PEDIATRIC FALLS EDUCATION 1
advertisement

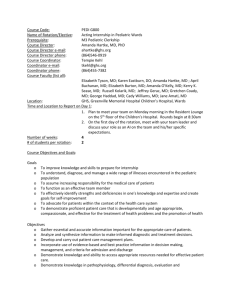
Running head: PEDIATRIC FALLS EDUCATION Educating Nurses on Pediatric Falls Risk Assessment Scales and Falls Prevention Measures Amanda Sikora and Lindsay Snyder The Pennsylvania State University - Capital Campus 1 PEDIATRIC FALLS EDUCATION 2 Abstract Pediatric falls were identified as a current problem on the pediatric acute care unit at Hershey Medical Center. A review of the literature was conducted and information regarding pediatric falls risk assessment and falls prevention interventions was identified. This information was presented to nurses via an educational poster and their knowledge regarding falls information before and after viewing the poster was assessed and recorded. As hypothesized, nurse knowledge of falls risk assessments and interventions improved after viewing the poster. There is a need for further research in pediatric falls to determine the most effective pediatric falls risk assessment scale and prevention interventions. Keywords: falls risk assessment, falls prevention interventions, nurse falls education PEDIATRIC FALLS EDUCATION 3 Educating Nurses on Pediatric Falls Risk Assessment Scales and Falls Prevention Measures Patient safety in the hospital environment is a top priority for healthcare organizations. Patient falls that occur in the hospital have remained both an important and challenging patient safety issue for many of these organizations. In 2005, the Joint Commission created a patient safety goal that focused on reducing the harm caused by inpatient falls. Then, in 2006, the Joint Commission required hospitals to implement falls reduction programs with the goal of reducing the harm resulting from inpatient falls (The Joint Commission, 2007). Additionally, the Magnet accreditation program identifies falls as a nursing sensitive indicator and those organizations seeking Magnet accreditation must meet or exceed national falls benchmarks in order to receive accreditation (Graf, 2011). When magnet status depends on criteria that is without a benchmark, against which it can be measured, as is so in pediatric fall risk assessment, hospitals need to be innovative, establish a bar to set for the industry, and create that standard that allows for growth and guidance (Graf, 2011). Falls in general can contribute to longer hospital stays, comorbidities, irreversible injuries, and a significant amount of money that is not always covered by insurance and thus may force the hospital to foot the bill (Graf, 2011; Schaffer et al., 2012). The goals set forth by the aforementioned organizations as well as the overall desire of organizations to improve safety and reduce patient falls, makes preventing falls an important topic for healthcare organizations today. Much research has been done on inpatient falls and their effects in the adult population (Child Health Corporation of America Nursing Falls Study Task Force, 2009). There are established falls risk scales and falls prevention programs that have been validated and are widely utilized in the adult population (Graf, 2011). The research and recommendations for inpatient falls in the pediatric population, however, are much more limited. Although falls occur PEDIATRIC FALLS EDUCATION 4 at a lower rate in the pediatric population, the rate of injury sustained from falls in the pediatric population is nearly the same as in the adult population (Jamerson et al., 2014). Injuries from falls can lead to an increased length of stay, increased complications and decreased family trust in the healthcare team (Graf, 2011). The impact that these falls have on patient outcomes makes inpatient falls an important topic to examine further in the pediatric population. The purpose of this research project is to assess nurse knowledge of falls risk assessment scales and falls prevention measures on the pediatric acute care floor at Hershey Medical Center. The review of the literature will explore the efficacy of pediatric falls risk assessment scales, the importance of caregiver education in relation to falls prevention, and effective inpatient falls prevention measures. The research project will address the following PICO question: In registered nurses working on the pediatric acute care unit, can a pediatric falls education poster improve nurses’ knowledge of pediatric falls scales and interventions to prevent falls? It is hypothesized that nurses’ knowledge of the aforementioned pediatric falls information will improve after viewing an educational poster. Review of the Literature Fall Risk Assessment Scales According to Hill-Rodriguez et al. (2009), the first step in preventing falls is identifying those who are at a high risk for falling. There is a great deal of research regarding falls in the adult population and there are validated tools that meet the appropriate sensitivity and specificity criteria which can identify those who are at risk for falls in the adult population (Hill-Rodriguez et al., 2009). The literature is much more limited in the pediatric population and there is much debate regarding the best tool to utilize in this unique population (Graf, 2011). Studies suggest that it is important to test screening tools within specific patient populations in order to PEDIATRIC FALLS EDUCATION 5 determine which scale is most appropriate (Graf, 2011; Jamerson et al., 2014). Regardless of the tool chosen to evaluate risk status, performing the evaluation at frequent intervals is important so that high risk patients can be monitored more frequently, falls prevention strategies can be implemented and parents can be educated regarding falls prevention strategies (Graf, 2011). In a study, Ryan-Wenger, Kimchi-Woods, Erbaugh, LaFollette, and Lathrop (2012), discuss the validation of the Pediatric Fall Risk Assessment (PFRA) tool which was developed to evaluate patients at low or high risk for falling. Demographically, there was no difference between control patients, who did not fall, compared to the variable patients who did fall, according to gender or ethnicity/gender. They found sensitivity scores ranging from 47.2% to 85.3% among GRAF-PIF, Humpty Dumpty, and CHAMPS scales, which are three of the most widely used pediatric fall assessment scales in the country. These three scales were compared to the ten item risk factors that make up the PFRA. The sensitivity scores of the three compared assessment tools fall short of the agreed upon standard of 90% or greater sensitivity. While the PFRA scored a 95.1% sensitivity rating, the 60% false-positive and 58.5% false-negative ratings the scale received were deemed unacceptable, giving none of the scales tested accurate enough precision or accuracy to determine fall risk among hospitalized pediatric patients (Ryan-Wegner, Kimchi-Woods, Erbaugh, LaFollette, & Lathrop, 2012). Harvey, Kramlich, Chapman, Parker, and Blades, (2010) researched five pediatric fall assessment instruments in order to compare the assessment tools and their criteria. Again, the study determined more research is required on this topic. The study concluded that two of the five instruments performed well, however, each scale assessed had negative attributes which negated the accuracy of fall risk prediction among pediatric patients. The CNMC and CHAMPS assessment tools revealed no errors yet the CNMC showed to have the least statistical accuracy PEDIATRIC FALLS EDUCATION 6 and the incapability to predict which children were of the highest risk (Harvey et al., 2010). This study found an additional risks, the length of stay and experiencing previous falls during the hospital stay, to contribute to the risk of falls among pediatric patients. Harvey et al. (2010) also determined the risk to be nine times greater of falling in children with temperament/behavior issues. The found blood disorders and cautions about potential bleeding to increase the risk of falls by four as compared to those hospitalized children without hematological identifiers (Harvey et al., 2010). The Humpty Dumpty Fall Scale (HDFS) is a widely used fall assessment scale throughout the country, which was developed at Miami Children’s Hospital. The scale was developed as a response to the need for fall risk assessment among the pediatric population where little to no pediatric specific risk factors had been identified. A Hill-Rodriguez et al. (2009) article based on a 2005-2006 chart review of 308 total patients determined that the HDFS may serve as a valid tool for recognizing pediatric patients who are at high risk for falls. Again, the study reported additional research is needed, but overall found the use of the HDFS on admission, at least once per shift, and upon change of patient level of care to at least bring more awareness to the potential risk of falls among the pediatric population (Hill-Rodriguez et al., 2009). In a direct contradiction of the Hill-Rodriguez et al. (2009) study, a case-control study of pediatric falls reviewing electronic medical records was done in 2013, finding the HDFS to have a sensitivity of 57% and a specificity of 39% (Messmer, P. Williams, & A. Williams, 2013). Messmer, P. Williams, and A. Williams (2013) admit the HDFS captures some of the risks identified with patients in a pediatric setting however, the low sensitivity and specificity of the scale indicate further assessment of the tool and probable adjustments needing to be made. The contradicting views on the HDFS contribute to the confusion and inconsistent nature of the risk PEDIATRIC FALLS EDUCATION 7 factors and assessment criteria the pediatric community so desperately wants to avoid (Messmer, P. Williams, & A. Williams, 2013). Caregiver Presence Studies have found that falls in the pediatric population often occur in the presence of caregivers. In a study conducted at 26 Child Health Corporation of America-member hospitals, 77% of children had an adult present in the room at the time of the fall (Jamerson et al., 2014). Another study found that caregivers were present during the fall 82.8% of the time (Razmus, Wilson, Smith, & Newman, 2006). These findings showcase a unique problem surrounding patient falls in the pediatric population. Since caregivers are present for the majority of falls, it is pertinent to explore what can be done to prevent pediatric inpatient falls in the presence of caregivers. Prevention Measures To date, there are no published pediatric hospital falls prevention programs (Cooper & Nolt, 2007). Several studies, however, have found interventions that have led to a reduction in pediatric falls. One study examined existing fall prevention methods on the pediatric units at the National University Hospital of Singapore. The researchers in this study utilized knowledge of current fall prevention measures and falls data from their electronic health record to determine priority interventions that could be implemented to prevent falls. They determined that reinforcement of fall prevention education for parents and caregivers should be done via physical checks that occur at the change of shift and a falls prevention poster should be placed at the foot of the patient bed (Lee, Yip, Goh, Chiam, & Ng, 2013). They did a pre and post-implementation audit and found that the implementation of the falls prevention strategies reduced overall fall rates from 1.0 falls per 1000 patient days in April-June 2010 to 0.3 falls per 1000 patient days in PEDIATRIC FALLS EDUCATION 8 April-June 2011 (Lee et al., 2013). There was a 100% reduction of falls in children three and younger in the presence of caregivers from April-June 2010 to that in 2011 (Lee et al., 2013). This study highlights the importance of reinforcing falls education and providing additional methods of teaching, like posters, to serve as a reminder of fall prevention strategies for both nurses and caregivers. Another study examined facilities and their varying methods of carrying out falls prevention education. Facilities had a lower fall rate if they used a pamphlet to educate patients and caregiver regarding use of side rails and educated patients and caregivers on more than one occasion regarding fall prevention (Fujita, Fujita & Fujiwara, 2013). The study identified that caregivers can find it difficult to use hospital equipment and thus may have difficulty correctly utilizing side rails, which can increase the child’s risk of falling (Fujita et al., 2013). They also found that it is not adequate to utilize verbal explanation alone to educate parents as facilities that utilized pamphlets and educated parents one more than one occasion during the hospital stay had a significantly lower fall rates (Fujita et al., 2013). Furthermore, a study completed by the Child Health Corporation of America suggests that a falls risk assessment should be completed and patients should be reassessed when assessment findings change and high risk patients should be identified via a physical marker such as a sticker or identification band, should wear non-slip footwear and should receive frequent monitoring (Child Health Corporation of America Nursing Falls Study Task Force, 2009). The researchers suggested that nurses should also offer assistance to those at a high risk for falls, should evaluate medication administration times in order to best reduce the risk of the patient falling, and should educate caregivers on the appropriate use of side rails and proper ambulation techniques (Child Health Corporation of America Nursing Falls Study Task Force, 2009). PEDIATRIC FALLS EDUCATION 9 By assessing patients for their falls risk status at frequent intervals, staff can readily identify patients that are at risk for falls and educate caregivers accordingly. All of the aforementioned studies highlight the importance of utilizing a validated falls risk assessment scale and involving caregivers in falls prevention efforts and education. Utilizing different measures for falls risk identification, such as wrist bands, communicating risk during shift report and providing consistent reinforcement of falls education via posters and verbal explanation, both nurses and caregivers can be part of the solution to reduce the number of falls that occur in the pediatric population. It is of the utmost importance that nurses have a thorough understanding of falls risk assessment scales and falls prevention interventions in order to create a safe environment for patients and ultimately reduce the number of inpatient pediatric falls. Action Plan The idea for this research project was identified by exploring priority topics on the pediatric acute care unit at Hershey Medical Center. One priority topic of interest was that of falls that occur in the inpatient setting in the pediatric population. The pediatric acute care unit experienced seven total falls from the months of January 2015 through October 2015 and, as a result, the unit was actively working to improve nurse knowledge of falls risk assessment and falls prevention interventions. As mentioned in the review of literature, falls prevention is not only an individual hospital goal but falls have been identified by both the Joint Commission and Magnet accreditation program as nursing sensitive indicators (The Joint Commission, 2007; Graf, 2011). All of the aforementioned factors identified falls as a priority topic to address in this research project. PEDIATRIC FALLS EDUCATION 10 Methods It was decided that this project would address the following PICO question: In registered nurses working on the pediatric acute care unit, can a pediatric falls education poster improve nurses’ knowledge of pediatric falls scales and interventions to prevent falls? To begin this project, a falls education poster was created by gathering pertinent falls information from the literature and falls data from the pediatric acute care unit at Hershey Medical Center (Appendix A). The poster focused on general falls information, falls risk assessment scales, falls risk factors, and falls risk identification measures utilized at Hershey Medical Center. From the information included in the educational poster, a falls knowledge assessment questionnaire was created (Appendix B). In the next step of the project, over several weeks on the floor, 18 nurses on the pediatric acute care floor at Hershey Medical Center were given the falls knowledge assessment questionnaire. Nurses included were part-time and full-time floor nurses of the pediatric acute care floor, float nurses that regularly floated to the pediatric acute care floor, and charge nurses or clinical heads from the pediatric acute care floor. The nurses filled out the questionnaire based on their current falls knowledge, the questionnaire was collected and the data was recorded. The same 18 nurses then viewed the falls education poster. After viewing the poster, they were administered the same falls knowledge assessment questionnaire and the data was recorded. Results After the data was collected, the results were compiled and analyzed. The results are shown in Figure 1 (Appendix C) and a graphical analysis is shown in Graph 1 (Appendix D). According to the pre-test results, the nurses on the pediatric acute care floor at Hershey Medical PEDIATRIC FALLS EDUCATION 11 Center were aware of the need for educating parents or caregivers in the room with a child with 100% of them acknowledging the need for caregiver education and what to include and what not to include in the caregiver education. The nurses had a much more difficult identifying all of the items that were actually included in the Humpty Dumpty Fall Scale as 0% of nurses were able to choose all criteria correctly. Another area of weakness included only 33% of the nurses knowing that pediatric falls happen less frequently than adult falls. Although many were unaware of the frequency of pediatric falls, 83% knew that injury occurred just as often in pediatric falls as they do in adult falls. While the results varied among individuals, 83% of the nurses were able to correctly answer how many falls the floor currently had this year, which fall alerts were in place on the floor, and what the best definition of a fall was. After the review of the falls education poster (Appendix A), many of the nurses were able correctly answer more of the questions in the post-test. The nurses on the pediatric acute care floor still had a difficult correctly identifying the criteria included in the HDFS with only 33% answering correctly. Discussion Overall, viewing the educational falls poster improved nurse knowledge regarding unit falls information and prevention measures. The nurses on the pediatric acute care floor, upon assessment of their questionnaire results, seemed to recognize the importance of caregiver education is and what information should be included in caregiver teaching. They had the most difficult time in recognizing the components of the Humpty Dumpty Fall Scale. Although this might seem trivial, it is important for nurses to understand the factors that place children at an increased risk for falls. By understanding the components of the Humpty Dumpty scale, nurses can readily recognize the things that place a child at a high risk of falling and can intervene appropriately. PEDIATRIC FALLS EDUCATION 12 Interestingly, aside from the questionnaire, many of the nurses commented on how helpful an educational falls prevention poster in the room would be due to the lack of retention caregivers have when education about falls is conducted. Their recommendation of supplying a falls prevention poster at the bedside has been studied and documented in the literature and has been found to improve caregiver knowledge of falls prevention and ultimately reduce fall rates (Lee, Yip, Goh, Chiam, & Ng, 2013). Limitations As mentioned in the review of the literature, there is limited data and research regarding pediatric falls (Graf, 2011). In addition, there are no established pediatric falls risk prevention programs (Cooper & Nolt, 2007). In an ideal setting, this research project would have gone beyond just assessment of nurses’ knowledge of pediatric falls risk assessment scales and interventions and would have addressed this gap in the knowledge. An additional limitation, which proved to be quite baffling, was the lack of data on how much hospital costs are impacted by pediatric inpatient falls. With the way hospitals are run today where it seems as though the bottom line is more important than care at times, one would expect extensive data of the financial impact pediatric falls have on an organization. Furthermore, unreported falls, how a fall is defined between organizations, and the way studies are done are all potential limitations related to this topic. In 2007, the NRC defined a fall as a “sudden unexpected descent from a standing, sitting, or horizontal position, including slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), with or without injury to the patient” (Cooper & Nolt, 2007). In 2012 study of a 10-item Pediatric Fall Risk Assessment (PFRA), it was explained how one third of the cases they analyzed had to be dismissed due to the way the PEDIATRIC FALLS EDUCATION 13 falls were categorized. Falls characterized as “accidental” and preventable but not predictable were the falls eliminated from the study. Only those falls that were called intrinsic physical or physiological in origin were considered in that study (Ryan-Wenger et al., 2012). The same article discussed the occurrence of falls that are not reported. While many may want to deny behavior like this occurs in a hospital nurses through the PFRA study admitted that not all falls are reported or even noted in the medical record (Ryan-Wenger et al., 2012). Implications Ideally, if this research project were to be explored further on the pediatric acute care unit at Hershey Medical Center, a required, standardized falls assessment and education protocol would have been implemented unit-wide. To ensure a seamless implementation, a unit chair from night shift and day shift would be selected to assist in leading the implementation process. These two individuals would share in the responsibility of holding staff meetings and disseminating communication in conjunction with management and the education department. Information regarding the new falls assessment and education protocol would be disseminated in this communication and staff members would have the opportunity to discuss any questions or concerns prior to the implementation of the new protocol. Requirements for implementation would include assessment of all patients’ risk for falls upon admission utilizing the Humpty Dumpty Fall Scale. Risk for falls would be reassessed every four hours and documented in the patient’s electronic medical record. All patients, depending on age, and their families would receive standardized education, based on information from the most current literature, regarding falls in the inpatient setting and what they can do to help with falls prevention. All patients at high risk for falls would be required to have documentation of their high risk status in their electronic medical record, would wear a “falls PEDIATRIC FALLS EDUCATION 14 risk” bracelet, would have a falls education poster placed in their room and would have “falls risk” indicated on the sign outside of their doorway. To assess the efficacy of the new falls protocol, weekly chart and patient room audits would be performed. Charts would be checked to ensure that patient’ risk status is evaluated and documented utilizing the Humpty Dumpty Fall Scale according to protocol. Room audits would be done to ensure that patients at a high risk for falls have all of the appropriate risk identification measures as defined in the protocol. Additional evaluation would include monthly analysis of falls data gathered from the MIDAS system. Furthermore, staff surveys would be completed on a monthly basis to assess staff perception of the efficacy of the new falls prevention protocol and would allow for staff to suggest improvements. By rolling out an evidenced-based falls risk assessment and falls prevention protocol, falls rates prior to and post implementation could be analyzed. Once efficacy of the new protocol is confirmed, the protocol could be rolled out on other pediatric units at Hershey Medical Center including the neonatal intensive care unit, continuing care nursery, pediatric intensive care unit, pediatric intermediate care unit and the pediatric hematology/oncology unit. There is clearly a lack of pre and post implementation analyses to show the most effective interventions in reducing pediatric falls rates. Such research could help to bridge the knowledge gap and could eventually lead toward a standardized falls prevention protocol that could be utilized on a national level. Conclusion In conclusion, the importance of addressing pediatric falls is evident. Both the Joint Commission and Magnet accreditation program have recognized the importance of addressing falls and have identified them as nursing sensitive indicators (The Joint Commission 2007; Graf, PEDIATRIC FALLS EDUCATION 15 2011). The requirements of these national organizations as well as the desire to prevent falls and reduce harm to patients showcases the importance of developing protocols to prevent falls in the pediatric population. This research project set out to explore nurses’ knowledge of falls and whether or not a falls education poster could improve nurse knowledge of falls risk assessment scales and falls prevention measures. The results of the research indicated that a falls education poster was effective in improving nurse knowledge of the aforementioned falls information. Nurses were particularly apt at identifying the importance of caregiver falls education and were aware of the falls prevention interventions in place on the unit. They struggled, however, with identifying the components of the Humpty Dumpty Fall Scale. It is pertinent that nurses have a better understanding of the factors that place a patient at a higher risk for falls so that they are able to intervene appropriately. Overall, the implementation of this project was fairly seamless. The issue of falls was a priority issue on the pediatric acute care unit that was readily identified by nurse leaders and preceptors. The review of the literature provided much background information regarding pediatric falls as well as falls risk assessment scales and falls prevention interventions. It was simple to then create and educational poster from the knowledge gained in the review of literature and subsequently create a falls knowledge assessment questionnaire based on the information included in the educational poster. Nurses on the unit were eager to participate in the project which aided in effortless data collection. The results of the implementation were consistent with the hypothesized outcome that nurses’ knowledge of falls would improve after viewing the educational falls poster. PEDIATRIC FALLS EDUCATION 16 This improvement in nurse knowledge with a simple falls education poster is just the beginning to implementing changes that can lead to better patient falls outcomes. The data and research is severely lacking related to the most effective falls risk assessment and falls prevention measures. To further expand on this research project, in an ideal setting, assessing additional nurses to include all that work on the pediatric acute care unit and the knowledge deficit they face would be instrumental. A more extensive literature review could be conducted to assess evidence-based practice that addresses the limitations mentioned above and an evidence-based falls prevention protocol could be implemented on the pediatric acute care unit at Hershey Medical Center. The falls data could be compared before and after the implementation of the new protocol to determine if the measures included in the protocol were effective in reducing the number of falls. If these measures were found to be effective, the protocol could be implemented on other pediatric units and eventually might contribute to creating a standardized, national falls prevention protocol. Creation of such a protocol could ensure that the most up to date, evidence-based measures are being implemented in order to prevent inpatient pediatric falls which can ultimately can lead to better patient outcomes. PEDIATRIC FALLS EDUCATION 17 References Child Health Corporation of America Nursing Falls Study Task Force. (2009), Pediatric falls: State of the science. Pediatric Nursing, 35(4), 227. Cooper, C. L., & Nolt, J. D. (2007). Development of an evidence-based pediatric fall prevention program. Journal of Nursing Care Quality, 22(2), 107-112. Doi:10.1097/01.NCQ.0000263098.83439.8c Fujita, Y., Fujita, M., & Fujiwara, C. (2013). Pediatric falls: Effect of prevention measures and characteristics of pediatric wards. Japan Journal of Nursing Science, 10(2), 223-231. doi:10.1111/jjns.12004 Graf, E. (2011). Magnet Children’s Hospitals: Leading knowledge development and quality standards for inpatient pediatric fall prevention programs. Journal of Pediatric Nursing, 26(2), 122-127, doi:10.0106/j.pedn.2010.12.007 Harvey, K., Kramlich, D., Chapman, J., Parker, J., & Blades, E. (2010). Exploring and evaluating five pediatric falls assessment instruments and injury risk indicators: An ambispective study in a tertiary care setting. Journal of Nursing Management, 18(5), 531. doi: 10.1111/j.1365-2834.2010.01095.x Hill-Rodriguez, D., Messmer, P. R., Williams, P. D., Zeller, R. A., Williams, A. R., Wood, M., & Henry, M. (2009). The humpty dumpty falls scale: A case-control study. Journal for Specialists in Pediatric Nursing : JSPN, 14(1), 22-32. doi:10.1111/j.17446155.2008.00166.x Jamerson, P., Graf, E., Messmer, P., Fields, H., Barton, S., Berger, A.,…Lunbeck, M. (2014). Inpatient Falls in Freestanding Children’s Hospitals. Pediatric Nursing, 40(3), 127-135. PEDIATRIC FALLS EDUCATION 18 Lee, Y. L. G., Yip, W. K., Goh, B. W., Chiam, E. P. J. & Ng, H. P. C. (2013), Fall prevention among children in the presence of caregivers in a paediatric ward: a best practice implementation. International Journal of Evidence-Based Healthcare, 11: 33–38. doi: 10.1111/1744-1609.12003 Messmer, P., Williams, P., & Williams, A. (2013). A case-control study of pediatric falls using electronic medical records. Rehabilitation Nursing, 38(2), 73-79. doi:10.1002/rnj.73 Razmus, I., Wilson, D., Smith, R. & Newman, E. (2006). Falls in hospitalized children. Pediatric Nursing, 32(6), 568-572. Ryan-Wenger, N., Kimchi-Woods, J., Erbaugh, M., LaFollette, L., & Lathrop, J. (2012). Challenges and conundrums in the validation of pediatric fall risk assessment tools. Pediatric Nursing, 38(3), 159-167. Schaffer, P. L., Daraiseh, N. M., Daum, L., Mendez, E., Lin, L., & Huth, M. M. (2012). Pediatric inpatient falls and injuries: A descriptive analysis of risk factors. Journal for Specialists in Pediatric Nursing, 17(1), 10-18. doi: 10.1111/j.1744-6155.2011.00315.x The Joint Commission (2007). Improving America's Hospitals: A Report on Quality and Safety. Retrieved from http://www.jointcommission.org/assets/1/6/2006_Annual_Report.pdf PEDIATRIC FALLS EDUCATION 19 Appendix A PEDIATRIC FALLS EDUCATION 20 Appendix B Pediatric Falls Knowledge Questionnaire Please answer the following questions about pediatric falls using your current knowledge on the subject and what protocol states on 3 Acute Care at HMC Children’s Hospital. 1. True or False: Pediatric falls are less common than adult falls. a. True b. False 2. True or False: Falls in pediatric patients are less likely to result in injury. a. True b. False 3. True or False: Falls education should be provided to parents/caregivers and documented upon patient admission. a. True b. False 4. Which of the following items are included in the Humpty Dumpty Falls Risk Assessment scale? Select all that apply. a. Age b. Gender c. Diagnosis d. Impairments e. Environmental f. Response to Surgery g. Medication Usage h. Caregiver Presence i. History of Falls 5. Which of the following items are currently in use to alert staff that a patient is at risk for falls? Select all that apply. a. Falls risk ID bracelet b. Flag outside of the patient’s room c. Patient wearing different colored gown or socks d. Falls risk poster at the bedside e. Documentation of risk status in the patient’s chart 6. Which of the following should be not be included in caregiver falls education? a. Keep side rails up b. Remain at the bedside at all times c. The wheels of the bed/crib should be locked d. The patient should wear non-slip footwear e. The bed should be in a low position 7. A pediatric nurse knows the best definition of a fall is a. A gradual decline of an individual from any position or height that results in injury to the patient. PEDIATRIC FALLS EDUCATION 21 b. A sudden, unexpected descent from a standing, sitting, or horizontal position, including slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), with or without injury to the patient c. A sudden drop from standing, sitting, or horizontal position, including slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), resulting in injury to the patient. d. A gradual or sudden decline from an unspecified position, location, or height not including a patient slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), with or without injury to the patient. 8. The Children’s Acute Care floor has had how many fall incidents since January 2015? a. 7 b. 3 c. 4 d. 2 PEDIATRIC FALLS EDUCATION 22 Appendix C Table 1: Falls Knowledge Assessment Results Question Correct Answer % Correctly Answered PreAssessment % Correctly Answered Post-Assessment True or False: Pediatric falls are less common than adult falls. True 33% 100% True or False: Falls in pediatric patients are less likely to result in injury. False 83% 100% True or False: Falls education should be provided to parents/caregivers and documented upon patient admission. True 100% 100% Which of the following items are included in the Humpty Dumpty Falls Risk Assessment scale? Select all that apply. A. Age B. Gender C. Diagnosis D. Impairments E. Environmental F. Response to Surgery G. Medication Usage H. Caregiver Presence I. History of Falls A, B, C, D, E, F, G 0% 33% Which of the following items are currently in use to alert staff that a patient is at risk for falls? A. Falls risk ID bracelet B. Flag outside of the patient’s room C. Patient wearing different colored gown or socks D. Falls risk poster at the bedside E. Documentation of risk status in the patient’s chart A, B, E 83% 83% Which of the following should be not be included in caregiver falls education? A. Keep side rails up B 100% 100% PEDIATRIC FALLS EDUCATION B. C. D. E. 23 Remain at the bedside at all times The wheels of the bed/crib should be locked The patient should wear non-slip footwear The bed should be in a low position A pediatric nurse knows the best definition of a fall B is A. A gradual decline of an individual from any position or height that results in injury to the patient. A. A sudden, unexpected descent from a standing, sitting, or horizontal position, including slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), with or without injury to the patient B. A sudden drop from standing, sitting, or horizontal position, including slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), resulting in injury to the patient. C. A gradual or sudden decline from an unspecified position, location, or height not including a patient slipping from a chair to the floor and an assisted fall (where an individual guides the falling individual to the floor), with or without injury to the patient. 83% 83% The Children’s Acute Care floor has had how many fall incidents since January 2015? A. 7 B. 3 C. 4 D. 2 83% 100% A. PEDIATRIC FALLS EDUCATION 24 Appendix D Graph 1: Falls Knowledge Assessment Results Pre-test and Post-test Comparison