About the Vincent Foundation
advertisement

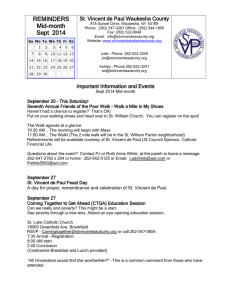
VINCENT FOUNDATION Case #1 Expert Panel Case Evaluation Hypoxic-ischemic brain injury occurring at age 5 years in a male child with underlying mild autism spectrum disorder Draft dated 14 November 2014 (JYS) CONTENTS About the Vincent Foundation .................................................................................................. 3 About the Expert Panel................................................................................................................ 4 Section 1 1.1 Clinical History ...................................................................................................................... 7 1.1.1 Summary Statement ............................................................................................. 7 1.1.2 Medical and Surgical History ............................................................................... 7 1.1.3 Birth History ........................................................................................................... 11 1.1.4 Family History ....................................................................................................... 12 Section 2 2.1 2.2 Clinical Data and Analyses Supplemental Information and Appendices Radiological Assessments ................................................................................................. 17 2.1.1 CT Scan Reports .................................................................................................. 17 2.1.2 MRI Scan Reports ................................................................................................ 17 2.1.3 PET Scan Reports ................................................................................................. 17 Metabolic and Neurometabolic Testing ........................................................................ 18 2.2.1 EEG Report 20.06.2012........................................................................................ 18 2.2.2 EEG Reports (21.6.2012, 22.6.2012, 23.6.2012, 19.7.12) ................................... 18 2.3 Medications and Timelines ............................................................................................... 21 2.4 Genetic Analyses............................................................................................................... 22 2.4.1 Amniocentesis - karyotype ................................................................................ 22 2.4.2 Amniocentesis - FISH ........................................................................................... 23 2.4.3 Microarray and Sequencing ............................................................................. 23 2.5 Physical Growth ................................................................................................................. 24 2.6 Neurology and Neuromuscular Evaluations .................................................................. 26 2.6.1 Neurological Status as of 30.08.2012 ................................................................ 26 2.6.2 Neurological Status as of 13.09.2012 ................................................................ 27 Vincent Foundation Clinical Case Compendium: Case 1 Page 1 of 38 2.6.3 Physical and Occupational Therapy Status as of 12.9.2012 ......................... 29 2.6.4 Speech and Language Evaluation as of 2.1.2013 ......................................... 34 Section 3 Evaluations and Guideline Recommendations .............................................. 36 3.1 Pharmacological Interventions ....................................................................................... 36 3.2 Nutrition and Nutritional Supplements ............................................................................ 37 3.3 Rehabilitation Interventions and Strategies ................................................................... 38 3.4 3.5 3.3.1 Physical Therapy.................................................................................................. 38 3.3.2 Occupational Therapy....................................................................................... 38 3.3.3 Speech and Language Therapies.................................................................... 38 3.3.4 Education ............................................................................................................. 38 Complimentary and Alternative Medicine Treatments ............................................... 38 3.4.1 Acupuncture ....................................................................................................... 38 3.4.2 Eastern Herbal treatment................................................................................... 38 Additional Interventions of Interest ................................................................................. 38 3.5.1 Intrathecal Baclofen........................................................................................... 38 3.5.2 Deep Brain Stimulation ....................................................................................... 38 3.5.3 Botulinum Toxin .................................................................................................... 38 Vincent Foundation Clinical Case Compendium: Case 1 Page 2 of 38 ABOUT THE VINCENT FOUNDATION The Vincent Foundation (www.vincentfoundation.org) is a non-profit organization whose primary mission is to promote translational research and novel treatments for children with brain injury. The Foundation’s multidisciplinary expert panel conducts in-depth clinical case evaluations of prevalent types of childhood brain injuries. These in-depth case studies serve as the basis for expert opinions about integrated and/or leading edge treatment interventions. The opinions are integrated into problem-based “personalized” reports that can provide clinical practitioners around the globe access to world-class medical opinions about optimizing treatment for these children. Patients seeking Foundation services must agree to provide detailed clinical data. The records will be de-identified before submission to our Expert Panel for a comprehensive review that results in a Foundation Expert Clinical Report. To be accepted for evaluation, the Foundation must be provided with complete medical records, including clinical notes and consultant reports, test results, details of prior treatments, copies of all radiological images, and have had a recent status re-evaluation by their clinical care team. In addition to the value of the Foundation’s Expert Clinical Report as an instructional tool, the document can provide patients with a more intensive, personalized assessment of clinical management than they would otherwise receive in a standard clinical setting, particularly in medical resource-poor regions. Vincent Foundation Clinical Case Compendium: Case 1 Page 3 of 38 ABOUT THE EXPERT PANEL Dr Ralf Clauss Dr Ralf Clauss is a Consultant Physician in Nuclear Medicine at the Royal Surrey County Hospital, UK. He completed his MBChB at the University of Pretoria and his MMed in Nuclear Medicine at the Medical University of Southern Africa. He completed his MD at the University of Düsseldorf in Germany and is a fellow of the Royal College of Physicians in London. In 1999, together with Dr Wally Nel, he described a patient in the Vegetative State who regained consciousness on the medication Zolpidem, the first ever patient in the world to do so. Dr Clauss completed a 99mTc HMPAO SPECT brain scan on this patient and discovered the effect of Zolpidem on cerebral perfusion after brain damage. Together with Dr Nel and other colleagues, he continues to research the effect of Zolpidem on brain damage and also the role of neurotransmitter homeostasis after brain damage particularly that of oxygen based amino acids such glutamate and GABA, and monoamines such as dopamine, noradrenaline and serotonin. [Dr X X] [Dr X X] [Dr X X] Medical editor: Dr. Glenn H. Bock Dr. Bock’s medical career has spanned more than 30 years. In addition to his medical practice, his professional activities included university hospital teaching positions, having served as Director of both Paediatric residency and Paediatric Nephrology fellowship programs at the Inova Fairfax Hospital for Children and Children’s Hospital National Medical Center, respectively. He also was a clinical and laboratory investigator throughout his career, and has published or presented nearly 100 peer-reviewed papers and textbook contributions. He has written or edited many medical manuscripts, research proposals, and public medical education media. Dr. Bock has recently retired Vincent Foundation Clinical Case Compendium: Case 1 Page 4 of 38 from clinical medicine. With a very broad knowledge base and a passion for life-long learning, he is now devoting his time to editing and writing on numerous medical topics. Dr. Bock received his medical degree from the University of Missouri – Columbia in 1975. He then served as a Paediatric resident at the State University of New York – Upstate Medical University, and completed a clinical and research fellowship in Paediatric Nephrology at the University of Minnesota Hospitals in Minneapolis. Vincent Foundation Clinical Case Compendium: Case 1 Page 5 of 38 SECTION 1: CASE 1 Clinical Data and Analyses CLINICAL DATA AND ANALYSES 1.1 CLINICAL HISTORY 1.1.1 Summary Statement This is a case of severe hypoxic-ischemic brain injury occurring at age 5 years in a male child with underlying mild autism spectrum disorder. The injury occurred in the immediate postoperative period following administration of several doses of ketamine and subsequent cardiopulmonary arrest. The total duration of the episode, from initial recognition to successful resuscitation, was 10 to 15 minutes. Thereafter he had severe dystonia/spasticity with radiographic confirmation of permanent cerebral hypoxic-ischemic injury. His global physical disabilities and inability to communicate verbally have made the evaluation of residual cognitive function and realistic expectations of cognitive potential difficult. 1.1.2 Medical and Surgical History This male child is currently 7 years old (DOB 15 June 2007). His diagnoses include congenital cleft lip and palate, developmental delay whose evaluation at age 4 years suggested mild autism spectrum disorder, and chronic severe ischemic brain injury following elective cosmetic nose surgery at age 5 years. Cleft Lip and Palate An uncomplicated amniocentesis was done at approximately 20 weeks gestation prompted by findings on fetal ultrasonography that suggested an orofacial abnormality. Karyotype was 46 XY, and no chromosomal abnormalities were identified. FISH showed normal copy numbers for chromosomes 13, 18, and 21 with a threshold of detection of mosaicism of 20% and a test sensitivity of 95%. He successfully underwent an initial cleft lip repair in the neonatal period. A partial cleft palate repair was done at age 3 years, and the subsequent cosmetic revision at age 5 years. His medical records do not suggest any chronic infectious illnesses associated with his cleft palate. Neurodevelopmental Delay Early gross motor development was normal; crawled at age 6-9 months, walked at 1 year. His first words were at 2.0 years. At age 3 years and 10 months he Vincent Foundation Clinical Case Compendium: Case 1 Page 7 of 38 underwent developmental assessment due to parent and teacher concerns about poor social skills and peer interactions, and observed speech and language difficulties. The Early Autism Project subsequently evaluated him at age 4 years and 5 months. The findings from these evaluations included: both expressive and receptive language delays with no structural oropharyngeal abnormalities, articulation difficult to understand, inconsistent eye contact, avoidance of peer interactions with a tendency to play by himself, short attention span and easily distractibility, use of nonverbal communication strategies He also was noted to enjoy music, could count and knew his alphabet, and understood familiar commands at home (with assistance of situational understanding and visual clues). The evaluations concluded that he had characteristics of mild autism, scoring 27 on the Childhood Autism Rating Scale (range for “minimal symptoms of autism” 15 - 29.5). Treatment recommendations from these evaluations included: Placing emphasis on the use of one language at home (multi-lingual family). The family followed through using English as primary language. Enhancing language development skills through exposure to children of his own language age, require use of language instead of acquiescing to nonverbal communication, implementing PECS (Picture Exchange Communication System) in school, Speech therapy Intensified behavioural therapy Assistance from a full-time shadow for socialization, limit setting, and assimilation He has not yet undergone a systematic re-evaluation of interventions and the domains of developmental progress. Vincent Foundation Clinical Case Compendium: Case 1 Page 8 of 38 Acute Hypoxic-Ischemic Brain Injury On 20 June 2012 (age 5 years), the child was admitted to the hospital for cosmetic nose revision and repair of extensive dental caries under general (inhaled) anaesthesia. There was no pre-medication, nor notation of problems with induction or intubation. No intraoperative problems or events are noted. In the recovery room he was agitated and 5 mg ketamine was administered IV by the anaesthesiologist. The solution was prepared as a 1:10 dilution of 1 mL ketamine (50 mg/mL) in a 10 mL syringe. A short time later in the recovery room the child was described as groggy, “making noise”, and touching his surgical dressing. A recovery room nurse administered an additional ketamine dose from the same syringe for “pain and agitation”. Although the narrative records state that the dose was an additional 5 mg, the amount given was not clearly documented. Very soon thereafter, the child’s father noted shallow breathing followed by cyanosis. He alerted the nursing staff and a code blue was called. The child appeared to have had a full cardiopulmonary arrest with an estimated duration of 10 to 15 minutes until successful resuscitation. He remained intubated and ventilated and BP was in acceptable range. Several hours’ later, vital signs were still in acceptable ranges, pupils were stated to be 2 mm but reactive, although no spontaneous movement was seen and the Glasgow Coma (GCS) scale was 3/15. He received several daily doses of intravenous dexamethasone, 4 mg, and mannitol 75 mL over 1 hour. His initial magnetic resonance imaging study, including an MRV, was done about 5 hours following his hypoxic event and was essentially normal (see Section 2.1.2. for sequential MR findings). Initial and serial laboratory studies are listed in Section 2.2.3. None of the initial test results obtained was sufficiently abnormal to explain the arrest. Additional studies done during this hospitalization included evaluation for possible Velo-Cardio-Facial Syndrome; ECG and echocardiogram were normal, and genetic testing by whole genome exome sequencing and microarray analyses were not consistent with the diagnosis (see full summary of findings in Section 2.4.). Plasma amino and organic acid analyses were normal as were serum lactate and pyruvate and, later, blood ammonia. The sequences of clinical events and findings during the hospitalization, lasting approximately 3 months (discharged 22 September 2012), are described below, and in Sections 2.2.3.(serial laboratory results) and 2.3. (medications). Stable VS with GCS remaining 3/5 for first 2 days, followed by improvement to 7/15 by day 2 to 3. Probable seizures early in course, received barbiturates. Vincent Foundation Clinical Case Compendium: Case 1 Page 9 of 38 EEG initially showed diffuse slow waveform cerebral rhythms that are noted to have improved over subsequent days although “slowing” persisted with diminished alpha component on repetitive studies. On day 10, GCS still noted to be 7/15. By day 22 the GCS was 11/15. Slow improvement of spontaneous activity, eye opening, not cognitively interactive for first 2 weeks. During that time, developed significant dystonia and spasticity. Slowly improving environmental and family/staff interactivity, smiling responsively by approximately week 4. Hospital interventions included intensive PT, OT, and speech therapy. Upper gastrointestinal dysfunction resulted in nasogastric tube feeding dependency in the hospital. Medications during latter part of hospitalization included baclofen 7.5 mg QID, artane 2 mg QID, Valium (changing/tapering doses), and lanzoprazole 15 mg QD. Rehabilitation Status Prior to Hospital Discharge Findings from comprehensive rehabilitation September 2012) and PT/OT reports: medicine re-evaluation (3 Tardieu Scale assessment performed and compared to initial assessment on 2 July 2014 ((Section 2.6.3.). Severe extensor posture, global dyskinetic movements including tongue. Poor head control, feet in equinovarus position. Inability to stand without support Ability to make sounds but no comprehensible vocalization Hearing appeared intact. Ability to fix eyes on people, interacted by laughing and smiling when spoken to. Responded to music, story-telling, visual stimulation in a similar fashion Inability to ascertain severity of present and potential cognitive impairment. Recommendations for management included: • Initial rehabilitation management “as an inpatient in a paediatric rehabilitation centre specializing in neurological rehabilitation”. • Use of botulinum toxin for management of dystonia/spasticity. • Use of dopaminergic drugs (levodopa mentioned specifically) • Consideration of intrathecal baclofen Oromotor function evaluation and videofluoroscopy were done 9 September 2012. The assessment concluded: “severe Oro-Pharyngeal Vincent Foundation Clinical Case Compendium: Case 1 Page 10 of 38 Dysphagia characterised by poor lip seal and bolus preparation, persistent tongue thrusting resulting in premature spillage and delayed trigger of the swallow reflex preceded by bolus filling in valleculae and pyrifom sinuses. Although nil aspiration was noted in this study, it cannot assumed that the patient is not at risk of aspiration, in view of significant base of tongue residue and delayed swallow reflex trigger.” Course of Chronic Hypoxic-Ischemic Brain Injury Principal observations Treatment since hospital discharge included PT, OT, and oromotor therapy on a regular basis. According to nursing and therapists’ notes, he appears to have made some modest progress in motor function, spasticity, and contractures but no recent formal evaluations have been done. By daily descriptions, his receptive language skills appear to be significantly better than verbal expressive language, and non-verbal communication strategies are used. Oromotor function improved such that nasogastric feeds were discontinued on 4 November 2012. At present he appears to do well with both solids and liquids orally. An autologous stem cell infusion was done in August 2013. This was followed by epoetin alfa treatment. The stem cell blood type was A(-); volume 71.5 mL, total nucleated cells 4.7 x 108 with 99.9% viability. No other details about the procedure and follow up are available at this time. In May – June 2014, he received short trials of Stilnox (zolpidem) and Ritalin (methylphenidate). The doses and times are noted in Section 2.3. These brief treatments were given both individually and in combination. On higher doses of Stilnox no sedative effect was noted; in fact his baseline level of activity appeared to increase, as did his heart rate. By contrast, Ritalin appeared to have a calming effect that lasted as much as 24-48 hours. Ritalin also appeared to be associated with a sad demeanour and insomnia. With a combination of both drugs, the Stilnox effect described above was dominant. 1.1.3 Birth History 31-year-old mother of Asian (Siamese) descent. G1P1 Amniocentesis done at approximately 20 weeks gestation (see findings in Medical and Surgical History). Full-term gestation without documentation of Vincent Foundation Clinical Case Compendium: Case 1 Page 11 of 38 complications except as related to abnormal fetal ultrasonography and subsequent amniocentesis. Delivered by Cesarean section. Birth weight 3.4 kg. 1.1.4 Family History Both parents in good health. Male sibling born (approximately) May 2008 in good health. Female sibling (cousin, now adopted) approximately 9 years old in good health. Nephews: 2 male children of paternal uncle with alkaptonuria. 1.2 CLINICAL PROBLEMS FOR EXPERT PANEL ASSESSMENTS In your assessments, please include those following clinical issues that are relevant to your area of expertise and feel free to add others. 1.2.1 Acute Brain Injury Event The degree of brain injury that resulted from this patient’s hypoxic event was severe although concurrent injury to other organs based on the available data was modest: elevations of liver transaminases were minimal, there was no evidence of acute kidney injury, and echocardiography demonstrated good myocardial function. However, noted is a significant elevation of CPK, which may occur in rhabdomyolysis. The fact that the AST was elevated, albeit mildly, while ALT elevations were minimal, further support consideration of concurrent rhabdomyolysis. Questions: Was the possible co-existence of transient rhabdomyolysis a significant finding in this setting? Given the clinical findings and studies performed, are there other potential underlying conditions to consider? 1.2.2 Neuromotor Dysfunction and Spasticity Previous treatment recommendations have included drug therapy to ameliorate muscle spasticity and to modulate CNS neurotransmitter balance. He has undergone a brief trial of zolpidem and methylphenidate treatment. The possible use of botulinum toxin and intrathecal baclofen has been raised and he has Vincent Foundation Clinical Case Compendium: Case 1 Page 12 of 38 received an autologous stem cell infusion. The patient’s cerebral palsy-like motor dysfunction, as well as consequent physical disabilities from muscle spasticity and contractures, doubtlessly affect physical rehabilitation, skills development, cognitive development, and health in general. His records indicate on-going physical and occupational therapy efforts, which include speech and language. Questions: Was the trial of zolpidem and methylphenidate sufficient to determine benefit? Is there a potentially beneficial drug regimen and, if so, with what goal(s)? What would constitute a protocol for a proposed drug regimen, how should this be coordinated with other efforts, how can side effects be addressed, and what metrics could be used to guide ongoing treatment? Regarding the autologous stem cell infusion, are there subsequent tests to be done and is there recent new stem cell or related research observations of potential benefit? How can the treatments provided by physical, occupational, and speech therapists be better coordinated and synergistic? In the hospital, the patient had several assessments with a Tardieu Scale (Section 2.6.3.). What roles should this, or other assessment tools, play in long-term treatment planning? Is there the need for reassessment of the therapies provided by home health caretakers; how can treatment coordination between all players best be implemented? Are there potential roles for other therapies such as non-invasive transcranial therapies (i.e. magnetic stimulation or ultrasound), acupuncture, Chinese herbal medicine, or other alternative medicine interventions? 1.2.3 Language, Communication, and Cognition The impression is that the patient vocalizes but has very limited recognizable speech. Records indicate comprehensible nonverbal communication, raising the issue of the degree to which language and other forms of expression are limiting communication and cognitive performance. There have been numerous previous recommendations about enabling the patient’s ability to communicate. For understandable reasons, most of these have focused on nonverbal means of communication. Vincent Foundation Clinical Case Compendium: Case 1 Page 13 of 38 Questions: Is the patient’s vocal language disability a fait accompli, or are there verbal and non-verbal communication tools and technology that currently exist or are in development to be explored? Would any other concomitant or novel treatments (such as for muscle spasticity and hypertonicity) be of any benefit? Is it likely that the patient’s pre-existing speech and language difficulties play any role in rehabilitation efforts? 1.2.4 Anthropometric Growth The patient’s weight and height have increased modestly over the intervening time since hospitalization. Upon closer examination (see Section 2.5.), statural growth (height) percentiles and z-scores have progressively diminished to zscores of less than -1.0. Although body weight has increased about 3 kg over this same interval, this increase reflects sustained but very poor weight percentile ranks and z-scores. Weight percentile has been consistently less than the 2nd percentile with z-scores in the -2.0 to -2.5 range. Questions: Does he have undernutrition/malnutrition (despite current caloric intake)? Is this having an adverse impact on recovery? Are there reasons to consider underlying malabsorptive or hormonal perturbations? Is there a practical need for a metabolic/nutrition evaluation of energy intake and needs (taking into account his energy consumption). If so, what baseline and subsequent anthropometric or other measures of nutritional status would be useful and what parameters should be used. 1.2.5 Hydration According to the patient’s recent intake records, there is good daily fluid intake, with an average in excess of 2,000 mL per m2 per day. Under usual circumstances this would be considered more than adequate to maintain hydration. However, central nervous system diabetes insipidus leading to excessive urine production may occur in patients with CNS injury. Physical and/or cognitive limitations may affect a handicapped child’s ad lib access to water in order to compensate for the urine losses. Also, his unmeasured losses may be increased in his tropical Vincent Foundation Clinical Case Compendium: Case 1 Page 14 of 38 environment. No documentation of urinary concentrating capacity or daily urine volumes is identified. Questions: Is chronic under-hydration a significant contributing factor in this patient’s growth impairment? If so, how can this best be evaluated and treated? Vincent Foundation Clinical Case Compendium: Case 1 Page 15 of 38 SECTION 2: CASE 1 Supplemental Information and Appendices SUPPLEMENTAL INFORMATION AND APPENDICES 2.1 RADIOLOGICAL ASSESSMENTS 2.1.1 CT Scan Reports 2.1.2 MRI Scan Reports Time after event Axial images in FLAIR, diffusion, Coronal T2, and Sagittal T1 weighted sequences. Essentially normal study. Specifically: 5 hours 2.1.3 ● ● ● ● No cerebral thrombosis or acute infarct Normal grey-white differentiation Normal basal ganglia No AVM 2 days Axial images in T1, T2, diffusion, and GRE sequences; Coronal in T2 sequence and Sagittal in T1. Acute hypoxic-ischemic injury posterior parts of (right > left lentiform nuclei indicating areas of acute hypoxic-ischemic injury in basal ganglia 21 days Axial images in T2 FLAIR, T1 diffusion, Coronal images in T2, Sagittal images in T1. New areas of hypoxic-ischemic injury in globus pallidi substantia nigra, and periventricular white matter, all bilaterally. Prior ischemic foci in putamina now in subactute phase Cerebral atrophy 45 days Axial images in FLAIR, T2, T1, and diffusion, Coronal images in T2, Sagittal images in T1. No new abnormalities or foci of injury seen Degree of cerebral atrophy unchanged Sizes of ventricles and cortical sulci same as previous study Normal MRS study PET Scan Reports Vincent Foundation Clinical Case Compendium: Case 1 Page 17 of 38 2.2 METABOLIC AND NEUROMETABOLIC TESTING 2.2.1 EEG Report 20.06.2012 An inpatient routine EEG recording was performed on 20.06.2012 with the patient in ICU. Activation procedure of photic stimulation was done. Background Activity & interictal EEG The overall cerebral rhythms are slow and consists of diffuse polymorphic delta activity (2.0-3.5 Hz, 20-200uv) and some theta activity (5- 6 Hz. 20-40 uv) and low voltage beta. Sleep spindles are not evident. Photic driving was poor. There is no significant response to deep noxious stimulus, Impression; This EEG of 20.06.2012 shows diffuse slow wave cerebral rhythms indicating diffuse cortical dysfunction or drug effect (encephalopathy). Suggest to repeat later. 2.2.2 EEG Reports (21.6.2012, 22.6.2012, 23.6.2012, 19.7.12) Vincent Foundation Clinical Case Compendium: Case 1 Page 18 of 38 2.2.3. Laboratory studies during early hospitalization (abnormal values indicated in red) Days after injury 20-Jun 20-Jun 21-Jun 21-Jun 21-Jun 22-Jun 22-Jun 22-Jun 23-Jun 23-Jun 24-Jun 27-Jun 30-Jun 9-Jul 9.1 12.1 13.4 13.5 13.2 12.8 Hb (g/dL) 11.9 10.9 9.5 WBC (x103) 21.7 14.6 14.4 18.6 19 19.4 16.8 13.3 % Neutrophils 83 86 68 64 69 66 71 71 Platelets (x103) 323 286 295 279 362 458 615 576 Sodium (mmol/L) 130 132 137 137 136 133 133 129 134 137 134 138 132 133 Chloride (mmol/L) 95 96 103 103 104 100 99 101 101 102 97 102 100 97 Potassium (mmol/L) 3.7 3.1 3.5 3.8 3.8 4.2 3.9 3.0 3.6 5.1 4.3 4.2 Urea (mmol/L) 4.6 2.6 1.8 2.5 2.7 2.3 3.2 3.7 3.2 4.3 3.3 1.9 2.9 3.2 Creatinine (mmol/L) 59 31 40 29 31 32 35 34 31 39 39 29 1.93 2.12 Calcium (mmol/L) 1.98 Magnesium (mmol/L) 0.85 2.17 2.06 2.16 2.46 0.77 Phosphorus (mmol/L) 1.17 Uric acid (mmol/L) 0.09 0.92 1.99 ALT (IU/L) 36 34 32 63 49 50 AST (IU/L) 65 52 45 87 82 94 GGT (IU/L) 25 19 20 31 37 73 Urinalysis Glucose 56 Negative RBC/heme/myoglobin 4+ Negative Vincent Foundation Clinical Case Compendium: Case 1 Page 19 of 38 Days after injury 20-Jun Micro RBC (/uL) 20-Jun 21-Jun 21-Jun 21-Jun 22-Jun 22-Jun 23-Jun 23-Jun 24-Jun 27-Jun 400 8.9 845 10.5 Free T4 (pmol/L) 9-Jul 369 30.3 8.1 0.9 3574 450 194 LDH (IU/L) TSH (mIU/L) 30-Jun Nil CRP (mg/L) CPK (IU/L) 22-Jun 702 0.167 12.6 Ammonia (umol/L) Lactate (mmol/L) 44 34 0.7 Plasma Amino Acids Normal Urine Organic Acids see note* Urine Orotic acid/creat 0.65 Plasma carnitine Normal Acyl carnitine Normal * “Marked increase 3-OH bulyrate (?butyrate) and acetoacetate. Possibilities: succinyl CoA3 ketoacid transferase deficiency or severe ketoacidosis See Fukao T. Succinyl CoA3 ketoacid transferase (SCOT) deficiency. Orphanet encyclopedia, September 2004. https://www.orpha.net/data/patho/GB/uk-scot.pdf Vincent Foundation Clinical Case Compendium: Case 1 Page 20 of 38 2.3 MEDICATIONS AND TIMELINES Vincent's Meds and Doses up to March 2013 35 Prevacid 30 Artane Dose (mg) 25 Valium 20 Baclofen 15 Nootropil (mL) 10 5 0 9/8/12 10/18/12 11/27/12 1/6/13 2/15/13 3/27/13 Date 16 4 Zolpidem 14 3.5 Methylphenidate 12 3 10 2.5 8 2 6 1.5 4 1 2 0.5 0 4/21/14 Oxytocin (mL) Dose (mL) Dose (mg) Vincent's Meds and Doses after May 2013 0 6/10/14 7/30/14 9/18/14 Date Vincent Foundation Clinical Case Compendium: Case 1 Page 21 of 38 2.4 GENETIC ANALYSES 2.4.1 Amniocentesis - karyotype RECEIVED DATE/TIME: 13/02/07 1200 COMMENTS: CULTURE #: 071049 AF GA: 20 WKS G1P0 LMP: UNK EDD: 26/06/07 CLINICAL DIAGNOSIS: ABNORMAL ULTRASOUND FINDINGS AMOUNT OF AF RECEIVED: 20 ML FLUID APPEARANCE: CLEAR PELLET SIZE / APPEARANCE: LARGE / CLEAR DATE OF COLLECTION: 12/02/2007 CHROMO KARY AF GTG-banded cells/colonies scored : 16/16 GTG-banded cells analysed/karyotyped: 5/5 Cultures analysed : 3 Estimated band level: 500 BPHS Karyotype : 46,XY Cultures indicate a male karyotype with no apparent chromosomal abnormalities. The result confirms earlier normal FISH findings. Vincent Foundation Clinical Case Compendium: Case 1 Page 22 of 38 2.4.2 Amniocentesis - FISH RECEIVED DATE/TIME: 13/02/07 1200 SOURCE: UNCULTURED CELLS FROM AMNIOTIC FLUID CLINICAL INDICATION: ABNORMAL ULTRASOUND DATE OF COLLECTION : 12/02/2007 FISH PROBES: AneuVysion Multicolor DNA Probe Kit (Vysis) (CEP 18/X/Y-alpha satellite, LSI 13 and 21) No. of cells/probe examined: 50 FISH nomenclature: nuc ish(DXZl,DYZ3)xl,(RBl,D18Zl,D21S259,D21S341, 021S342)x2 FISH indicates a male fetus with normal copy numbers of chromosomes 13, 18 and 21. However, the assay is unable to detect mosaicism occuring below 20% at the established analytical sensitivity of 95%. This test is not meant to be a standalone test. Please correlate FISH findings with karyotype results. This test was developed and its performance characteristics determined by the Cytogenetics Laboratory, Department of Pathology, SGH. The above probes have been cleared and approved by the FDA for clinical use. 2.4.3 Microarray and Sequencing Studies performed for further evaluation of possible velo-cardio-facial syndrome. Results reviewed by Dr. Shprintzen. A whole genome exome sequencing analysis was done in conjunction with microarray analysis. The exome sequencing found mutations in the following genes: 1 2 A clinically significant known deleterious mutation was found in the CHD8 gene (c436G>A Val/Met) (OMIM*610528) which is altered in patients with Autism Spectrum Disorder (ASD). CHD8 is located on chromosome 14q11.2 and the occurrences of the condition are de novo. A clinically significant known deleterious mutation was found in the TBX1 gene (c1178C>T–aa Thr/Met) (OMIM*602054) which is altered in patients with velo-cardio-facial syndrome (VCFS, OMIM#192430). TBX is located on chromosome 22q11.21 and the inheritance pattern of the condition is autosomal dominant or sporadic. Vincent Foundation Clinical Case Compendium: Case 1 Page 23 of 38 3 4 5 A homozygous mutation in both copies of MTRR, at 5p15.31, a gene associated with homocystinuria. A mutation in BRCA1, a gene associated with breast cancer. A mutation in COL2A1, the gene associated with Stickler syndrome. The CGH microarray analysis showed three copy number variants (CNVs), all of the duplications. Two of these CNVs were on the X chromosome and are known to be normal variants. The third was on chromosome 18 at the q21.1 band and is in a noncoding portion of DNA (intronic). Dr. Shprintzen did not believe that the findings supported a diagnosis of velo-cardio-facial syndrome. 2.5 PHYSICAL GROWTH 40% 0 Height Percentile 35% -0.2 Height z-score 30% -0.4 25% -0.6 20% -0.8 15% z-score Percentile Case 1 Height (percentiles and z-scores) -1 10% -1.2 5% -1.4 0% 60 70 80 90 Age (months) Vincent Foundation Clinical Case Compendium: Case 1 Page 24 of 38 Case 1 Weight (percentiles and z-scores) 0 -0.5 Percentile 8% -1 -1.5 6% -2 4% -2.5 -3 2% Weight Percentile Weight z-score Weight z-score 10% -3.5 0% -4 60 70 80 90 Age (months) Vincent Foundation Clinical Case Compendium: Case 1 Page 25 of 38 Case 1 Weight and Height values 19 117 Height (cm) 115 17 114 16 113 15 111 112 110 14 Height (cm) Weight (Kg) 18 109 13 108 9/18/14 6/10/14 3/2/14 11/22/13 8/14/13 5/6/13 1/26/13 10/18/12 107 7/10/12 12 2.6 Weight (Kg) 116 Date NEUROLOGY AND NEUROMUSCULAR EVALUATIONS (See full rehab evaluation in hospital record) 2.6.1 Neurological Status as of 30.08.2012 At 5 + years his general condition is satisfactory. He is alert, looks around and makes sounds. He is non-verbal and non-ambulatory. There is fairly good eye contact and he enjoys watching television. There is asymmetrical dystonic spastic quadriparesis (left > right) with some athetoid posturing and tongue thrust especially when he is upset. There is dystonic torticollis with intermittent head tilt to the left and postural scoliosis. On stance (on the standing frame), his knees are straight and he can plantigrade his feet. The neck needs support. There is thumbln-palm deformity on the left side. He can cross-sit well, although he has a stooped posture (poor trunk control) and the head control is intermittent. The overall spasticity scoring (Modified Ashworth Score) is about Grade 1+/2 on the left side. Systemic examination is within normal limits. Vincent Foundation Clinical Case Compendium: Case 1 Page 26 of 38 2.6.2 Neurological Status as of 13.09.2012 Neurological assessment Able to fix eyes on people around him, able to laugh and smile when talked to especially by parents. Severe abnormal posturing of body, dyskinetic movements affecting limbs, trunk and oro-motor including tongue. Pupils: 2 mm reactive to light, reactive to threat. Cries and groans, no comprehensible vocalization. Posture post correction and at rest in ATNR. Hearing appears intact Head control still poor (floppy) Minimal voluntary movement noted during examination Feet in equinovarus position Upper limb Tone: Right increased (MAS 2) Left increased (MAS 3) Power: Unable to elicit objectively due to spasticity and dyskinetic movements of both upper limbs, at least 1-2/5 Dystonic movements noted during the examination but some voluntary resistance felt on attempt to passively extend right elbow, right wrist Reflexes: RIGHT LEFT biceps triceps brisk brisk brisk brisk PROM cannot get full range cannot get full range Lower limb Tone: Right increased (MAS 3) Left increased (MAS 3) Power: Unable to elicit due to severe spasticity of both lower limbs Vincent Foundation Clinical Case Compendium: Case 1 Page 27 of 38 RIGHT LEFT brisk brisk up going brisk brisk up going Reflexes: knee ankle extensor PROM contracture at ankle contracture at ankle Sensation: appears intact Function Poor head control on sitting up with support C- shaped trunk with extensor thrust on attempt to sit longer, flexible scoliosis noted Not able to stand with support Stand: dependent Not able to walk Totally dependent IMPRESSIONS Hypoxic brain injury resulting in severe movement disorder (dystonia with underlying spasticity) Minimally conscious state Unable to ascertain severity of cognitive impairment Dysphagia needing modification in mode of feeding RECOMMENDATIONS In view of his current neurological and functional sta it is recommended that the patient is to be managed as an inpatient in a paediatric rehabilitation centre specializing in neurological rehabilitation. The movement disorders need to be intervened optimally as it directly affects his energy expenditure and his future functional gains. Optimization of medications that would significantly reduce the dystonic movements need to be explored.Further, dopaminergic drugs such as levodopa should be looked into. Another option is trial of intrathecal baclofen if dystonia is not well controlled with the above medications or if there is poor tolerance to the above/develop adverse effects. Vincent Foundation Clinical Case Compendium: Case 1 Page 28 of 38 Botulinum toxin injection for focal management of dystonia/spasticity should be added into the management of high risk musculoskeletal regions prone to developing contractures such as ankles, knees, wrist and hand. A combination of management must be looked into i.e. use of appropriate orthoses, medications and serial casting where appropriate. Nutritional status should be optimized and feeding option and regime must be explored in view of his current (at that time) gastrointestinal concern and dsyphagia. The proposed programme may take up to 6 months or so in a rehabilitation setup specializing in neurological rehabilitation. Most children who have sustained moderate to severe brain injury/insult will have some degree of cognitive, physical and or behaviour deficits. Improvement (neurological and functional) after a brain injury happens at a different rate for every child but usually continues for a long time. It is pertinent to realize that the recovery is most rapid in the early stages. Therefore, acomprehensive paediatric rehabilitation team in an appropriate paediatric .rehab, setup will be able to address the above concerns and work with the child and family to maximise the recovery. This is comprised of the following: Continuous medical assessment and management. Provision of therapy services (physiotherapy, occupational therapy, speech and swallowing, psychology and behavior) Neuropsychological and clinical psychology assessment and management Case Management services where appropriate Family Support Ongoing Education about Brain Injury to caregiver 2.6.3 Physical and Occupational Therapy Status as of 12.9.2012 Current Intervention The patient’s parents and carers have been shown how to continue on-going programme of positioning and stretching to try to control his hypertonic synergies, reduce his reflex uncontrolled movements and reduce the associated risks, including:1 Range of motion exercises for both Upper and Lower extremities Purpose; To maintain joint flexibility and muscle length Vincent Foundation Clinical Case Compendium: Case 1 Page 29 of 38 2 24 hour positioning management; Purpose: To maintain the daytime intervention done by OT and PT. The intervention will be ineffective if the child is left to adopt destructive posture during the hours spent in bed. inhibiting spasm by positioning (supine, sitting; prone and prone standing) normalize tone with weight bearing training improve normal body alignment and symmetrical posture by positioning, with the use of positioning aids and lycra suit. Supine, Prone, Side lying - using grasshopper system Sitting - Paediatric wheelchair, grasshopper system (current system does not offer enough support for patient’s head control) Standing –Jenx Humprey Prone Stander 3 Righting and equilibrium reactions facilitation: Using gymball and grasshopper system. 4 Sensory stimulation: Purpose: To improve body awareness Joint sensation by weight bearing exercise (standing, 4 point kneeling) to inhibit abnormal muscle tone Tactile by touching different type of textures and surfaces Visual by using RBW (Red, Black and White) colour to encourage visual tracking and facilitate head movement Auditory by singing and storytelling session 5 Head and Trunk Control Training: in prone and sitting facilitated using Grasshopper system 6 Oral Placement Therapy Programme -initiated and supervised by paediatric dysphagia specialised Speech and Language Pathologist (once per week) and carried out daily by caregivers Vincent Foundation Clinical Case Compendium: Case 1 Page 30 of 38 7 Speech: Using positioning to help inhibit hypertonic patterns to aim to facilitate head and shoulder control and to help promote efficient breathing patterns During all treatment interventions language, singing, stories etc are used to encourage the patient’s involvement and enjoyment Summary and Recommendations A suggested Daily Schedule has been provided to give a possible framework for Caregivers to follow for home/on-going interventions based on the patient’s current physiotherapy, occupational therapy and speech and language interventions which would also include the following:24 hour postural programme is recommended to be continued to try to prevent musculoskeletal complications arising from long-term hypertonic synergy patterns - a comprehensive mattress and sleeping posture system has been ordered and awaiting delivery Weight-bearing activity /standing should be continued with a minimum of 6 hours per week weight bearing through the acetabulum/hips to reduce risk of pelvic migration and wind-swept hips. It is also recommended that the patient continue with his physiotherapy, occupational therapy and speech and language therapy upon return home or if moving onto a specialised paediatric rehab facility which would then coverContinued detailed oral placement therapy programme to improve swallowing Continued communication work to find a suitable system to facilitate the patient’s ability to communicate Continued work to enhance any neuro-plasticity allowing improvements to his dyskinesia with more voluntary movement control and inhibition of his reflex patterns and involuntary dystonia and synergies. Vincent Foundation Clinical Case Compendium: Case 1 Page 31 of 38 TARDIEU SCALES UPPER LIMB : INITIAL (Approx. late June-early July) RIGHT R2-R1 Joint/ Muscle LEFT R2 (PROM) X/Rl 140° 0/140° Sh./Vertical Adductors 2/120° R2 (PROM) 140° 40° 180° 1/140° Sh. /Internal Rotators 1/140° 180° 0° 170° 0 /170° Elb./Flexors 2/155° 170° 15° 0° 140° 0/l40° Elb./Extensors 2/140° 130° 5° 0° 90° 0 /90° Elb./Pronators 2 /45° 90° 45° 0° 90° 0 /90° Elb./Supinators 1 /90° 90° 0° 0° 90° 0 /90° Wr./Flcxors 1 /90° 90° 0° 0° 70° 0 /70° Wr./Extensors 1 /70° 70° 0° Hand/palmar Intcrossei & FDS Thumb in full palmar flexion 0° Thumb in full palmar flexion X/R1 R2-R1 20° 40° Thumb LOWER LIMB : INITIAL (Approx. late June-early July) RIGHT Joint/ Muscle R2-R1 R2 (PROM) X/Rl 25° 70° 2 /45° Hip/ Extensors 25° 65° 2/ 40° 10° 130° 5° 25° LEFT X/R1 R2-R1 2/ 30° R2 (PROM) 70° ip/ Adductors 1/30° 65° 35° 2/ 130° Kn./ Extensors 2/ 130° 130° 10° 180° 2/175° Kn./ Flexors 2/165° 180° 15° 35° 2/10° Ank./ Plantarflexors 4/35° 10° 25° Vincent Foundation Clinical Case Compendium: Case 1 40° Page 32 of 38 UPPER LIMB: 13 September 2012 RIGHT Joint/ Muscle R2-R1 R2 (PROM) X/Rl 0° 140° 0/140” Sh./Vertical Adductors 0° 180° 0/ 180” 0° 170° 0° LEFT X/R1 R2-R1 1/ 140” R2 (PROM) 140” Sh. /Internal Rotators 1/ 180” 180” 0” 0/170” Elb./FIexors 1/170” 170” 0” 140° 0/140” Elb./Extensors 0/140” 140” 0° 0° 90” 0 /90° Elb./Pronators 0 /90” 90” 0° 0° 90” 0 /90° Elb./Supinators 0 /90° 90” 0° 0° “ 0° 90” 0 /90° Wr./Flexors 0 /90° 90° 0° 70” 0 /70° Wr./Extensors 0 /70° 70” Hnd./palmar Interossei & FDS Thumb still in full palmar flexion Thumb still in full palmar flexion 0” 0” Thumb LOWER LIMB : 13 September 2012 RIGHT Joint/ Muscle R2-R1 R2 (PROM) X/Rl 0° 70° 1 /70° Hip/ Extensors 0° 65° 1/65° 10° 130° 0° 5° LEFT X/R1 R2-R1 1/70° R2 (PROM) 70° Hip/ Adductors 1/65° 65° 0° 1 / 130° Kn./Extensors 1/130° 130° 0° 180° 2/ 180° Kn./ Flexors 1 /180° 180° 0° 35° 2 / 30° Ank./ Plantar flexors 2 / 20° 35° 10° Vincent Foundation Clinical Case Compendium: Case 1 0° Page 33 of 38 2.6.4 Speech and Language Evaluation as of 2.1.2013 Communicating what he wants with Yes /No: The patient is able to shake his head for ‘No’. This is sometimes accompanied by a vocalization that is heard as an /o/, a clear /no/ or an approximation of the word. He blinks his eyes for ‘Yes’. This is usually accompanied by a slight nod of the head or a vocalization of ‘ye’ or ‘eh’. His yes/no communication is in response to questions by the clinician, Conductor or the nurse e.g. “Do you want to play with bubbles?” His responses are consistent during speech therapy and at home. Communicating what he wants by looking at a choice of four pictures: The patient has a portable communication book containing pictures of objects that he needs and daily activities. The pictures are arranged four per page, on the top / bottom right and top / bottom left side of the A4 sheet. The patient is able to scan all four pictures before looking at the picture of an activity or object that he wants. The pictures are organized according to categories of ‘drinks’, ‘toys and leisure activities’, ‘favourite songs’, ‘seats’, and ‘body parts’. He also has these pictures categorised and secured by keyrings. Communicating by hand tapping or swiping on a picture/ icon : The patient is trying out hand-tapping a Yes / No toggle on the iPad. He has better control over his left hand and is able to tap ‘yes’ most of the time. However, the iPad is touch sensitive and requires precision, so there are times when he rests his hand on an icon too long or touches a wrong icon. The iPad’s small size means that only two icons at most can be displayed, in order for the patient to succeed in touching the correct icon. Communicating with a yes/no switch The patient has recently tried using a domed light switch to help him communicate yes/no more effectively. He is able to slowly move his left hand to touch the switch to answer yes/no questions. We may move on to using a Jelly Bean switch for communication as appropriate. Vocalising At the moment, the patient is able to say /m/and /ah/, and approximations of ‘no’, ‘yes’ and ‘more’. However, due to difficulties controlling muscle movements, these vocalisations are inconsistent. Vincent Foundation Clinical Case Compendium: Case 1 Page 34 of 38 SECTION 3: CASE 1 Evaluations and Guideline Recommendations EVALUATIONS AND GUIDELINE RECOMMENDATIONS 3.1 PHARMACOLOGICAL INTERVENTIONS Based on recent videos in the above patient, there is a symptom complex seen that includes a disattention to verbal stimuli and a perpetuating restlessness, combined with a fairly consistent dorsal hyperextension, dystonia/spasticity. One direction to approach such a symptom complex from is the hypothesis of an impaired homeostasis of oxygen based neurotransmitters in the brain, which may occur in addition to other features after brain injury. Such a hypothesis would consider the possibility that the availability of one or more of such neurotransmitters may be impaired, either due to a lack of production in the brain or due to a leakage through an insufficient blood brain barrier after brain damage. There could be several neurotransmitters which could be affected, such as amino acid or monoamine based neurotransmitters which could be underactive or overactive, or whose neurologic outflow could have an imbalance between them. Important also is to consider the “now” situation only, in the sense that although previous drug applications may have resulted in previous reactions or homeostatic disturbance, or even damage, their pharmacological actions will by now have played out due to metabolic binding and breakdown, amongst others. That means the neurological symptom complex that is seen in the above patient at the time of the videos was a result of a stable “new” homeostatic neurotransmitter environment after brain injury. If this is true, then one can postulate the following: The observed symptom complex may be partially due an abnormality in the Glutamate/ GABA based system with features of dystonia and deficient attention. Zolpidem is a GABA agonist which, in uninjured persons causes sedation, but in some patients after brain injury results in improvement of neurological disabilities such as impaired consciousness, cognition or impaired motor features and then, as the dose increases, leads to sedation. In the above patient, there was no significant change seen in neurological disability, and there was also no sedation, even after dose escalation. Vincent Foundation Clinical Case Compendium: Case 1 Page 36 of 38 There may be an abnormality in the monoamine based system with deficient attention, which in the monoamine homeostasis may point to a relative deficiency in noradrenaline and dopamine, and a relative overexpression of serotonin activity. A pharmaceutical that counters noradrenalin/ dopamine deficiencies is methylphenidate, which blocks dopamine and noradrenaline transporters in the brain, and hence results in an increased concentration of dopamine and noradrenalin within synaptic clefts, countering such deficiencies. The above patient received methylphenidate, which had a calming effect, but resulted in a sad demeanour. Upon concurrent application of zolpidem and methylphenidate, the zolpidem effect dominated. In theory, further insights could be gained from scans on brain metabolism such as 99mTcHMPAO SPECT and 18FFDG PET scans, as they would show metabolic changes that may not be picked up clinically, but such procedures should be contemplated only if information garnered from them could lead to a therapeutic benefit for the patient. 3.2 NUTRITION AND NUTRITIONAL SUPPLEMENTS (i.e. creatine, neurotransmitter precursors etc.) Vincent Foundation Clinical Case Compendium Case 1 Page 37 of 39 3.3 3.4 3.5 REHABILITATION INTERVENTIONS AND STRATEGIES 3.3.1 Physical Therapy 3.3.2 Occupational Therapy 3.3.3 Speech and Language Therapies 3.3.4 Education COMPLIMENTARY AND ALTERNATIVE MEDICINE TREATMENTS 3.4.1 Acupuncture 3.4.2 Eastern Herbal treatment ADDITIONAL INTERVENTIONS OF INTEREST 3.5.1 Intrathecal Baclofen 3.5.2 Deep Brain Stimulation 3.5.3 Botulinum Toxin Vincent Foundation Clinical Case Compendium Case 1 Page 38 of 39