postoperative complications

ORIGINAL RESEARCHES
UDC 616.366-002-089.168.1-085.246.2
Use of Enterosgel in complex treatment and prophylaxis of post-operative intraperitoneal in complication of acute cholecystitis
A.A. KARLYICHUK, F.G. KULACHEK, I.S. BILYK, R.I. SYDORCHUK, I.I. BILYK
Department of General Surgery, Bucovinian State Medical Academy
_____________________________________________________________________________________
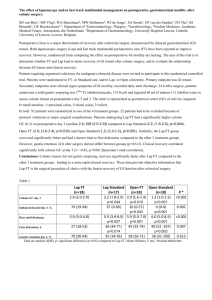
Results of treatment of 106 patients with acute cholecystitis, with the commonly adopted scheme and with the conduction of the colonic sanation and enterosorption in pre- and postoperative periods. It was established that administration of enterosorbent Enterosgel according to our techniques provides more effective complex treatment of acute cholecystitis in postoperative period and prophylaxis of intraperitoneal complications in patients with its destructive forms.
_____________________________________________________________________________________
Introduction. Despite the large number of scientific works dedicated to the diseases of the gall bladder and the bile ducts, there are still a lot of problems, both strategic and connected with the treatment, that still have no final solution. For example, mortality in acute cholecystitis remains high (8-10%) [6, 13,
14]. Intraperitoneal complications in the post-operative period is one of the main reasons of mortality
[6, 10, 11, 12].
It has been found that in the recent years, in spite of the large number of antibacterial medications, there has been no tendency towards rate reduction of purulent inflammation complications. It is mostly caused by antibiotic drug wastage that causes formation of new, antibacterial therapy-resistant microorganisms – “hospital strains” as well as shift of range of the defined hospital-acquired agents, with increase of the role of gram-negative opportunistic flora [5, 7, 8].
Regarding all the above-said it is possible to conclude that antibiotics alone are not enough for prophylaxis of post-operative complications and that it is necessary to find another ways to solve this problem.
Study objectives. To define efficiency of use of Enterosgel in enterosorption and colonic sanation in complex treatment and prophylaxis of intraperitoneal complications in patients with acute cholecystitis in the post-operative period.
Materials and methods. An analysis of 106 patient records has been performed for patients operated due to acute cholecystitis. Patients of the first study group (n=34) in the post-operative period took
Enterosgel in complex therapy p.o. on day 1, 3, 7 and 10 after the operation. Enterosgel was administered at a dose of 15 g diluted in 150 g water 3 times a day. The second study group comprised
55 patients with a destructive form of acute cholecystitis, in which single colonic sanation had been carried out in the process of preoperative preparation according to the developed methodology (Patent of Ukraine No 17922A) as a prophylaxis of intraperitoneal complications. Colonic sanation was repeated on the first day after operation. In the majority of cases, one colonic sanation was enough, however, in case of expressed pathological changes in the abdominal cavity, tissue destruction, repeated surgical
invention (programmed laparotomy, relaparotomy), methodology was used repeatedly. An additional colonic sanation was performed in case of an early bowel obstruction. As a maximum, 6 colonic sanations have been performed in one patient.
In the control group (17 patients), a standard complex treatment was conducted both in preoperative and postoperative periods. All the groups were sufficiently representative by the main anthropometric data, which provided data randomization.
The schedules of anesthetic management, drug infusion therapy and homeostatic correction were the same for all the groups. All the patients were examined using general clinical and laboratory assessments (complete blood count, biochemical blood assay) as well as biochemical studies of bile microflora and peritoneal exudate (in case of its presence).
Study results and their discussion. The large part of the patients was operated within 2 days from their admission. 14 (25.6%) of the patients operated due to destructive forms of acute cholecystitis experienced obstructive jaundice caused by gallstones in the common bile duct. A postoperative clinical examination showed that in the patients of study (main) groups, the temperature was normalized already by day 3 in 80.2%; 61.2 % - in the control group; a postoperative intestinal paralysis was mostly liquidated in the first group in the same ratio – 74.4%, in the group 2 – in 79.3%, in the control group –
52.3; on days 7 and 8 number of leukocytes in the study groups (1 and 2) was (7,66±0,23)x10 9 and -
(7,78±0,26)x10 9 , respectively (on admission - (9,12±0,12) x 10 9 and (11 ± 0,54) x 10 9 ), in control group -
(8,9 ± 0,68) x 10 9 , on admission - (9,1±0,72) x 10 9 ). Before the hospital discharge, the following values were found (see Table 1).
Table 1. Laboratory values before the discharge
Group General bilirubin,
µmol/l
Main (1) 15.4 ±
0.48
(p<0.05)
Main (2) 14.7 ±
0.53
(p<0.05)
Control 18.2 ±
0.76
Creatinine,
µmol/l
84.3 ± 11.2
(p<0.01)
85.72 ±
14.8
(p<0.01)
112.1 ±
18.3
Urea, mmol/l
7.8 ±
0.19
(p<0.05)
7.63 ±
0.51
(p<0.05)
8.31 ±
0.25
General protein, g/l
81.5 ±
5.14
(p<0.5)
84.17 ±
8.94
(p<0.5)
79.78 ±
6.32
Albumin,
%
71.82 ±
3.01
(p<0.05)
59.14 ±
2.11
(p<0.05)
56.71 ±
1.93
Globulin, %
α1, α2
9.8 ±
0/12
(p<0.5)
9.31 ±
0.37
(p<0.5)
10.27
± 0.14
β
9.1 ±
0.04
(p<0.05)
9.2 ±
0.05
(p<0.05)
9.9 ±
0.14
Postoperative complications in the patients of both study groups were observed in 5 patients
(pneumonia – 2, cardiovascular and pulmonary insufficiency – 2, wound abscess – 1).
γ
18.2 ±
0.10
(p<0.05)
18.7 ±
0.37
(p<0.05)
19.3 ±
0.04
In the patients of the control group, postoperative complications were observed in 8 patients
(postoperative pancreatitis – 1, purulent cholangitis – 1, abdominal abscess – 1, wound abscess – 2, pneumonia – 2, cardiovascular insufficiency – 1).
Thus, the data received can be explained by positive influence of enterosorbent and colonic sanation on the biocenosis of the intestinal microflora, which is of expecial importance in the presence of functional
insufficiency [2,10] and reduction of passage of toxic substances from the intestine in the portal circulation and back, reduction of the liver burden [1,3], as well as by the fact that enterosorbent adsorbs mostly substances with molecular weight ranging from 70 to 1000 (urea, bilirubin etc.) almost without absorption of the substances with molecular weight 1000 and more (general proteins, immunoglobulins) [3,4].
Colonic sanation effectivity in correction of intestinal microflora is shown in the Figure 1.
Captions to the figure:
Before colonic sanation - After colonic sanation
Figure 1. Clinical efficiency of a single colonic sanation (concentration change of the main pathogenic agents in the colon lumen).
Conclusions.
1.
Enterosorption provides minimally invasive detoxification effect from various endo- and exogenous substances, with the involvement of natural detoxification functions in the process.
2.
Use of enterosorbent Enterosgel improves general health status of the patients, stimulates subsiding of the general process, induces faster normalization of liver function as well as of other organs and reduces the number of postoperative complications.
3.
The developed method of colonic sanation is an effective prophylaxis of intraperitoneal complications after operative invasions on the bile ducts.
References
1.
Bely V. Ya., Belyaeva O.A. Pathogenic therapy of endotoxicosis in diffuse peritonitis //
Materials of republican research and practical conference “Diagnostics and surgical treatment of diseases and damages of extrhepatic biliary ducts”. Kyiv, 1996. P. 64-65.
2.
Bely V. Ya., Radzichovsky A.P., Belyaeva O.A. Role of GIT paresis in endotoxicosis syndrome in peritonitis // Materials of republican research and practical conference “Actual problems of practical surgery of the organs of abdomen and genitourinary tract”. Kyiv, 1996. P. 100-
102.
3.
Belekov N.A., Solomennikov A.V., Shalachova M.Ya et al. Dynamics of blood biochemical parameters in enterosorption // Human physiology, 1989. – No 1. – P. 143-147.
4.
Vasilyev I.T. Mechanism of endotoxicosis development in acute abscess diseases of abdominal organs. // Surgery, 1995. No 2. P. 54-58.
5.
Veselov A. Ya. Modern ideas on normal digestive tract microflora in adults and on its change within the norm and in some diseases of the digestive organs // Laboratory science.
No 4, 1998, p. 4-11.
6.
Malyugina T.A. Choleperitonitis. Moscow, Medicine, 1973. 256 p.
7.
Sidorchuk I. Yu. Pathogenesis of intestinal disbacteriosis in human patients // Actual nutrition morphogenesis: Materials of science conference. Chernovtsy, 1996. P. 291-292.
8.
Sidorchuk I. Yu. Bacterial translocation and body resistance in acute peritonitis. Synopsis of thesis for a degree of Candidate of medical sciences: 14.00.27. Kyiv, 1997. 24 p.
9.
Skiba V.V., Stadnik V.Ya., Chmel V.E. Enterosorption in treatment of bile ducts obstruction //
Report theses of the conference “New ways and spheres of clinical application of sorption detoxification”. Dnepropetrovsk, 1985. P. 215-216.
10.
Cherpak B.D., Borozdny B.T., Virchenko S.B. Enterosorbul in treatment of postoperative GIT paresis // “New ways and spheres of clinical application of sorption detoxification”.
Dnepropetrovsk, 1985. P. 224-225.