analysis or output are simply not
possible given the constraints of the available data.
We are keen to benefit from your intelligence so if you have an idea please suggest it or talk
to us first if that seems more sensible.
There will be a separate consultation relating to Absence statistics but we are happy to hear
ideas about that area if you have any comments now.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
34
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
35) Summary
The HSCIC is working to extend the scope of existing Health and Community Health Service
workforce statistics to beyond just NHS employed staff.
The HSCIC is taking the opportunity of this development to review its existing staff in post
publications in terms of how statistics are presented, which staff are counted, how those staff
are defined and the criteria used for counting them.
We are seeking input from users to ensure that our future publications deliver what users
need to understand the health care workforce.
We will act on good suggestions that come about from this consultation and improve our
products whenever we see an opportunity to do so, but this will need to be balanced against
delivering the full range of services expected from us and changes may need to be phased
in as data of sufficient quality becomes available.
36) Next steps
Please consider the issues raised:
If you wish to discuss any issue, or talk through something that we haven’t explained clearly
then contact us directly or use the NHS Networks discussion group to engage with other
respondents.
We appreciate there are a lot of things to consider and a decision on one can impact on
multiple issues. There are lots of tables for review, so if communicating with us will help
simplify or clarify things we are very willing to engage in conversations.
Comments, opinions, and suggestions gathered from this consultation exercise will help us
finalise the design of publications and tailor the statistics published to user requirements.
Please pass this consultation on to any other parties you believe would be interested.
37) How to respond
This consultation process is open to anyone – whether responding as an individual or
representing an organisation. The closing date for the consultation is 13 August 2015.
A short form version of the issues raised is attached with space for responses, however we
will accept responses sent to us that do not use the response form.
Although we are happy to talk about the proposed developments, we will require a written
submission of your views if they are to be considered as part of the consultation.
Please email comments to
enquiries@hscic.gov.uk
with the subject heading clearly stating ’HCHS Workforce Consultation’.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
35
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Alternatively, if you are unable to respond via email, you can post your
comments/suggestions to:
HCHS Workforce Consultation
Bernard Horan
Room 4 South
1 Trevelyan Square
Boar Lane
Leeds
LS1 6AE
Please ensure that you include your contact details (noting the type of organisation you
represent, if applicable) on any documents you contribute if you wish us to contact you to
inform you of the outcome of the review.
If you have a query regarding how to complete your response, or would like to discuss any
issue in order to respond more constructively, or you require a copy of this consultation
paper in any other format, e.g. Braille, Large Font, or Audio, please contact the HSCIC on:
0300 303 5678 (9am to 5pm, Monday to Friday) or enquiries@hscic.gov.uk
38) Publication of the consultation outcome
An anonymised summary of the responses received will be made available on our website
around September 2015:
http://www.hscic.gov.uk/article/1165/Search-catalogue?topics=1/Workforce/Staff
numbers&sort=Date&size=10&page=1#top
39) Responses: Confidentiality and disclaimer
The information you send us may be passed to colleagues within the HSCIC, other
government departments or related agencies. Even where confidentiality is requested, if a
request for disclosure of the consultation response is made in accordance with the freedom
of information legislation, and the response is not covered by one of the exemptions in the
legislation, the HSCIC may have to disclose the response, in whole or in part.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
36
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Appendix A: Methodology for grade and staff
group mismatch
Existing Earnings publication reclassification of staff based on their Occupation Code
and Job Role proposed for staff in post publications.
Staff with an Occupation Code that indicates they are a Senior Manager but who have
an AfC grade of Band 1 to Band 6 are examined to see what their Job Role suggests
their job is. If the Job Role suggests a more appropriate Occupation Code than Senior
Manager for their grade then the Occupation Code field is amended to the suggested
code.
Staff with an Occupation Code that indicates they are a Nurse but who have an AfC
grade of Band 1 to Band 4 are examined to see what their Job Role suggests their job
is.
If the Job Role suggests a more appropriate Occupation Code then the Occupation
Code field is amended to the suggested code. Enrolled and Registered Nurses are
permitted to have a Nurse Occupation Code and have an AfC grade of Band 4.
Other qualified staff who have an AfC grade of Band 1 to Band 3 are examined to see
what their Job Role suggests their job is.
If the Job Role suggests a more appropriate Occupation Code then the Occupation
Code field is amended to the suggested code.
Those staff for which a more appropriate Occupation Code for the grade is not
suggested by the Job Role field have their Occupation Code changed to ZZZZ and
are classified as ‘Unknown Staff Group’. Their Job Role is changed to ‘Unknown’.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
37
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
Appendix F – NHS Networks details
How to join NHS Networks
NHS Networks is free to join and is open to anyone interested in engaging in discussions on topics
relating to the NHS. If you are interested then please register with NHS Networks
To find out more about NHS networks go to
http://www.networks.nhs.uk/getting-the-most-out-of-nhs-networks-free-services-and-paid-support2013/view
Once you have registered to ask questions or provide opinions about what we are consulting on or
how you think healthcare workforce statistics can be improved go to the Home Page and click in
the box called ‘Share’ and select ‘Find a network’.
This will give an alphabetical index of networks and a search facility above that.
Our network is called ‘Healthcare Workforce Consultation’.
http://www.networks.nhs.uk/
If you would like to engage with us directly please mail bernard.horan@hscic.gov.uk or call
Bernard Horan on 0113 25 47040 (please do not leave a message but email instead and leave
your number for us to call you).
Although you can discuss issues with us directly or others through NHS Networks we will require a
written submission of your final opinions to count towards this consultation.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
38
NHS Hospital & Community Health Service in England workforce statistics – proposed developments
For further information
www.hscic.gov.uk
0300 303 5678
enquiries@hscic.gov.uk
Copyright © 2015 Health and Social Care Information Centre. All rights reserved.
This work remains the sole and exclusive property of the Health and Social Care
Information Centre and may only be reproduced where there is explicit reference to
the ownership of the Health and Social Care Information Centre.
This work may be re-used by NHS and government organisations without permission.
Copyright © 2015, Health and Social Care Information Centre. All rights reserved.
39