full text
advertisement

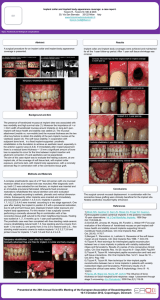
Submission to Journal of Clinical Periodontology: CPE-12-12-4284.R2 TITLE Disparity in embrasure fill and papilla height between tooth- and implant-borne fixed restorations in the anterior maxilla: a cross-sectional study RUNNING TITLE Embrasure fill and papilla height KEY WORDS Dental implant, tooth, fixed partial denture, embrasure, papilla AUTHORS Cosyn, J., Raes, M., Packet, M., Cleymaet, R., De Bruyn, H. AFFILIATIONS AND INSTITUTIONS Jan Cosyn1,2, Magalie Raes1, Mathieu Packet3, Roberto Cleymaet2,3, Hugo De Bruyn1,4 1 University of Ghent, Faculty of Medicine and Health Sciences, Dental School, Department of Periodontology and Oral Implantology, De Pintelaan 185, B-9000 Ghent, Belgium 2 Free University of Brussels (VUB), Faculty of Medicine and Pharmacy, Dental Medicine, Laarbeeklaan 103, B- 1090 Brussels, Belgium 3 Private multidisciplinary practice, Ghent, Belgium 4 Malmö University, Faculty of Odontology, Department of Prosthodontics, 205 06 Malmö, Sweden CONTACT ADDRESS CORRESPONDING AUTHOR Jan Cosyn University of Ghent, Faculty of Medicine and Health Sciences, Dental School, Department of Periodontology and Oral Implantology, De Pintelaan 185, B-9000 Ghent, Belgium E-mail: jan.cosyn@ugent.be 1 WORD COUNT 3003 CONFLICT OF INTERESTS AND SOURCE OF FUNDING The authors declare they have no conflict of interests. The study was supported by the authors and their institutions. ABSTRACT Purpose: The objective of the present study was to compare interproximal fill and papilla height between different embrasures. Material and methods: One hundred and fifty non-smoking consecutive patients (mean age 54, range 32–73; 63 males and 87 females) without periodontal disease were selected in a multidisciplinary practice during regular supportive care. All had been treated for multiple tooth loss in the anterior maxilla at least one year earlier by means of a fixed restoration on teeth (n = 50) or implants (n = 100) using straightforward procedures (without hard and/or soft tissue augmentation). Embrasure fill was assessed by means of Jemt’s papilla index and papilla height was registered following local anesthesia by means of bone sounding by one clinician. Results: Tooth-pontic and tooth-implant embrasures demonstrated comparable interproximal fill and papilla height (≥ 58 % Jemt’s score 3; mean papilla height ≥ 4.1 mm). Between missing teeth, embrasure fill and papilla height were lower regardless of the embrasure type. The implant-implant and implant-pontic embrasure demonstrated comparable outcome (≤ 42 % Jemt’s score 3; mean papilla height ≤ 3.3 mm; p ≥ 0.416), which was significantly poorer when compared to the pontic-pontic embrasure (82 % Jemt’s score 3; mean papilla height 3.7 mm; p ≤ 0.019). Overall, papilla index and papilla height demonstrated a weak correlation (Spearman’s correlation coefficient: 0.198; p = 0.002). Conclusions: The reestablishment of a papilla is difficult when there is no tooth involved. In that scenario a short papilla should be expected and implant-borne restorations demonstrate the poorest outcome. Moreover, an implant with a pontic may not perform better than adjacent implants. 2 CLINICAL RELEVANCE Scientific rationale: The objective of the present study was to compare interproximal fill and papilla height between different embrasures in 150 consecutive patients with fixed restorations on teeth or implants. Principal findings: The reestablishment of a papilla was most difficult between missing teeth. The implantimplant and implant-pontic embrasure demonstrated comparable outcome, which was significantly poorer when compared to the pontic-pontic embrasure. Practical implications: An implant with a pontic may not perform better than adjacent implants in terms of papilla presence. 3 Introduction The aesthetic outcome of a prosthetic treatment is difficult to evaluate as it may be affected by many parameters. In a recent systematic review on the professional assessment of aesthetics in implant dentistry this complexity was highlighted and the need for a consensus on objective and well-defined aesthetic parameters was described (Benic et al. 2012). Albeit there is currently little agreement on such parameters, the presence of papillae may be considered an important characteristic of an aesthetic result. A number of studies have been published on papillae in the context of single implant treatment (Grunder 2000, Choquet et al. 2001, Kan et al. 2003, Henriksson & Jemt 2004, Cardaropoli et al. 2006, Juodzbalys & Wang 2007, Lai et al. 2008, Chen et al. 2009, Cosyn et al. 2011, 2012a, Buser et al. 2011, den Hartog et al. 2008, 2011a,b, Gallucci et al. 2011, Raes et al. 2011). Choquet et al. (2001) described complete papilla index in 58 % of the cases between a tooth and an implant with mean papilla height of nearly 4 mm as assessed by bone sounding. The latter may not differ substantially from papilla height between teeth (Tarnow et al. 1992), which has been explained by the preservation of bone and supracrestal fibers at the tooth facing the implant restoration. Hence, factors causing loss of these tissues such as periodontal disease, multiple surgeries with papilla openings and incorrect implant positioning in relation to the tooth, may in turn be responsible for partial or complete papilla loss (Cosyn et al. 2012c). A recent study has shown that a conventional bridge is still a common treatment concept for single tooth replacement in general practice (Cosyn et al. 2012b). In this concept, the embrasure is formed by a tooth and a pontic. The tissue preserving effect of a tooth may also apply here, which is in line with a ‘predictable papilla length’ of about 5 mm for interproximal tooth surfaces as described by Salama and co-workers (1998). On the other hand, data on papilla index for a tooth-pontic (T-P) embrasure are lacking. Hence, the first objective was to compare papilla index and height between the tooth-implant (T-I) and the T-P embrasure. Complexity increases when two adjacent teeth need replacement in the anterior maxilla. Especially the reestablishment of a papilla between missing teeth is particularly challenging since the interdental bone peak will flatten following tooth loss. Essentially, such an embrasure can be formed by two pontics, two implants or an implant and a pontic. Salama and co-workers (1998) observed a ‘predictable papilla length’ of about 5 mm for interproximal tooth surfaces, 4.5 mm between adjacent implants and 5.5 mm for interproximal implant surfaces not facing another implant. These data suggest the most optimal papilla for an implant-pontic (I-P) and ponticpontic (P-P) embrasure. However, the lack of clear selection criteria and the fact that papilla length was registered by sounding the first tooth- or implant-to-bone contact instead of the interproximal crestal bone peak, 4 make a correct interpretation difficult. Tarnow and co-workers (2003) described mean papilla height of 3.4 mm between implants as assessed by sounding the interproximal crestal bone peak on the basis of a quite heterogeneous sample in terms of implant position (anterior as well as posterior), implant type (one- as well as two-piece implants) and bone conditions (native as well as regenerated bone). To overcome aesthetic failures as a result of a deficient papilla, Tarnow et al. (2003) and Barreto et al. (2008) suggested to place only one implant instead of two and to splint it to a cantilevered ovate pontic. Interestingly however, Tymstra et al. (2011) demonstrated identical embrasure fill for the implant-implant (I-I) and I-P embrasure. Limitations include a very small study sample (5 patients per embrasure type) and lack of data on papilla height. This information clearly shows that the available literature falls short when it comes to data on papillae formed by two pontics, two implants or an implant and a pontic. Hence, another objective was to compare papilla index and height between these embrasures. This information is important from an aesthetic point of view (Tarnow et al. 1992, Jemt 1997) and may become one of the reasons to select or refute a prosthetic treatment option in clinical practice. Material and Methods Patient selection This cross-sectional study was based on a convenience sample of 150 consecutive patients consulting for regular supportive care in a multidisciplinary practice in Ghent between September 2009 and January 2012. Patients were selected on the basis of specific inclusion and exclusion criteria. Inclusion criteria were as follows: - Fixed restoration on teeth (FRT) or implants (FRI) replacing 2 or more adjacent teeth in the anterior maxilla (15-25) and at least 1 year in function. - Prosthetic procedures performed by 1 of 2 restorative dentists (RC/MP). - With respect to FRI, surgical procedures performed by 1 of 2 implant surgeons only using two-piece implant systems (JC/MP). - Informed consent. Exclusion criteria were as follows: - Systemic diseases. - Intake of medication that could induce gingival overgrowth. - Smoking or history of smoking. - Prostheses without ovate pontic design. - History of periodontal treatment. 5 - Periodontal disease at the time of examination. - Hard and/or soft tissue augmentation procedures. - With respect to FRI, suboptimal implant position (T-I distance < 2 mm, I-I distance < 3 mm) as clinically and/or radiographically assessed. - With respect to FRI, peri-implant probing depth > 4 mm and/or bone loss ≥ 2 mm. Measurements between an abutment tooth and adjacent pontic (T-P) and between pontics (P-P) were performed in 50 patients with a FRT (Group I). Measurements between a tooth and an implant (T-I) and between adjacent implants (I-I) were performed in 50 patients with a FRI (Group II). In another 50 patients with a FRI, papillae were studied between an implant and a pontic (I-P) (Group III). All embrasures were evaluated in the anterior maxilla and if the embrasure type of interest was present at multiple locations in a patient, the most central location was selected. The study protocol was approved by the Ethical Committee of the University Hospital in Ghent. Outcome variables The following outcome variables were registered for 250 embrasures with different embrasures in 150 patients by the same experienced and calibrated clinician (JC): - Embrasure fill was assessed by means of Jemt’s papilla index (Jemt 1997). - Papilla height was registered following local anesthesia by means of bone sounding using a periodontal probe (PCPUNC 15, Hu-Friedy®, Leimen, Germany) as described by Tarnow et al. (1992). All recordings were rounded off to the nearest 0.5 mm. Calibration for papilla index was based on 20 duplicate recordings in 4 patients with a time interval of 1 week. Calibration for papilla height was based on a comparison of clinical height to radiographic height of 10 central maxillary papillae in 10 patients. Radiographic papilla height was determined on the basis of digital radiographs taken with the long-cone paralleling technique. Designated software (DBSWIN, Dürr Dental AG, BietigheimBissingen,Germany) was used to calculate radiographic papilla height. Cases used for calibration included all embrasure types. Statistical analysis Data analysis was performed with the patient as the experimental unit. The majority of the data were nonnormally distributed and therefore non-parametric tests were applied. For all continuous variables (age, years in function, papilla height) mean values and standard deviations were calculated, whereas frequency distributions 6 were made for categorical variables (gender, papilla index). Disparities between patient groups in terms of age and years in function were evaluated using the Kruskal-Wallis test. For gender, the Fisher’s exact test was adopted. The Wilcoxon signed ranks test was used to study disparities in papilla index and papilla height between paired data (T-P and P-P within the same patient; T-I and I-I within the same patient). The Fisher’s exact test was adopted to compare unpaired data in terms of papilla index (T-P and T-I in different patients; P-P, I-I and I-P in different patients). Disparities in papilla height between unpaired data were evaluated using the Mann-Whitney test (T-P and T-I in different patients) or Kruskal-Wallis test (P-P, I-I and I-P in different patients). The level of significance was set at 0.05 with no correction for multiple testing. Results The total sample included 150 patients with a mean age of 54 (range 32-73). Sixty-three were males and 87 were females. Restorations had been on average 4 years in function (range 1-10). Table 1 gives an overview of patient’s age, gender and years in function of the restoration per patient group. Patient groups did not differ in any of these aspects (p ≥ 0.091). Sixty-seven patients were rehabilitated using parallel-walled Biomet 3i® (Palm Beach, Florida, USA) implants with an external connection, 22 using tapered Biomet 3i® implants with an internal connection and 11 using Replace Select tapered TiUnite® (Nobel Biocare, Göteborg, Sweden) implants. (HERE APPROXIMATELY TABLE 1 PLEASE) Embrasure fill Duplicate registration of papilla index resulted in high intra-examiner agreement (Spearman’s correlation coefficient: 0.915; p ≤ 0.001). Table 2 shows frequency distributions on papilla index sorted per embrasure type. T-P and P-P embrasures assessed in the FRT group, did not differ significantly in papilla index (p = 0.439). In the FRI group with adjacent implants however, significantly less interproximal fill was observed for I-I when compared to T-I embrasures (p < 0.001). Comparison of unpaired data in different patient groups revealed comparable papilla index for T-P and T-I embrasures (p = 0.185). Particularly interesting from an aesthetic point of view was the evaluation of papilla index between missing teeth with P-P, I-I or I-P embrasures as possible solutions. Significantly more interproximal fill was observed for the P-P embrasure when compared to I-I (p < 0.001) and I-P (p < 0.001). I-I and I-P embrasures demonstrated comparable papilla index (p = 0.416). As also shown in 7 table 2, complete interproximal fill was only accomplished in less than half of the cases when one or two implants formed the embrasure. A clinical example of an I-P embrasure is shown in figure 1. (HERE APPROXIMATELY TABLE 2 & FIGURE 1 PLEASE) Papilla height Clinical and radiographic papilla height demonstrated high agreement (Spearman’s correlation coefficient: 0.994; p ≤ 0.001). Based on the total patient sample papilla height and years in function demonstrated a significant, yet weak correlation (Spearman’s correlation coefficient: 0.178; p = 0.029). Table 3 shows the results on papilla height sorted per embrasure type. T-P and P-P embrasures as assessed in the FRT group, differed significantly in papilla height with papillae being on average 0.5 mm shorter between pontics (p = 0.001). In the FRI group with adjacent implants, papillae were on average 0.8 mm shorter for I-I when compared to T-I embrasures (p < 0.001). Comparison of unpaired data in different patient groups revealed comparable papilla height for T-P and T-I embrasures (p = 0.383). When scrutinizing possible solutions for recreating papillae between missing teeth, papillae were on average 0.4 – 0.5 mm higher for the P-P embrasure when compared to I-I (p = 0.019) and I-P (p = 0.004). I-I and I-P embrasures demonstrated comparable papilla height (p = 0.486). As also shown in table 3, the probability of ending up with an ideal papilla (≥ 4 mm) between missing teeth was reduced by half when one or two implants formed the embrasure. (HERE APPROXIMATELY TABLE 3 PLEASE) Correlation of papilla index with papilla height On the basis of the total sample (n = 250) papilla index and papilla height demonstrated a weak, yet significant correlation (Spearman’s correlation coefficient: 0.198; p = 0.002). Discussion The amount of soft tissues filling the embrasure may be affected by ample factors. These have been identified in a study on single implant treatment using multivariate analyses and include periodontal disease, multiple surgeries with papilla openings and factors relating to the implant and contact point position (Cosyn et al. 2012c). In the present study patient selection was very strict taking into account most of these factors. Albeit this stringent intake took many years, it ensured a quite homogeneous study sample allowing for comparisons of 8 multiple embrasures in different patient groups. Salama and co-workers (1998) were the first to document ‘predictable papilla length’ for different embrasures. However, their findings are difficult to interpret given the lack of clear selection criteria and the fact that papilla length was registered by sounding the first tooth- or implant-to-bone contact instead of the interproximal crestal bone peak. Clearly, accurate data on papillae for different embrasures are needed as these may be important from an aesthetic point of view. A key finding was that the T-I and T-P embrasure demonstrated similar papilla index (≥ 58 % with complete fill) and papilla height (≥ 4.1 mm on average). These data do not differ substantially from those between teeth (Tarnow et al. 1992), suggesting a tissue preserving effect of the tooth. On the other hand, when the embrasure was not formed by a tooth significantly less embrasure fill and/or papilla height were found. This situation occurs when adjacent teeth are missing and need replacement. The most favourable outcome was found when such an embrasure was formed by two pontics (82 % with complete fill and 3.7 mm mean papilla height). Whenever one or two implants formed such an embrasure, significantly less embrasure fill (≤ 42 % with complete fill) and papilla height (≤ 3.3 mm on average) were demonstrated. Tarnow et al. (2003) described mean papilla height of 3.4 mm between implants, which is very similar to our observation (3.3 mm on average). Interestingly, the I-P embrasure did not perform better than the I-I embrasure in contrast to previous beliefs (Tarnow et al. 2003, Barreto et al. 2008), which is in agreement with a recent pilot study (Tymstra et al. 2011). This information is clinically relevant when it comes to replacing two missing adjacent teeth in the anterior maxilla. The installation of only one implant with a cantilevered pontic is less expensive than two implants, but may not result in superior aesthetics as shown in this study. Moreover, clinicians should be aware of the fact that there are only limited data on implant success and complications for a cantilever bridge on only one implant (Aglietta et al. 2009, 2012, Tymstra et al. 2011). By and large, about 1 mm shorter papillae were demonstrated between implants or between an implant and a pontic when compared to embrasures formed by one or two teeth. Possibly this is related to a lack of inserting supracrestal fibers around implants (Berglundh et al. 1991). In addition, one may also expect significant loss in the vertical dimension in such embrasures since the bone peak will flatten following tooth extraction. The papillary asymmetry may therefore even become 2 mm as described by Kourkouta et al. (2009), which is detrimental from an aesthetic point of view when a central and lateral incisor or a lateral incisor and a cuspid on one side need replacement. Ridge preservation, orthodontic extrusion, bone augmentation, distraction osteogenesis and root submergence have been proposed as treatment options (Zetu & Wang 2005, Salama et al. 2007). Given the technical complexity of these concepts and their single focus on bone foundation, it is clear that 9 implant dentistry has no straightforward solution for this problem and a FRT with a P-P embrasure may be considered the best option from an aesthetic point of view to treat this. On the other hand, the range on papilla height for a P-P embrasure was very high in this study and one could question whether it is ethical to remove sound tooth structure in order to install a FRT. Future studies should therefore focus on papilla reconstruction between implants or between an implant and a pontic using connective tissue grafting. Since it is also unclear whether further improvement in the papilla formed by two pontics is possible using connective tissue grafting, prospective studies should also focus on FRT. In this study the papilla index by Jemt (1997) was used to study embrasure fill. As this index was initially designed for single tooth implants with adjacent teeth, it may not really hold up when there is no tooth forming the embrasure, i.e. between pontics, beween adjacent implants or between an implant and a pontic. In these situations, the two adjacent crowns can be made to any shape to close down the embrasure space resulting in a high papilla index score whereas papilla height may remain low. This phenomenon may explain why the P-P embrasure demonstrated complete fill in 82 % of the cases, whereas mean papilla height was only 3.7 mm. Hence, it is not surprising that papilla index and papilla height only demonstrated a weak correlation. Clearly, the results on papilla height may be considered crucial in this study and papilla index data should be interpreted with caution as these may be prone to bias. A second limitation of this study relates to the fact that T-T embrasures were not included. On the other hand, it was our objective to study embrasures in the context of different treatment options for tooth loss and these do not include T-T embrasures. Another concern of this study relates to the bone sounding technique and the associated risk of soft tissue damage. Because of this, imaging techniques may be preferred in future studies. However, an important limitation of these methods is a lack of visibility of the tip of the papilla due to overlap of teeth. This is especially the case in the canine and premolar region and was the very reason why we only included digital radiographs of the central papilla to evaluate accuracy of clinical registrations. A final concern of this study relates to the external validity of the results. An attempt was made to select a homogeneous sample in terms of clinicians, periodontal and peri-implant conditions, implant types and positions, and pontic design. However, more factors may affect the presence of a papilla (Chang 2007, Chow et al. 2010), and the impact of socio-economic and geographic aspects remains to be investigated. In conclusion, this clinical study showed that the reestablishment of a papilla is difficult when there is no tooth involved. In that scenario a short papilla should be expected and implant-borne restorations demonstrate the poorest outcome. Moreover, an implant with a pontic may not perform better than adjacent implants. 10 Acknowledgements The authors wish to thank all participants for their contribution. References Aglietta, M., Iorio Siciliano, V., Blasi, A., Sculean, A., Brägger, U., Lang, N.P., Salvi, G.E. (2012) Clinical and radiographic changes at implants supporting single-unit crowns (SCs) and fixed dental prostheses (FDPs) with one cantilever extension. A retrospective study. Clinical Oral Implants Research 23, 550-555. Aglietta M, Siciliano VI, Zwahlen M, Brägger U, Pjetursson BE, Lang NP, Salvi GE. (2009) A systematic review of the survival and complication rates of implant supported fixed dental prostheses with cantilever extensions after an observation period of at least 5 years. Clinical Oral Implants Research 20, 441-51. Barreto, M., Francischone, C.E., Filho, H.N. (2008) Two prosthetic crowns supported by a single implant: an esthetic alternative for restoring the anterior maxilla. Quintessence International 39, 717-725. Benic, G.I., Wolleb, K., Sancho-Puchades, M., Hämmerle, C.H.F. (2012) Systematic review of parameters and methods for the professional assessment of esthetics in dental implant research. Journal of Clinical Periodontology 39 (Suppl. 12), 160–192. Berglundh, T., Lindhe, J., Ericsson, I., Marinello, C.P., Liljenberg, B., Thomsen, P. (1991) The soft tissue barrier at implants and teeth. Clinical Oral Implants Research 2, 81-90. Buser, D., Wittneben, J., Bornstein, M.M., Grütter, L., Chappuis, V., Belser, U.C. (2011) Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. Journal of Periodontology 82, 342-349. Cardaropoli, G., Lekholm, U., Wennström, J.L. (2006) Tissue alterations at implant-supported single-tooth replacements: a 1-year prospective clinical study. Clinical Oral Implants Research 17, 165-171. Chang, L.C. (2007) The association between embrasure morphology and central papilla recession. Journal of Clinical Periodontology 34, 432-436. Chen, S.T., Darby, I.B., Reynolds, E.C., Clement, J.G. (2009) Immediate implant placement postextraction without flap elevation. Journal of Periodontology 80, 163-172. 11 Choquet, V., Hermans, M., Adriaenssens, P., Daelemans, P., Tarnow, D.P., Malevez, C. (2001) Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. Journal of Periodontology 72, 1364-1371. Chow, Y.C., Eber, R.M., Tsao, Y.P., Shotwell, J.L., Wang, H.L. (2010) Factors associated with the appearance of gingival papillae. Journal of Clinical Periodontology 37, 719-727. Cosyn, J., De Bruyn, H., Cleymaet, R. (2012a) Soft tissue preservation and pink aesthetics around single immediate implant restorations: a 1-year prospective study. Clinical Implant Dentistry and Related Research [Epub ahead of print]. Cosyn, J., Eghbali, A., De Bruyn, H., Collys, K., Cleymaet, R., De Rouck, T. (2011) Immediate single-tooth implants in the anterior maxilla: a 3-year case cohort study on hard and soft tissue response and aesthetics. Journal of Clinical Periodontology 38, 746-753. Cosyn, J., Raes, S., De Meyer, S., Raes, F., Buyl, R., Coomans, D., De Bruyn, H. (2012b) An analysis of the decision-making process for single implant treatment in general practice. Journal of Clinical Periodontology 39, 166-172. Cosyn, J., Sabzevar, M.M., De Bruyn, H. (2012c) Predictors of inter-proximal and midfacial recession following single implant treatment in the anterior maxilla: a multivariate analysis. Journal of Clinical Periodontology 39, 895-903. den Hartog, L., Raghoebar, G.M., Slater, J.J., Stellingsma, K., Vissink, A., Meijer, H.J. (2011a) Single-tooth implants with different neck designs: a randomized clinical trial evaluating the aesthetic outcome. Clinical Implant Dentistry and Related Research [Epub ahead of print]. den Hartog, L., Raghoebar, G.M., Stellingsma, K., Vissink, A., Meijer, H.J. (2011b) Immediate non-occlusal loading of single implants in the aesthetic zone: a randomized clinical trial. Journal of Clinical Periodontology 38, 186-194. den Hartog, L., Slater, J.J., Vissink, A., Meijer, H.J., Raghoebar, G.M. (2008) Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: a systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. Journal of Clinical Periodontology 35, 1073-1086. Gallucci, G.O., Grütter, L., Chuang, S.K., Belser, U.C. (2011) Dimensional changes of peri-implant soft tissue over 2 years with single-implant crowns in the anterior maxilla. Journal of Clinical Periodontology 38, 293-299. 12 Grunder, U. (2000) Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. International Journal of Periodontics and Restorative Dentistry 20, 11-17. Henriksson, K., Jemt, T. (2004) Measurements of soft tissue volume in association with single-implant restorations: a 1-year comparative study after abutment connection surgery. Clinical Implant Dentistry and Related Research 6, 181-189. Jemt, T. (1997) Regeneration of gingival papillae after single-implant treatment. International Journal of Periodontics and Restorative Dentistry 17, 326-333. Juodzbalys, G., Wang, H.L. (2007) Soft and hard tissue assessment of immediate implant placement: a case series. Clinical Oral Implants Research 18, 237-243. Kan, J.Y., Rungcharassaeng, K., Umezu, K., Kois, J.C. (2003) Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. Journal of Periodontology 74, 557-562. Kourkouta, S., Dedi, K.D., Paquette, D.W., Mol, A. (2009) Interproximal tissue dimensions in relation to adjacent implants in the anterior maxilla: clinical observations and patient aesthetic evaluation. Clinical Oral Implants Research 20, 1375-1385. Lai, H.C., Zhang, Z.Y., Wang, F., Zhuang, L.F., Liu, X., Pu, Y.P. (2008) Evaluation of soft-tissue alteration around implant-supported single-tooth restoration in the anterior maxilla: the pink esthetic score. Clinical Oral Implants Research 19, 560-564. Raes, F., Cosyn, J., Crommelinck, E., Coessens, P., De Bruyn, H. (2011) Immediate and conventional single implant treatment in het anterior maxilla: one-year results of a case series on hard and soft tissue response and aesthetics. Journal of Clinical Periodontology 38, 385-394. Salama, M., Ishikawa, T., Salama, H., Funato, A., Garber, D. (2007) Advantages of the root submergence technique for pontic site development in esthetic implant therapy. International Journal of Periodontics and Restorative Dentistry 27, 521-527. Salama, H., Salama M.A., Garber, D., Adar, P. (1998) The interproximal height of bone: a guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Practical Periodontics and Aesthetic Dentistry 10, 1131-1141 13 Tarnow, D., Elian, N., Fletcher, P., Froum, S., Magner, A., Cho, S.C., Salama, M., Salama, H., Garber, D.A. (2003) Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. Journal of Periodontology 74, 1785-1788. Tarnow, D.P., Magner, A.W., Fletcher, P. (1992) The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. Journal of Periodontology 63, 995-996. Tymstra, N., Raghoebar, G.M., Vissink, A., Meijer, H.J. (2011) Dental implant treatment for two adjacent missing teeth in the maxillary aesthetic zone: a comparative pilot study and test of principle. Clinical Oral Implants Research 22, 207-213. Zetu, L., Wang, H.L. (2005) Management of inter-dental/inter-implant papilla. Journal of Clinical Periodontology 32, 831-839. 14