AIM 1: We will methodically test and optimize image quality
advertisement

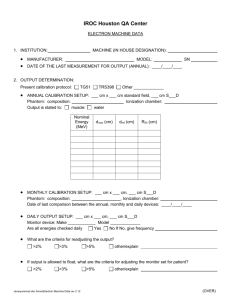
SPECIFIC AIMS Computed tomography (CT) is a valuable diagnostic tool in the evaluation of important childhood diseases, but the exposure to ionizing radiation may increase the risk of cancer. Although infants (children < 1 year-old) are a particularly high-risk group, current CT imaging strategies for infants are often extrapolated by assumptions made with datasets generated from older patients and imaging phantoms specifically designed for adult sizes. Our goal is to study and develop CT imaging tailored for infants. The imaging strategies we develop will offer a substantial reduction in radiation exposure and maintain image quality. Primary Hypothesis: We hypothesize that a highly optimized infant chest CT protocol may be developed using image quality phantoms tailored to infant body habitus. Furthermore, this optimization will produce acceptable image quality while offering a lower exposure to ionizing radiation in infant patients when compared with the current standard clinical protocol. Specific Aim 1: We will methodically test and optimize image quality parameters from chest CT scans performed on infant and adult specific phantoms. We recently developed a novel infant-specific CT phantom that accurately models infant size, density and body habitus. CT scan parameters will be methodically adjusted with the goal of reducing exposure to ionizing radiation while minimizing the degradation of image quality. We will measure CT number, low contrast detectability, spatial resolution, and tube current modulation (TCM) performance. These parameters will be compared among the scans on infant and adult phantoms to determine phantom-specific differences. The optimized chest CT protocol will be defined as one that is comparable to the current protocol across the different image quality metrics, while offering the lowest dose. Specific Aim 2: We will evaluate image quality and patient and organ-specific doses in the clinical application of chest CT imaging optimized for infants. CT examinations from infant patients will be collected before and after optimization of CT parameters based on the phantom work in Specific Aim 1. Expert pediatric radiologists will subjectively assess image quality. Dosimeter measurements will be collected, and through Monte Carlo simulation of the CT datasets, patient and organ doses will be calculated. The image quality metrics, overall dose, and dose to radiosensitive organs will be compared between un-optimized and optimized CT protocols. We anticipate that the optimized protocol will offer comparable image quality to the standard protocol, while providing a reduced exposure to ionizing radiation. BACKGROUND AND SIGNIFICANCE CT is an increasing source of radiation exposure for pediatric patients, and the factors available for lowering exposure and optimizing image quality remain relatively untested. A pressing need exists to minimize exposure of infants to ionizing radiation. Children less than one-year old are a particularly high-risk group for developing cancer after radiation exposure due to their rapidly growing tissues, wider distribution of active bone marrow, and longer post-exposure life expectancy.2 These factors coupled with the increasing utilization of computed tomography (CT) in the pediatric population3,4 emphasize the goal of developing imaging practices that deliver ionizing radiation as low as (is) reasonably achievable (ALARA principle). 5 The goal of the work outlined in this grant is to study and develop optimized CT methodologies for the at-risk infant population. Several factors emphasize the need for further research in this area. Research focused on CT dose reduction in children often encompasses the full pediatric age range from 0-18 years, and a tailored methodology for infants is often extrapolated by assumptions made with datasets generated from older patients and imaging phantoms specifically designed for adult sizes.6,7 An infant specific protocol definition and dose information is necessary, however, due to the significantly different size and shape of infants compared to older children. In 2011 the National Institute of Biomedical Imaging and Bioengineering released effective dose (ED) goals for routine CT exams of “less than 1 mSv”.8 Although initially intended for the adult population, current ED values for children <1 year-old still fall short of this target, with a recent study finding a range of 1.9-19.0 mSv for neonate abdomen CT.9 This wide range also highlights the variation among practices at different institutions, and the general need for dose optimization.10 The standard methodology used to determine radiation exposure during CT also does not account for the unique features of neonates and infants. Although CTDI and DLP are the standard dose outputs from Phelps – Infant CT 1 diagnostic CT scans, they are widely regarded as suboptimal, as they are computed using cylindrical acrylic phantoms, and are inaccurate for patient size, shape, and location of the organs in the scanned region.11 This inadequacy is compounded in children since 1) neonatal and infant sizes are far removed even from the smaller of the two phantoms sizes (16 and 32 cm diameter) used for console dose display and 2) the use of tube current modulation (TCM) gives uneven dose along the scan length, which is not captured by the scanaveraged CTDI provided by the CT console. Multiple parameters on modern CT scanners help modulate exposure to ionizing radiation and also enhance or subtract from image quality (Table 1). However, how trade-offs among these scan parameters influence radiation exposure and image quality remain largely unstudied in the infant population. This is also compounded by new scanner technology such as sophisticated image reconstruction techniques5,12-14 that although promising are yet to be fully tested and validated in the pediatric population. We estimate that in 2012 over 28,600 CTs were performed in infants treated at 49 top children’s hospitals in the United States8 and this number does not take into account many other facilities, which may treat and image infants, so the impact of this work is substantial. PRELIMINARY STUDIES A previous study has demonstrated the need for dedicated infant specific phantoms for image quality analysis (Figure 1). We have developed an infant specific phantom that accurately models the infant body habitus and have gathered preliminary data on image quality (Figures 2-3). We have tested the virtual scanner on several pilot datasets and initial dose distribution maps (Figure 4) appear in agreement with previous reports using this technology.15,16 Table 1. Key CT parameters that affect radiation exposure and image quality Tube potential (kV) Tube current (mA) Tube current modulation (TCM) Beam collimation Rotation time Helical pitch Image quality reference level Reconstruction algorithm Figure 1. Line plots show the variation in a) image noise and b) iodine CNR for different phantom sizes and tube potentials. Large variation in these image quality parameters is apparent at 80 kV, highlighting the requirement of a dedicated small diameter phantom for representative image quality assessment at this tube potential. Reproduced with permission from Siegel et al Radiology 2004;233:515-22.1 RESEARCH DESIGN AND METHODS The proposed research, with the goal of fully understanding and optimizing infant chest CT, can be defined via two distinct aims. The first involves a parametric phantom experiment in order to derive an optimized clinical protocol. Following this, the optimized protocol will be evaluated clinically in terms of image quality and radiation dose in order to establish its efficiency and reliability. The clinical scans will also be simulated using a Monte Carlo approach, allowing insight into how protocol parameters such as the TCM affect image quality and patient dose. AIM 1: We will methodically test and optimize image quality parameters from chest CT scans performed on infant and adult specific phantoms. Hypothesis: We hypothesize that a highly optimized infant chest CT protocol may be developed using image quality phantoms tailored to infant body habitus. RATIONALE: Current CT parameters used to image infants generally assume a weight-based adjustment from phantom work that simulates larger patients and clinical experience/practice. To the best of our knowledge CT protocols have yet to be optimized with specific phantoms that take into account the unique body habitus of the infant (age <1 year-old). This is a particularly important demographic to focus on reduced exposure CT protocols, as lifetime cancer risks attributable to CT for a 1 year old have been estimated as an order of magnitude higher than the adult value.17 To the best of our knowledge no infant specific CT phantom exists that provides these parameters, which are essential for CT protocol development. The protocol we develop will then be tested in patients (Specific Aim 2). The smaller size and lower attenuation of infants are not well represented by current phantoms, but Phelps – Infant CT 2 adjustments in CT protocols based on patient weight are commonly assumed. For example, the QRM image quality phantom series (QRM, Moehrendorf, Germany) have a suitable diameter of 100 mm, but some inserts are inappropriate as they are designed for use within a larger phantom, and to our knowledge no TCM phantom exists. Furthermore, size-specific dose estimates (SSDE) have recently been proposed to adjust for the differences in body morphology between adults and children; however, rather than a protocol optimization tool, the SSDE are a post scan conversion tool. Thus, we do not know of any complete image quality phantom set that accounts for differences in children and adults. Attempting to evaluate the image quality of these low-dose protocols using adult-sized phantoms would result in unrealistically high image noise and possible photon starvation, as the x-rays would insufficiently penetrate the phantom (Figure 1). The development and image quality testing of a dedicated infant-sized phantom is therefore necessary to ensure accurate and representative protocol development. EXPERIMENTAL DESIGN: We recently created an infant phantom that accurately models the unique shape and size of children <1 year old. The phantom is constructed with inserts to measure CT number, low contrast detectability, spatial resolution and TCM performance (Figure 2). Serial CT scans through this dedicated infant phantom and an adult phantom will be performed and the scan parameters methodically adjusted for each scan. Dose will be estimated using the console CTDI value. The measures of image quality and dose will be compared among the CT scans and the optimized protocol will be selected as the one that offers the lowest dose while maintaining or exceeding the image quality characteristics of the original standard protocol. Figure 2. Two-view diagram shows the specification for the image quality in the infantsized phantom. Each x-y plane image is aligned with the corresponding y-z section beneath it. TCM=tube current modulation. METHODS: Phantom design: We constructed an infant phantom with a plastic housing 110 mm in diameter (similar diameter as the chest of an infant), and it contains material to test four specific aspects of image quality: CT number evaluation, low contrast detectability, spatial resolution, and tube current modulation (TCM) performance (Figure 2). We will use the commercially available adult phantom (Phantomlab Catphan, Gresham, OR). CT scanning: Serial CT imaging of the phantoms will be performed on a 64-slice scanner (GE HD750, General Electric Medical Systems, Milwaukee, WI) with scan parameters adjusted according to Table 2. The parameters in current clinical practice at our institution are located on row 1 of Table 2. The tube potential will remain constant at 80kV, as this setting has shown to be most appropriate for infant scanning.7 CT images will be reconstructed using three separate image reconstruction algorithms (FBP, ASIR, MBIR). Table 2. CT parameters for optimization Tube Current min-max mA Noise index 80-200 12 10-375 14,16,18,20 10-375 12,14,16,18,20 Pitch 0.969 0.969 1.375 14,16,1 Note: First row (italics) is the un-optimized clinical protocol. Tube potential (kV)=80, rotation time=0.5 seconds, prescribed image thickness = 2.5 mm are held constant for all protocols. Phantom Analysis: Data from images acquired from the serial CT scans of the phantom will be analyzed at a clinical radiology workstation (IMPAX v6, Agfa Healthcare, Greenville, SC). Image quality parameters will be measured for each scan and reconstruction type (10 scans x 3 reconstructions = 30 CT datasets of each phantom). CT number and image noise will be measured by taking the mean value and standard deviation of 1 cm2 circular regions of interest (ROI) placed over the background water and over each density insert. Three sets of measurements taken at different slices will be averaged. Low contrast detectability will be assessed by three board certified radiologists (with 3, 6 and 9 years of post-residency experience) by using a 4-alternativeforced-choice test.12 Paired t-tests will be used to assess statistically significant differences in objective image quality parameters among the CT datasets. EXPECTED RESULTS: We will determine thresholds and tradeoffs among CT parameters that impact image quality and exposure to ionizing radiation. The optimized protocol will be defined as one that is comparable to Phelps – Infant CT 3 the current protocol across the different image quality metrics, while offering the lowest dose. We anticipate that MBIR will allow for a substantially lower dose over ASIR and FBP reconstruction algorithms; and the optimized protocol developed with the infant phantom will confer a dose savings over the protocol developed with the adult phantom. POTENTIAL PROBLEMS AND ALTERNATIVES: We assume that the infant phantom will lead to improvements in our current infant CT protocol. It could be that the parameters in Table 2 we have selected may not confer improvements in image quality at equivalent or even reduced doses. If this is the case, we will test smaller incremental variations to the standard infant protocol as well as several other CT parameters such as patient positioning, gantry rotation time and prescribed image thickness that may lend to trade-offs in image quality and reduced exposure to radiation. Also, this is a scanner specific protocol and if we find the phantom confers an advantage we would need to translate this work to other CT models and vendors. Regardless of the outcome, the work will at least validate the current protocol in clinical use and possibly reveal more optimal CT parameters. AIM 2: We will evaluate image quality and patient and organ-specific doses in the clinical application of chest CT imaging optimized for infants. Hypothesis: We hypothesize that the optimized infant chest CT protocol developed in Aim 1 will demonstrate acceptable image quality while offering a lower exposure to ionizing radiation when compared with the current standard clinical protocol. RATIONALE: Although the phantom work outlined in Aim 1 will define an optimized CT protocol for use in infants, it is important to test the clinical feasibility of the optimized protocol and understand the effect the protocol has on image quality and dose reduction. Although CTDI and DLP are the standard dose outputs from diagnostic CT scans, they are widely regarded as inadequate, as they are computed using cylindrical acrylic phantoms and do not account for patient size, shape, or location of the organs in the scanned region.11 We will study subjective and objective assessments of image quality in order to verify the clinical utility with and without the optimized CT protocol. We will also simulate patient-specific and organ-specific doses from scan datasets obtained on these patients using a Monte Carlo-based virtual scanner. Figure 3. Dose efficiency measured on the infant specific phantom is increased with type of image reconstruction: forward back plane (FBP), automatic statistical (ASIR) and model-based iterative reconstruction (MBIR). SD=standard deviation, HU= Hounsfield units. EXPERIMENTAL DESIGN: We will prospectively collect 10 infant chest CT examinations performed with the optimized protocol developed in Aim 1 and retrospectively collect and additional 10 chest CT examinations previously performed with the un-optimized clinical protocol. The studies will be evaluated for objective image noise and subjective image quality. We will implement a virtual scanner to simulate patient specific and organspecific doses. The image quality metrics, overall dose and dose to radiosensitive organs will be compared between un-optimized and optimized CT protocols. METHODS: Patient population: Infant patients (age <1 year-old) who are referred for chest CT to evaluate a clinically necessary medical condition will be eligible for the study. 10 patients will be enrolled consecutively and prospectively and scanned using the optimized protocol determined in Aim 1. By searching the radiology PACS at our institution, we will retrospectively collect chest CT examinations from a separate group of 10 consecutive patients who were <1 year-old and scanned with the un-optimized protocol. CT Protocol: All CT imaging will be performed on the 64-slice scanner described in Aim 1. The optimized CT protocol will be determined in Aim 1. The un-optimized protocol that is currently in use in our institution is described in row 1 of Table 2. Subjective Analysis: Three radiologists (same as in Aim 1) will independently evaluate CT datasets for five categories of image quality: 1) overall image noise, 2) image artifacts, 3) conspicuity of mediastinal structures Phelps – Infant CT 4 4) visibility of small structures and 5) diagnostic acceptability. Categories 1-4 will be rated on a 5-point Likert scale (1=unacceptable, 2=below average, 3=average, and 4=above average, 5=excellent).18-21 The readers will be blinded to the study goals; the patient and scan identifiers will be removed (anonymized) and the order of the 20 studies randomized prior to image review and rating on a PACS workstation (Impax ES version 6, Agfa Technical Imaging Systems, Ridgefield Park, NJ) with clinical grade high-resolution monitors. Objective Analysis: Image noise will be measured by calculating the standard deviation (SD) of HU scale in a 10-15 mm diameter region of interest (ROI) on three tissue types. ROIs will be drawn in the lumen of the aorta at the level of carina, subcutaneous fat of the anterior chest, and the right paraspinal muscle. Dosimeter Measurements: Accurate CTDI-type dose using dosimeter measurements in the CIRS newbornsized tissue equivalent CT phantom will be obtained and compared to the console dose display. This will enable the discrepancy between console dose display and size-specific dose to be accurately measured for this protocol. Differences among the dosimeter measurements and console dose display will be compared using the student t-test. Dose Simulation: The 20 infant CT datasets will be used as input into the virtual scanner (Monte Carlo particle interaction code EGSnrc.22) to simulate patient-specific and organ-specific doses. The actual TCM from each scan will be incorporated using the longitudinal approximated method.23 We will thus be able to evaluate the function of the TCM between patients, both in terms of overall dose and dose to radiosensitive organs. Statistical Analysis: While we anticipate variation, we have performed a power calculation in order to plan the number of patients needed for these experiments. Assuming a difference of 65% in the console CTDIvol between the un-optimized and optimized protocol as indicated by data reported in the literature,18 n=10 patients in each group is sufficient to give a two-tailed alpha =0.05 and a power of 80%. Modified CTDIvol levels, simulated patient doses and image quality ratings from the optimized and unoptimzed protocols will be compared using Wilcoxon signed rank tests. Figure 4. Normalized color-coded dose distribution map produced by a virtual CT scan simulating 18 million photon histories, with data input from a chest CT dataset. The map shows higher dose received by the bones due to their greater attenuation (artifact from metallic brassiere wire also appears red for same reason). EXPECTED RESULTS: We anticipate that the optimized protocol will offer comparable image quality to the standard protocol, while providing ~40% lower radiation exposure to the patient, in accordance with previous findings.18 From the Monte Carlo virtual scans, we expect there to be considerable inter-patient variation in dose. This is due to the large expected range in infant size and habitus affecting the TCM, as well as the differences resulting from changes in the scan length. The inter-patient variation of radiosensitive organ doses is uncertain, as is how this correlates to overall patient dose and image quality. POTENTIAL PROBLEMS AND ALTERNATIVES: If the optimized protocol does not offer images of the same or superior diagnostic interpretability as the standard protocol, Aim 1 will be repeated with less aggressive protocol modification. Calibration of the virtual scanner is not trivial and may be time consuming. We will use SPEKTR,24 a computational toolset designed specifically to facilitate calculation of x-ray spectra, to help ensure beam accuracy over the range required. Further calibration can be achieved through comparison between the physical and simulated doses in the CIRS phantom. TIMELINE OF EVENTS 07/14 – 09/14 Specific Aim 1, Comparison of Infant and Adult Phantoms 10/14 – 03/15 Specific Aim 2, Clinical Assessment 04/15 – 06/16 Data Analysis and Write-up Phelps – Infant CT 5 BIBLIOGRAPHY 1. Siegel MJ, Schmidt B, Bradley D, Suess C, Hildebolt C. Radiation dose and image quality in pediatric CT: effect of technical factors and phantom size and shape. Radiology 2004;233:515-22. 2. Vock P, Stranzinger E, Wolf R. Dose Optimization and Reduction in CT of Children. . Radiation Dose from Multidetector CT, Medical Radiology, Diagnostic Imaging 2012:419-36. 3. Kalra MK, Maher MM, Toth TL, et al. Techniques and Applications of Automatic Tube Current Modulation for CT1. Radiology 2004;233:649-57. 4. Miglioretti DL, Johnson E, Williams A, et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA pediatrics 2013;167:700-7. 5. Pontana F, Duhamel A, Pagniez J, et al. Chest computed tomography using iterative reconstruction vs filtered back projection (Part 2): image quality of low-dose CT examinations in 80 patients. European radiology 2011;21:636-43. 6. Singh S, Kalra MK, Shenoy-Bhangle AS, et al. Radiation dose reduction with hybrid iterative reconstruction for pediatric CT. Radiology 2012;263:537-46. 7. Yu L, Bruesewitz MR, Thomas KB, Fletcher JG, Kofler JM, McCollough CH. Optimal tube potential for radiation dose reduction in pediatric CT: principles, clinical implementations, and pitfalls. Radiographics 2011;31:835-48. 8. Boone JM, Hendee WR, McNitt-Gray MF, Seltzer SE. Radiation exposure from CT scans: how to close our knowledge gaps, monitor and safeguard exposure--proceedings and recommendations of the Radiation Dose Summit, sponsored by NIBIB, February 24-25, 2011. Radiology 2012;265:544-54. 9. Dougeni E, Faulkner K, Panayiotakis G. A review of patient dose and optimisation methods in adult and paediatric CT scanning. European journal of radiology 2012;81:e665-83. 10. Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Archives of internal medicine 2009;169:2078-86. 11. Boone JMS, Keith J.; Cody, Dianna D.; McCollough, Cynthia H.; McNitt-Gray, Michael F.; Toth, Thomas L.; Goske, Marilyn J.; Frush, Donald P. Size-Specific Dose Estimates (SSDE) in Pediatric and Adult Body CT Examinations. Report of AAPM Task Group 204 College Park, MD: American Association of Physicists in Medicine 2011. 12. Mieville FA, Gudinchet F, Brunelle F, Bochud FO, Verdun FR. Iterative reconstruction methods in two different MDCT scanners: physical metrics and 4-alternative forced-choice detectability experiments--a phantom approach. Physica medica : PM : an international journal devoted to the applications of physics to medicine and biology : official journal of the Italian Association of Biomedical Physics 2013;29:99-110. 13. Chen M, Steigner M, Leung S, et al. Simulated 50 % radiation dose reduction in coronary CT angiography using adaptive iterative dose reduction in three-dimensions (AIDR3D). Int J Cardiovasc Imaging 2013;29:1167-75. 14. Koc G, Courtier J, Phelps A, Marcovici PA, MacKenzie JD. Improved CT Depiction of Small Pediatric Vessels with Model-Based Versus Adaptive Statistical Iterative Reconstruction. Pediatric Radiology 2014;in press. 15. Fearon T, Xie H, Cheng JY, Ning H, Zhuge Y, Miller RW. Patient-specific CT dosimetry calculation: a feasibility study. Journal of Applied Clinical Medical Physics 2011;12. 16. Deak P, Straten M, Shrimpton P, Zankl M, Kalender W. Validation of a Monte Carlo tool for patient-specific dose simulations in multi-slice computed tomography. European radiology 2008;18:759-72. 17. Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR American journal of roentgenology 2001;176:289-96. 18. Pickhardt PJ, Lubner MG, Kim DH, et al. Abdominal CT with model-based iterative reconstruction (MBIR): initial results of a prospective trial comparing ultralow-dose with standard-dose imaging. AJR American journal of roentgenology 2012;199:1266-74. 19. Katsura M, Sato J, Akahane M, et al. Comparison of pure and hybrid iterative reconstruction techniques with conventional filtered back projection: image quality assessment in the cervicothoracic region. European journal of radiology 2013;82:356-60. 20. Neroladaki A, Botsikas D, Boudabbous S, Becker CD, Montet X. Computed tomography of the chest with model-based iterative reconstruction using a radiation exposure similar to chest X-ray examination: preliminary observations. European radiology 2013;23:360-6. 21. Singh S, Kalra MK, Moore MA, et al. Dose Reduction and Compliance with Pediatric CT Protocols Adapted Phelps – Infant CT 6 to Patient Size, Clinical Indication, and Number of Prior Studies1. Radiology 2009;252:200-8. 22. Kawrakow I, Rogers D. The EGSnrc code system: Monte Carlo simulation of electron and photon transport. 2000. 23. Khatonabadi M, Zhang D, Mathieu K, et al. A comparison of methods to estimate organ doses in CT when utilizing approximations to the tube current modulation function. Med Phys 2012;39:5212-28. 24. Siewerdsen J, Waese A, Moseley D, Richard S, Jaffray D. Spektr: A computational tool for x-ray spectral analysis and imaging system optimization. Medical physics 2004;31:3057. Phelps – Infant CT 7