YELLOW FEVER VACCINE ADVERSE
advertisement

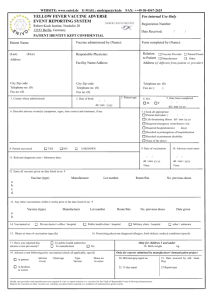
WEBSITE: www.enivd.de E-MAIL: Domingo-CarrascoC@rki.de Phone: ++49 1711605757 For internal Use Only YELLOW FEVER VACCINE ADVERSE EVENT REPORTING SYSTEM Registration Number: Robert Koch Institut, Nordufer 20, 13353 Berlin, Germany Date Received: / / PATIENT IDENTITY KEPT CONFIDENTIAL Vaccine administered by (Name): Patient Name: Form completed by (Name): Relation Vaccine Provider Patient/Parent to Patient Manufacturer Other Address (if different from patient or provider) Responsible Physician: Address: Facility Name/Address City Zip code: Telephone no: (0) Fax no: (0) City Zip code: Telephone no: (0) Fax no: (0) 1. County where administered: 2. Date of birth: Telephone no: (0) Fax no: ( ) / 3. Patient age: / 5. Date form completed 4. Sex M dd / mm / yyyy / F / dd / mm /yy yy 7. Check all appropriate: Patient died (date) 6. Describe adverse events(s) (symptoms, signs, time course) and treatment, if any / / Life threatening illness dd / mm /yy yy Required emergency room/doctor visit Required hospitalization ( days) Resulted in prolongation of hospitalization Resulted in permanent disability None of the above 8. Patient recovered YES NO 9. Date of vaccination UNKNOWN / 11. Relevant diagnostic tests / laboratory data: 10. Adverse event onset / / / dd / mm/ yy yy dd / mm / yyyy Time: Time: _____ 12. Enter all vaccines given on date listed in no. 9 Vaccine (type) Manufacturer Lot number Route/Site No. previous doses a. b. c. d. 13. Any other vaccinations within 4 weeks prior to the date listed in no. 9 Vaccine (type) Manufacturer Lot number Route/Site No. previous doses Date given a. b. Private doctor’s office / hospital 14. Vaccinated at: Public health clinic / hospital Military clinic / hospital other / unknown 15. Illness at time of vaccination (specify) 16. Preexisting physician -diagnosed allergies, birth defects, medical conditions (specify 17. Have you reported this adverse event previously? No To public health authorities To manufacturer Only for children 5 and under 19. Adverse event following prior vaccination (check all applicable, specify in patient in brothers or sisters Adverse Event Onset age Type Vaccine Doses no. In series 18. Birth weight kg Only for reports submitted by manufacturer/ immunization project 20. Mfr.imm.proj.report no 21. Date received by mfr. /imm. Proj. 22. 15 day report 23 Report type Health care providers and manufacturers are required by law to report reactions to vaccines list the Table of Reportable Events Following Immunization. Reports for reactions to other vaccines are voluntary excepted when required as a condition of immunization grant awards.