What clinical symptoms reflect postoperative recovery of
advertisement

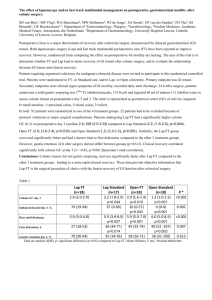
Which clinical symptoms reflect postoperative recovery of gastrointestinal motility? SH van Bree1, LE Nijhuis1, MS Vlug2, WA Bemelman2, WJ de Jonge1, SA Snoek1, EP van der Zanden1, FO The1, MW Hollmann3, RJ Bennink4, GE Boeckxstaens1,5. Department of 1Gastroenterology, 2Surgery, 3Anesthesiology, 4Nuclear Medicine, Academic Medical Center, Amsterdam, the Netherlands. 5Department of Gastroenterology, University Hospital Leuven, Catholic University of Leuven, Leuven, Belgium. Introduction: Impaired gastrointestinal (GI) transit or postoperative ileus (POI) largely determines clinical recovery and duration of hospitalization after abdominal surgery. As colonic motility is the main determinant of clinical recovery, first defecation and flatus are often used as primary outcome parameters in clinical trials. However, whether they actually correlate with GI transit remains unclear. Especially as new potential treatments for POI are emerging, there is a definite need for accurate and reliable outcome variables to objectively evaluate new treatments. Aim: To study the relationship between GI transit and clinical symptoms after GI surgery and to evaluate which symptoms/signs are reliable markers of GI recovery. Methods: Between Oct 2005 and Aug 2009, 85 patients (26-81 y) undergoing segmental colectomy for malignant colorectal disease were included. Clinical symptoms of upper- and lower GI motility were evaluated daily using self-designed questionnaires. 24 h after surgery, patients underwent a solid gastric emptying test (99mTc labelled pancake, 115 Kcal) and ingested 60 ml of indium-111 labelled water to assess colonic transit on postoperative day 2 and 3. The latter was measured by calculating the geometrical center (GC) of activity (segment 0=small intestine; 1=proximal-; 2=distal colon; 3=toilet). A composite score of upper- and lower GI recovery was calculated as time until tolerance of solid food in combination with defecation. Statistical analysis was done using Spearman’s rank correlation. Results: On postoperative day 1, only nausea correlated with gastric retention (r=0.30, p=0.010). Similarly, first flatus (r=-0.27, p=0.022) and first day of tolerance of solid food (r=-0.33, p=0.004) showed a weak correlation with colonic transit on day 3. On the other hand, colonic transit correlated significantly with time until discharge (r= -0.55, p<0.001), time to first defecation (r=-0.46, p<0.001), and the composite score (r=-0.45, p<0.001). 7 patients developed a major complication (i.e. anastomosis leakage and hernia) with paralytic ileus requiring a nasogastric tube on day 3. In these patients indium-111 had not reached the colon at day 3 corresponding to a colonic GC of 0. Conclusions: Paralytic ileus is a distinct type of POI characterized by total inhibition of GI motility. Time until first defecation and time to tolerance of solid food in combination with defecation correlate significantly with colonic GC at day 3 and are the most reliable parameters to indirectly evaluate GI transit. In contrast, time to first flatus is an inaccurate surrogate marker of colonic transit and should not be included in clinical trials.