Annual report Jan-Dec 2013 FINAL DRAFT 2
advertisement

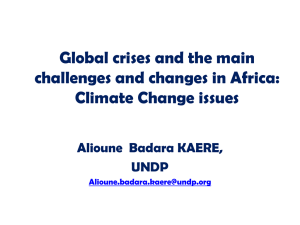
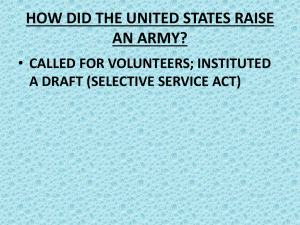
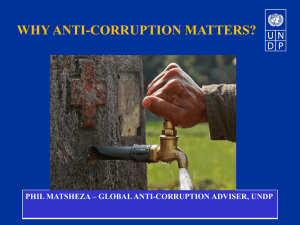
ANNUAL REPORT JANUARY - DECEMBER 2013 South Africa UNDP Support to the Limpopo Health Sector UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Contents Executive summary ................................................................................................................................. 3 1. Background & Context..................................................................................................................... 6 2. Overall progress overview ............................................................................................................... 7 2.1 Sub-programme: Health Professionals Volunteerism and Capacity Development ................ 7 2.1.1 Recruitment and placement of volunteers ................................................................................ 7 2.1.3 Registration of pharmacists and nurses ..................................................................................... 8 2.1.4 Volunteer well-being .................................................................................................................. 8 2.1.4 Knowledge enhancement of the volunteers ......................................................................... 10 2.1.5 Contribution of the volunteer programme to the health sector .......................................... 10 Figure 6: Number of Repatriated Doctors in 2013 ........................................................................ 13 3. 4. 5. 6. General Administration and Management .......................................................................... 14 Implementation Strategy Review .................................................................................................. 14 4.1 Participatory/Consultative processes .................................................................................... 14 4.2 Quality of Partnerships .......................................................................................................... 14 Management Effectiveness Review .............................................................................................. 15 5.1 Quality of Monitoring ............................................................................................................ 15 5.2 Timely delivery of outputs ..................................................................................................... 15 5.3 Resource allocation ............................................................................................................... 15 5.4 Project Risks and Actions ....................................................................................................... 18 Implementation challenges ........................................................................................................... 21 6.1 Programme funding ............................................................................................................... 21 Annexure1: Phase III Alignment to Provincial and National Priorities .................................................. 21 2 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Executive summary This is the fourth and last year of implementation for the UNDP Support to the Health Sector in Limpopo programme. The major focus in 2013 has been to execute the activities as agreed upon in the programme document, within the relative scope reviews during the course the year. During the reporting period, not much progress was made due to financial constraints as a result of organisational changes within the Department, and being placed under administration for several months. Since activities in the three sub-programmes, namely; Health planning support programme, Knowledge Management and Leadership Development as well as MDGs, Monitoring and Evaluation System were suspended in 2012, no implementation progress can be reported over this period. The sub-programmes were suspended at the request of the Department, which included the suspension of the recruitment of UNVs. By December 2013, the programme retained 17 volunteer doctors, whilst 11 had been repatriated. From July 2013, the Health Professions Council of South Africa (HPCSA) revised its previous regulation, which gave provision for volunteers practicing in the country for a period longer than six months to practise without following various confirmation processes. The new regulation requires that foreign qualifications be verified by the Educational Commission for Foreign Medical Graduates (ECFMG). Due to this development, the volunteers may not be registered with HPCSA in order to practice until these requirements have been fulfilled. The recruitment of nurses and pharmacists could not resume not only because of the financial situation, but most importantly, due to the strict requirements of registration, as reported in the 2012 annual report. The current programme cycle will end in September 2014. Terms of reference for the final evaluation of the programme have been developed for the appointment of an evaluation team. The process of developing a framework for new project cycle has been discussed and agreed upon. Based on the establishment of the focus areas of the programme, the draft of the document will be presented by UNDP in early 2014. The Steering Committee convened during the first quarter of 2013, at which the department committed to funding the recruitment and placement of doctors, whilst the other sub-programmes remain suspended due to financial constraints. In December 2013, the Department re-assigned the programme to a different directorate, designating the current discussions of the new programme document to a new Focal person. The programme had an opening balance of US$136 216.87 in January 2013. An income of R7,500,000 (US$ 1,196,211. 45) was received in August 2013. The total programme expenditure in 2013 is R 9,969,792 (US$ 1,084,852.25), with an opening balance of (US$ 249,320.24) in January 2014. 3 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Programme contribution to the provincial and national strategic goals In the various areas of specialization, the UNV volunteers in 13 hospitals distributed across the five districts of the province have made extraordinary and dedicated contribution to the South African medical system in the province of Limpopo. Whilst the implementation of programmes for combating HIV and AIDS, STI, TB and other communicable diseases has been enhanced in the largely rural areas of the province, the service volunteers have contributed towards the following three MDGs, (i) (ii) (iii) Goal 4: Reduce child mortality Goal 5: Improve maternal health Goal 6: Combat HIV/AIDS, malaria and other diseases The Department of Health Limpopo has recorded an improvement in the TB treatment success rate from 75% to 77.8% between 2010 and 2012. Access to tertiary services has improved through the increase of tertiary disciplines from 75% in 2010 to 77.8% in 2012. The anti-retro viral treatment service points have been increased from 483 to 493 (Annual Performance Plan, 2013/2014). The programme retained 28 doctors in January 2013, of which 67% of them are specialists, serving in 13 hospitals within the 5 districts of the province. The average number of cases handled have increased significantly, with the doctors contributing 0.05 % towards the overall service volumes provided by the health institutions in the province. The average number of hours served by each doctor per hospital is 151 per month. Over time, the doctor to patient ratio has decreased from 18:100,000 in 2011/12 to 16:100,000 in 2012/13, due to the increased service volumes. The department has reported a percentage increase in patients using regional hospitals services, varying from 64% in 2009/10 to 65% in 2010/11. This can be attributed to the placement of volunteer specialists in regional and district hospitals, evidenced by the increased the number of cases attended within the districts themselves. Additionally, the assignment of volunteer doctors in the management of HIV/AIDS clinics has added value in the provision of services to patients. This is demonstrated by the upward access to comprehensive HIV and AIDS, STIs, care, treatment, management and support of patients from 10.4% in 2009/10 to 49.5% in 2011/12 4 Programme contribution to provincial and national strategies UNDP Support DoHSD Strategic Goals 2010/11 National Department of Health Ten Point Plan National Government Outcome No. 2 Immediate Outcomes Intermediate Outcomes Final Outcomes Strategic Impact Increased culture of volunteerism Effective corporate governance is provided Strategic leadership and creation of a social compact for better health outcomes; Improved hospital performance vis-ὰ-vis organizational management and development Appropriate human resource management and development is provided National Health Insurance (NHI) implemented; Sound financial management practice is promoted Improved quality of health services; Comprehensive HIV and AIDS, TB, STI and other communicable diseases programmes are implemented Overhauled healthcare system Improved human resources, planning, development and management; Revitalized infrastructure Accelerated implementation of programmes for HIV and AIDS, STIs, TB and associated diseases; Mass mobilization for better health for the population; Reviewed Drug Policy; and Strengthened research and development Improved Doctor-patient ratio Improved knowledge and access to health related information Diversification and increase in the number of health professionals Districts Health Services and Primary health Care services are strengthened Quality of health care is improved Emergency medical services are improved Tertiary services are developed Infrastructure development and maintenance is improved A long and healthy life for all South Africans”. UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 1. Background & Context UNDP Support to the Health Sector programme is a partnership with the Department of Health in Limpopo, with the objective to support the Department in its effort to improve health care service delivery in the province. Since the inception of the partnership in 2002, UNDP has assisted the Government of Limpopo in addressing the shortage of health personnel caused by brain-drain; and building capacity of local health professionals to improve service delivery and management of health care in the province. During the first 2 phases of programme implementation, the programme focused on the recruitment and placement of doctors. In the current phase (Phase III), which began in 2009 October, in addition to the recruitment and placement of volunteers, the scope of the programme expanded to include 3 additional complementary sub-programmes: Health Planning Support Programme (Health economics) Knowledge management and leadership development; and Monitoring and evaluation, which includes the domestication of MDGs. The programme made a contribution in addressing the 4 key challenges as identified in the Annual Performance Plan, Vote 7, 2010 /11- 2013/14. These challenges are: Mismatch between health service demands and available resources; Shortage of skilled health professionals; Inadequate evidence-based decision making, planning, and resource allocation; and Inadequate management skills at some key level of the department. The province is largely rural with an estimated population of 5, 404, 868 people which constitutes 10.4 % of the South African total population. Being a rural province, the resultant brain drain creates a huge shortage of health professionals in the province as health professionals leave the province for better opportunities locally and internationally. The province currently has 40 hospitals, 22 health centres and 416 clinics. 6 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 2. Overall progress overview 2.1 Sub-programme: Development Health Professionals Volunteerism and Capacity The mobility of medical professionals from the most rural to the tertiary hospitals within the province is an old phenomenon. Local and international migration of South African doctors for better remuneration and better working conditions remains very high. Similarly, the willingness and ability of certain expatriates to work in difficult conditions where local health professionals are reluctant to serve is low. The option of private practice for those doctors who remain becomes attractive because of its smaller workload as opposed to the very high demand in the public sector. As much as the workload for experienced doctors in rural hospitals may be reduced in the presence of Community Service doctors, the demand for their supervision may not always be effective. This sub-programme provides the much needed assistance to the Department to alleviate the impact of the scarcity of doctors through the recruitment of United Nations Volunteers who serve in mostly rural hospitals and Community Health Centres for duration of one year. 2.1.1 Recruitment and placement of volunteers A total of 28 doctors were retained into 2013. The programme did not recruit new doctors during this reporting period, however, the Terms of Reference were revised and adopted in late September 2013. Amongst the 11 doctors repatriated in 2013, two had served for the maximum 6 years permissible within the UN system. Following a Project Steering Committee meeting held in March 2013, the recruitment was set to begin upon receipt of resources. A transfer of funds was received by UNDP in August 2013, after which the programme identified five candidates for possible recruitment. On an on-going basis, potential candidates continue to be solicited. A decision to waive the interview process, taken in 2011 in order to expedite the recruitment process has been reviewed. This arose from feedback received from hospitals regarding the inadequate skills of some of the volunteer doctors recruited during this period. From 2013, all candidates whose profiles have been submitted to the department for screening would undergo interviews, enhanced through the Skype technology in order to mitigate identity concerns. 2.1.2 Registration on volunteer doctors In July 2013, the Health Professions Council of South Africa (HPCSA) enacted a new regulation, recognising the registration of volunteer services to exceed six months. Alongside other volunteers in the country, the UNVs have been thus been re-classified as long-term assignments, requiring them to initiate the verification of qualifications to HPCSA through the Educational Council of Foreign Medical 7 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Graduates (ECFMG). Whilst the new policy has been communicated to the Department, the registration of the doctors has not been renewed. Due to the length of this process, by December 2013, only four doctors whose reports have been transmitted to HPCSA. 2.1.3 Registration of pharmacists and nurses Despite the consultations made in 2012 regarding a possible provision for volunteer registration of nurses and pharmacists, no further progress was made in advancing their recruitment during this reporting period. 2.1.4 Volunteer well-being The monitoring of living conditions of volunteers is a standard activity conducted by the PMU, UNV Field Unit as well as the UN Security Service. A number visits to the doctors were conducted in 13 hospitals where the volunteers are assigned. Feedback has been received from the hospital and clinical management personnel through solicited meetings. A close relationship between the PMU and the hospitals is crucial, considering the movement of hospital management, in order to provide a better understanding of UN Volunteers conditions of service. Although one incident of harassment outside hospital premises was reported, however, volunteers are constantly reminded to be discreet and vigilant for any potential threat to their security in an outside the hospital premises. (i) Living conditions Whilst accommodation provided by the hospitals within their premises varies according to locality and availability, there are isolated incidents where preference is given to community service doctors, allied medical practitioners and doctors recruited through other government programmes. As such, the volunteers have either been relocated to smaller or vacated from their apartments. Although a single maintenance related matter was received from one of the rural hospitals. Where no similar reports were received, living conditions of the volunteers have generally met the expectation. (ii) Treatment of volunteers by local health professionals Constant engagement and reports from the hospitals and the respective supervisors regarding performance issues and professional support of the volunteers is very crucial. Although most of the district hospitals have continued to renew contracts of the volunteers, more negative feedback has been received post-repatriation. There is thus a growing need for the PMU to actively involve the clinical management of the hospitals to solicit accurate progress reports of the doctors in order to take appropriate action. On the other hand, following their exit, doctors who have served in the tertiary hospital have raised issues ranging from misalignment and displacement by the hospital. 8 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) As much as most of the volunteers are also viewed as committed, having adapted to the culture of their institutions, the fact that they are employed under relatively modest salary conditions leaves a perception of them as inferior. (iii) Workload and compensatory time-off (CTO) Flexible working schedules for some of the doctors placed at the tertiary hospital are still a challenge to achieve. In this institution, mobility of specialist is high, resulting in high workload levels for the volunteers to absorb. New managers refuse to adopt and accommodate the practice of CTO in order to crises created by the shortfall of specialists at the institution. One specialist was suspended after a series of disagreements with the supervisor related to CTO. Figure 1: Average number of hours and cases attended in 2013 1200 1000 800 600 400 200 0 (iv) Jan Feb Mar April May June Jul Aug Sep Oct Nov Dec Cases attended 612 840 453 496 645 403 270 429 429 398 404 312 Hours worked 167 174 201 231 239 191 189 136 204 276 169 154 UNV workload The workload of volunteers continues to reflect an outlook of their contribution at their duty stations. As captures in Figure 1 above, the average hours worked per month among the doctors changed significantly from the second quarter as large number of volunteers, mainly assigned in the periphery were gradually being repatriated. 9 UNDP Support to the Health Sector in Limpopo 2.1.4 Annual Report (January –December 2013) Knowledge enhancement of the volunteers Training and academic exposure are highly recognized in volunteer acknowledgement, motivation and ultimately, retention. Particularly in South Africa, volunteers are mostly deployed to serve in various hospitals, unfamiliar with local epidemiology, the practice of health care and the organization of the health system in the country. Workshops and conferences have been used as tools for development and competence enhancement. During this reporting period, volunteers have attended various conferences relevant to their areas of specialization to keep abreast of developments in medicine. 2.1.5 Contribution of the volunteer programme to the health sector The recruitment and placement UNV volunteers have been invaluable in maintaining the quality of health care service delivery in Limpopo. Across the five districts of the province, 13 hospitals have benefited. The volunteers continue to support the attempt by the department to foster the Primary Health Care approach to healthcare. Their participation in community outreach, serving the local clinics and community health centres has assisted in health promotion and preventive activities, timely diagnosis and advance a team approach to healthcare services. Whilst providing specialist care within the tertiary, regional and district hospitals, their skills have been useful managing the rate of transfer of patients within and outside the province with reduced costs. Most importantly, volunteers have filled the difficult void due to their willingness to work in difficult and rural conditions, where local health professionals are difficult to retain in similar circumstances. Figure 2: Volunteers per Area of Specialization 10 3 2 2 3 2 2 2 1 1 10 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Figure 3: Number of Volunteers per Hospital 7 4 3 3 2 2 1 1 1 1 1 1 1 Figure 4: Distribution of Volunteers per District Sekhukhune, 6 Capricon, 10 Mopani, 8 Vhembe, 4 11 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Table 1: List of volunteers in the programme in 2013 Name and Surname Area of Specialization Hosting Hospital Status of UNV 1. Bautista, Jose Family Medicine Mecklenburg In service 2. Thomas Kaung Family Medicine Mecklenburg 3. Tawheed Emam Surgery St Ritas 4. Ebrima Jarra Family Medicine Elim Repatriated 5. Karchenko Andriy Anesthesiology Philadelphia Repatriated 6. Sharonova Tatiana Pediatrics Lebowakgomo Repatriated 7. Nuzhat Sultana Ahmed Family Medicine Zebediela In service 8. Serguei Nikiforov Surgery Letaba In service 9. Lioudimila Nikiforova Obstetrics and Gynecology Letaba In service 10. Zhyrnyi Sergii Surgery Letaba In service 11. Iryna Danylenko Internal Medicine Polokwane In service 12. Akeem Adedolapo Family Medicine Botlokwa In service 13. Misra Rajeev Cardiology Polokwane In service 14. Kapoor Pardeep Kumar Cardiology Polokwane Repatriated 15. Sergiy Bocharov Anesthesiology Polokwane Repatriated 16. Ivantchenko Nikolaevitch Neurology Polokwane Repatriation pending 17. Jerome Hubahib Internal medicine Polokwane In service 18. Delinikaytis Sergey Orthopedic Surgery Polokwane In service 19. Shahid Mehmood Family Medicine Siloam In service 20. Patrick Mulindwa Obstetrics & Gynaecology Sekororo In service 21. Khan Inamullah Family Medicine Sekororo In service 22. Abu Minah Family Medicine Sekororo In service 23. Godwin Attamah Family Medicine Dilokong In service 24. Narendra Kumar Sharma Ophthalmology Polokwane/Mankweng Repatriated 25. Dieudonne Takam Family Medicine Maphutha-Malatji Repatriated 26. Pyai Win Gaung Paediatrics Letaba Repatriated 27. Benicio Torralba Ophthalmology Elim Repatriated 28. Azmi Ahmed Internal Medicine St. Ritas Repatriated Repatriated In service 12 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Figure 5: Number of Years in Service per Volunteer in 2013 7 6 5 4 3 2 1 0 1 2 3 4 5 6 Years of service 6 5 4 3 2 1 No of volunteers 2 0 0 1 4 3 Figure 6: Number of Repatriated Doctors in 2013 Series1 Q1 0 Q2 5 Q3 3 Q4 3 13 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 3. General Administration and Management The persistent resource constraints and the suspension of other sub-programmes have maintained the PMU under the operations of the Programme and Administration Coordinator with support and oversight from UNDP. The Knowledge Management Programme Officer and Programme Manager vacated the positions in September and November 2012 respectively. 4. Implementation Strategy Review The Steering Committee (PSC), co-chaired and represented by UNDP and the Department, still assumes the policy and advisory role on strategic issues and ongoing oversight. The disbursement of resources by the department, at the representation of the PSC guided the essential activities which had to be sustained, that the Programme Management Unit (PMU) planned to implement for the period in review. 4.1 Participatory/Consultative processes The Steering Committee convened during the first quarter to streamline and harmonize the 2013 deliverables as the current phase of the programme nears its end in September 2014. The department committed to an allocation of R15.4 million for 2013 to fund the recruitment and retention of doctors, however, other sub-programmes remain suspended due to inadequate resources. New discussions about the review of the programme as well as the development of the project document for the next phase resumed and will be completed before the September 2014. More focus has been placed on the contractual arrangements of the volunteers in 2013. 4.2 Quality of Partnerships The partnership between UNDP and the Department has been effective in the provision of high level supervisory and technical support to the programme. As the donor and beneficiary of the programme, the Department has been actively involved in the planning of activities and programme activities, through representation and participation in PSC engagements. Several challenges relating to health institutions have been effectively dealt with. Whilst resource constraints have been a great test to the achievements of results, the programme has adapted to ensure that the available funds are disbursed effectively. 14 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 5. Management Effectiveness Review 5.1 Quality of Monitoring Although the Steering Committee had one seating during this reporting period, meetings between the focal points have been held to discuss implementation challenges, resource constraints and the future of the programme as it nears its end in 2014. During the course of 2013, quarterly progress reports provided insight on challenges presented at the level of health institutions in the field, resource utilization, risks and other issues in the implementation of the programme. 5.2 Timely delivery of outputs Since the funds were received in August 2013 and the recruitment profile approved in October 2013, the recruitment process could not yield new recruits at the end of the financial year. By December 2013, the programme had 17 volunteers, a number reduced from 28. 5.3 Resource allocation The opening balance of funds as at January 2013 was US$ 136,216. 87 An income of R7,500,000 (US$ 1,196,211) was received in August 2013. The total programme expenditure in 2013, as depicted in Table 2, is R 9,969,792 (US$ 1,084,852.25), with an opening balance of (US$ 249,320.24) in January 2014 15 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Table 2: Financial expenditure report per sub-programme: January - December 2013 16 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 17 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 5.4 Project Risks and Actions RISK TYPE DESCRIPTION IMPACT SUGGESTED MANAGEMENT RESPONSE RESPONSIBLE PARTY Organizational Non-provision of UNDP or UNV inputs to ensure efficient/effective programme deliverables. Ineffective scope management of programme may disrupt continuity of UNV assignments, affecting delivery levels. Regular Project Steering Committee meetings and bilaleral consultations. UNV PO / PMU Project Evaluation Limited capacity of the UNV Programme office in supporting UNV volunteers. Retention strategies through ongoing training and enhancement of UNV skills. UNDP/ DOH Regular interaction and appropriate segregation of responsibilities between the PMU and the UNV PO. Financial Irregular funding schedules Insufficient commitment that allows for appropriate administration of contracts of volunteers and programme staff Over expenditure and intermittent accounting affects monitoring and proper planning Voluntary separation of volunteers due to uncertainty and lack of security. Provide regular progress and expenditure reporting to expedite continued funding PMU/ UNDP/ DOH Align Annual Workplans to available resources PMU 18 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) RISK TYPE DESCRIPTION IMPACT SUGGESTED MANAGEMENT RESPONSE RESPONSIBLE PARTY Operational Voluntary separation of programme staff. Delivery levels affected negatively due to insufficient capacity. Efficient management of operational processes and information PMU / UNDP Security of the office premises Loss or damage to property Political Change in political/ administrative leadership Negative impact on continued leadership, strategic and financial support of the programme Regular consultations and PCS meetings to concretize long-term commitment. UNDP / DOH / PSC Regulatory Change in country regulations for clinical practice Lack of compliance by the volunteers due to additional requirements required by regulatory institutions disallows UNV practice. Constant engagement of the department for additional support to ensure attainment of the requirement documentation for compliance. Regulatory Amendment of regulations for foreign citizenship by the government Non-provision of HPCSA registration and work permits has occupational risks and could render the work and stay of UNVs illegal Lack of valid work permits, Diplomatic ID Cards render the work and stay of UNVs illegal Timely processing of contract extensions to expedite renewal of work permits 19 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) RISK TYPE DESCRIPTION IMPACT SUGGESTED MANAGEMENT RESPONSE RESPONSIBLE PARTY Security Ineffective monitoring and security and safety of UNVs at duty stations Injury to UNVs and loss or damage to property may weaken retention capacity of the programme. Regular security visits of PMU, UNDSS and UNV teams to duty station UNDP/ PMU Security alerts and information regarding potential threats disseminated to UNVs PMU UNVs encouraged to report threats of potential danger to the PMU for immediate action 20 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) 6. Implementation challenges 6.1 Programme funding The impact of financial resource shortage has had an impact on achieving deliverables for the 2013 financial year. The late receipt of funds made it difficult to expedite the recruitment of doctors. Annexure1: Phase III Alignment to Provincial and National Priorities Relevant National Outcome A long and healthy life for all South Africans Objective: To increase the life expectancy of our citizens and ensure that all people have access to health care. Relevant National Activities (RSA) Ensure a well-coordinated roll-out of antiretrovirals (ARVs) with a specific emphasis on effective roll-out of the preventative mother to child treatments; Integrate HIV and tuberculosis (TB) services; Strengthen maternal health services; Develop a national strategy for chronic diseases; Conduct hospital audit process in 2010, with the view to improving hospitals. Relevant National outputs Reduce the mortality rate; Reduce the impact and prevalence of HIV and AIDS and Tuberculosis, and Ensure an effective healthcare system. Medium Term Strategic Framework (Relevant to Health) Transform the public health system so as to reduce inequalities (National Health Insurance) in the health system, improve quality of care and public facilities, boost human resources and step up the fight against HIV and AIDS, TB and other communicable diseases as well as lifestyle and other causes of ill-health and mortality. 21 UNDP Support to the Health Sector in Limpopo Annual Report (January –December 2013) Department of health and Social Development (Limpopo province) Vision: A health promoting and developmental to the people of Limpopo Mission: The department is committed to provide sustainable Health and Developmental services through a comprehensive and integrated system Department Health and Social Development Strategic goals Implement comprehensive HIV and AIDS care, treatment and management, Tuberculosis (TB), Sexual Transmitted Infections (STIs) and other communicable diseases programmes Strengthen Districts Health Services and Primary health Care services Human Resources management issues Relevant Millennium Development Goals (MDGs) Reduce child mortality Improve maternal health Combat HIV/AIDS, Malaria and other diseases Relevant UNDAF Outcome Democracy, good governance and administration Envisaged Programme Outcomes Improved healthcare service delivery in Limpopo Province Increased culture of volunteerism Improved hospital performance vis-ὰ-vis organizational management and development Integration of health economics in health service planning Improved knowledge and access to health related information Improved monitoring and evaluation capacity Expected Programme Outputs Recruitment of PMU staff: 1 Programme Manager; 2 Programme Officers; 1 Programme Assistant and 1 Programme Driver Recruit and place 75 UNV medical doctors, 8 UNV Clinical Engineers, 30 UNV Pharmacists, and 15 UNV special Nurses Develop a framework for a mentorship programme strategy Develop and implement a leadership development seminar series programme targeting senior management of health facilities and health managers Develop guidelines and frameworks for effective health services planning Develop a concept document for the establishment of a health knowledge management centre in Limpopo province Develop and implement monitoring and evaluation system 22