Service Spec Kent Infant Feeding Service March 2014
advertisement

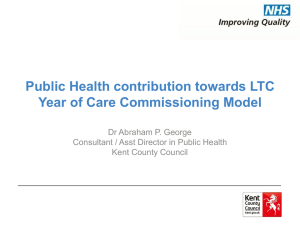
SERVICE SPECIFICATION FOR THE PURCHASE OF KENT COMMUNITY INFANT FEEDING SERVICE (excluding Medway) 1st October 2014 to 30th September 2017 This document defines the COMMUNITY INFANT FEEDING SERVICES purchased by Kent County Council Copyright © The Kent County Council 2014 This material may not be copied or published without the Kent County Council’s permission in writing 1. INTRODUCTION AND SCOPE Breastfeeding performance, both initiation and continuation are targets in the Public Health Outcomes Framework. Currently Kent is performing worse than local authorities in comparable areas. Community services to support infant feeding have been in place across Kent, funded by the former Eastern Coastal Kent and West Kent PCTs and through Children’s Centres funded by Kent County Council. Further funding has been made available to enable Kent County Council to tender for an integrated service This will be both universal and targeted to areas of highest need in line with the Marmot principle of proportionate universalism1. The scope is intended to widen with an emphasis on working more in settings with schools, workplaces, town centres and with media to promote the benefits of breastfeeding. This service must also cater for the needs of nonbreastfeeding mothers in a way that promotes the Marmot objective of achieving a healthier start to life. The new service is expected to start operating from 1st October 2014 and run for three years. There will be a period of mobilisation and handover prior to the service starting. This contract may be extended for a further year subject to agreement of both parties. The indicative cost of this Service is a maximum of £475,000, we would welcome bids that demonstrated how a quality service could be provided below this price. The Service will cover the following local authority areas as follows: Local Authority Area Number of births 2012 6-8 week breastfeeding prevalence (12/13) Dartford Borough Council 1,560 34.0% Gravesham Borough Council 1,472 38.4% Sevenoaks District Council 1,383 48.2% Tonbridge and Malling Borough 1,432 44.9% Council Tunbridge Wells Borough Council 1,326 56.9% Maidstone Borough Council 2,040 41.5% Canterbury City Council 1,419 42.7% Swale District Council 1,777 28.1% Ashford Borough Council 1,597 38.8% Dover District Council 1,257 33.4% Thanet District Council 1,654 32.5% Shepway District Council 1,230 32.3% Kent 18,147 43.2% And the following Clinical Commissioning Groups: Clinical Commissioning Groups NHS Dartford Gravesham and Swanley NHS West Kent NHS South Kent Coast NHS Canterbury and Coastal NHS Swale NHS Thanet NHS Ashford 1 6-8 week breastfeeding prevalence (12/13) 36.4% 47.8% 34.6% 42.2% 24.8% 32.5% 38.8% Marmot, M (2010) Fair Society, Healthy Lives: Strategic Review of Health Inequalities in England 2. BACKGROUND Successful infant feeding is important to the future health of the child. Breastfeeding specifically confers a number of health benefits to both the baby and to the mother; a report commissioned by UNICEF in 20112 described the economic benefits of breastfeeding. There is very strong evidence that breastfeeding prevents: four acute conditions in infants: gastrointestinal disease, respiratory disease, otitis media, and necrotising enterocolitis (NEC) breast cancer and other cancers in mothers. In addition the UNICEF reports that there is good evidence that if the number of babies receiving any breastmilk at all rose by 1% in the UK this could lead to a small increase in IQ. A very modest increase in exclusive breastfeeding rates could national prevent at least three fewer cases of Sudden Infant Death Syndrome annually. Increasing breastfeeding rates could lead to around a 5% reduction in childhood obesity Nationally the prevalence of breastfeeding is low compared to other European countries and this is reflected in Kent. Kent is also poor compared to other similar areas. Kent Breastfeeding Initiation 2010-11 (percentage of maternities where status is known) (Child and Maternal Health Observatory, 2012) The National Infant Feeding Survey 20103 found that the highest incidences of breastfeeding were found among mothers aged 30 or over (87%), those from minority ethnic groups (97% for Chinese or other ethnic group, 96% for Black and 95% for Asian ethnic group), those who left education aged over 18 (91%), those in managerial and professional occupations (90%) and those living in the least deprived areas (89%). Whilst mothers of first babies were more likely to start breastfeeding than mothers of second or later babies (84% compared with 78%), mothers who had previously breastfed a baby for at least six weeks were more likely to start breastfeeding their latest baby than those who had breastfed a previous child for less than six weeks or not at all (97% compared with 79% and 35%). These variations were evident in all countries and were consistent with the patterns found in previous 2 UNICEF UK (2012) Preventing disease and saving resourses:the potential contribution of increasing breastfeeding in the UK Information Centre for Health and Social Care (2011). Infant Feeding Survey 2010: Early Results. London: Information Centre. Available at: https://catalogue.ic.nhs.uk/publications/public-health/surveys/infa-feed-serv-2010-earl-resu/infa-seed-serv-2010-earl-resu-rep.pdf 3 surveys. The chart before shows the prevalence trend in the better and worst areas and the Kent average. A national problem which is replicated in Kent is drop-off rates. The Kent 2012/13 initiation rate was 72.1% and by the 6-8 week check prevalence was only 40.8% (Public Health Outcomes Framework). The following chart shows the reduction in prevalence over time in West Kent PCT. Chart showing reduction in prevalence at each 'check' for each Clinical Commissioning Group in west Kent area - 06/07-10/11 (pooled data) 100% At delivery At transfer/ discharge At 10 day check At 6-8 week check Coverage Percentage 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Dartford Gravesham & Swanley Maidstone & Malling WKW Clinical Commissioning Group West Kent Across Kent there has been a general lack of investment and in latter years some funding changes have resulted in further gaps in service. This has resulted in serious inequalities in service provision. The main components of this service have been: specialist lactation services advising mothers and their families specialist project management and training to professional groups (such as supporting the Baby Friendly Initiative) working in partnership with voluntary services such as the National Childbirth Trust, La Leche League and independent organisations to promote to women and their families the range of community service provision available and to promote to the voluntary sector any funding opportunities or resources media and publicity, for example promoting Breastfeeding Awareness Days, providing media interviews, generating positive press, production of leaflets and information, ekbaby website and social media The aim of the new service is to increase the uptake of the initiation and continuance of breastfeeding by facilitating service development and improvement. One identified barrier to successful breastfeeding is tongue tie. It is intended that existing arrangements for referral into this procedure will be reviewed with maternity commissioning with the aim of creating an integrated programme to support infant feeding during the course of this contract. 3. SERVICE CONDITIONS AND ENVIRONMENTAL FACTORS A barrier that has been identified nationally and locally is attitudes and beliefs. These maybe from the family culture, previous experiences and practices, or from the wider environment which is not supportive of breastfeeding in public for example. A local example of family influences was identified through a needs assessment which was undertaken in Swanley amongst teenage mothers. The author discovered through the questionnaire that the teenage mother’s parents had a huge part to play in their infant feeding decisions. A focus group was therefore held for grandparents. The conclusion was that there also needs to be some education for them in order to equip them to support the mother-to-be. The involvement of fathers is essential. 4. ROLES RESPONSIBILITIES and RESOURCES Provider: The provider will need to deliver all elements identified in this service specification and be responsible for delivering the outputs and outcomes described. They will also need to provide: All resources required for delivery Adhere to the service standards as outlined below Designated lead member of staff to liaise with the Commissioner for this contact Ability to be flexible, innovative and to ensure that any changes in good practice, guidance and legislation are incorporated into the running of the service Attend any performance monitoring and evaluation meetings, training, seminars, and other reasonable request Commissioner: The commissioner will need to agree the format and delivery method of the programme. They will also provide: Pre-paid fees for Baby Friendly Initiative accreditation Children’s Centres: are anticipated to carry out the following tasks: Co-ordination of peer supporter rotas (timetable of sessions to be run by peer supporters) Provision of premises for drop-ins, clinics and 1 to 1 interventions Resources for clinics and 1 to 1 interventions DBS vetting of all peer supporters Participate in Baby Friendly Initiative which includes training for all front line staff Maternity Units: Maternity units will be supporting the breastfeeding pathway by: working towards Baby Friendly Initiative accreditation supported by the provider Hosting ward-based and ante-natal peer supporters Health Visiting Teams: will be supporting the breastfeeding pathway: Working towards Baby Friendly Initiative accreditation To work collaboratively with the new service to achieve shared objectives 5. SERVICE OUTCOMES As a minimum this service will operate for 12 hours a day for 5 days a week. The service must have a flexible approach and staff able to deliver evening and weekend working if desirable based on identified need. Safeguards for any individuals working outside of these hours need to be put in place, for example Lone Working policies and home visiting should not be in place without rigorous safeguards and the agreement of a Home Visiting Policy with the commissioner. They should also be in line with the policies of organisations with which visits have been agreed, for example Children’s Centres. The new service must work closely with maternity services, health visitors, children’s centres, general practice, public health and communities. It must contribute to a seamless pathway and intervene to increase initiation and decrease the drop-off rates from the handover from maternity to health visiting that are evident. The NICE Topic-specific Advisory Group suggested that commissioned services ensure multiple access points through which women can be referred or contacted directly by peer supporters. Access points may include health centres, postnatal wards and community and hospital antenatal clinics, (because women who are provided with appropriate breastfeeding information during the antenatal period are more likely to initiate and continue breastfeeding), and drop-in centres or baby cafes. Kent County Council requires that the majority of peer supporter drop-ins are held in Children’s Centres. Where this is not the case alternative arrangements will need to be agreed by the Commissioner. Service models should focus on women who are least likely to breastfeed: young women, women with low educational achievements and those from disadvantaged backgrounds. The new provider will be challenged to achieve 45% partial or exclusive breastfeeding in all Kent CCGs at 6-8 weeks. Given that the UNICEF model is based on 45% of mothers exclusively breastfeeding at four months to achieve the projected savings, we expect the service to put in place plans to extend exclusive breastfeeding rates at 4 months. This will require fundamental changes in practice and in the cultural environment. Expected Service outcomes are: Increased quarter on quarter initiation prevalence rates (Public Health Outcomes Framework) Increased quarter on quarter prevalence rates at 10-14 days recorded by Health Visitors Increased quarter on quarter prevalence rates at 6-8 weeks (Public Health Outcomes Framework) and better data recording Demonstration of a universal service available to all women, with a more targeted approach in areas of highest need. An increased number of women reporting satisfaction at all stages of their journey until 26 weeks Baby Friendly Initiative accreditation must be achieved in all services by the end of the contract term The Service must provide accredited peer support training, supervision and refresher courses. To increase Welcome signage and engage with local authorities Mind the Gap plans for increasing breastfeeding Evaluation of workplace, school, primary care and other community setting interventions must be undertaken with the aim of making environments more conducive to breastfeeding. 6. THE RESPONSIBILITIES OF THE SERVICE 1. To work more closely with women in ways that women say they want in a way that empowers them to take control over decisions about their health and the health of their baby. Regular engagement work will be a key part of building understanding and should include women who are unlikely to breastfeeding so we gain better understanding of what may help them to do so. This may include working with the wider family of the women so they can better support them; e.g. fathers, Grandparents etc. 2. To co-ordinate community breastfeeding support provision and ensure that there are good relationships and excellent communication with and between partner organisations, including the voluntary sector 3. To extend the provision of breastfeeding support into a complete infant feeding service working with Kent Community Healthcare Trust to support weaning. 4. To ensure that all services provided have robust financial, clinical and managerial governance 5. To ensure services are provided universally but proportionately according to levels of deprivation to contribute to the reduction in health inequalities. 6. To work closely with midwifery units, health visiting teams and Childrens Centre to implement the national breastfeeding pathway 7. To ensure that signposting to other organisations/services which offer complimentary or enhanced provision both ante-natally and post natally as agreed with the Commissioner. (For example the National Breastfeeding Helpline and local La Leche League offer 24 hour support) 8. To be responsible for the achievement of the 95% coverage target re: 6-8 week breastfeeding data through liaison with the Child Health Information Service, General Practice and Kent County Council Public Health and provide progress reports back to general practice and children’s centres 9. To collect, analyse and interpret high quality data from a range of sources and provide reports to Kent County Council, District Councils and to Clinical Commissioning Groups. 10. To provide Community based lactation clinics in all district and borough council areas. Lactation Specialists should be registered and qualified to provide specialist advice to mothers. 11. Lactation specialists should also be part of the Tongue Tie pathway 12. To recruit, develop and supervise an adequate number of peer supporters who will have contact with mothers within 48 hours of birth in line with the NICE benchmarking tool, it is estimated that the number will need to rise to 50 whole time equivalents over the course of the contract To co-ordinate peer support networks (opportunities for sharing learning) in Children’s Centres in Kent including support to young parents through YAPS groups identifying areas where there are gaps in provision in order to ensure services are equitable. To provide ante-natal and hospital based peer support To ensure that peer supporters are part of the multi-disciplinary team To ensure that all peer supporters understand the limits of their capabilities and work within policy guidelines e.g. peer supports policy, Kent County Council policies To recruit a diverse range of peer supporters To re-imburse peer supporters for travelling costs and to ensure that crèche facilities are offered and made available when required. 13. To ensure that Kent Community NHS Trust and all Hospital Trusts achieve UNICEF Baby Friendly Initiative accreditation within the life of the contract (3 years). These Hospital Trusts are Maidstone and Tunbridge Wells NHS Trust, Dartford and Gravesham NHS Trust, East Kent Hospitals University Foundation NHS Trust. Medway Hospitals Trust provides services for both Medway and Kent This should include: Project management support for Baby Friendly Initiative programmes across Kent Comprehensive training sessions at an NHS venue for health visiting, paediatric and any midwifery staff that have not completed the session previously, including provision of all appropriate resources whilst providing updates as required to ensure professional are kept up to date Comprehensive audit of community staff knowledge and interviews to assess mother’s experience of care using BFI audit tool Achievement of Children’s Centre training programmes and GP eLearning Attending associated meetings with Community, Midwifery managers and GPs Updating the support information leaflets and websites and disseminate updates to staff leads 14. To support Primary Care through provision of training and professional support to enhance their role in promoting breastfeeding 15. To innovate and progress social marketing/community development approaches in areas where rates remain low despite peer support being in place 16. To make the best use of technology including the use of applications to educate and inform 17. To maintain a strong communication presence in Kent and use a range of channels to communicate with both the public and professional in an effective way. This may include a Kent wide website, social media, written literature, content on KCC cooperate website, campaigns etc. The organisation will need a strong communication plan that is agreed by the commissioner and articulates clear and consistent messages around infant feeding. This will need to set out any policy’s or safeguards for the use of social media and any specifications that apply to any websites, such as being smart phone accessible and legally compliant. Information about the service will to be available in a range of formats so that it is accessible to all parties including those with additional needed and makes the service appealing to those who may not traditionally access the service. The organisation will be expected to update information on a regular basis and review the communication plan with commissioners to reflect technological changes and up-grades. Consultation and engagement will be key to ensure the service is communicated in an effective way. 18. To pro-actively engage with the media and have in place a comprehensive media strategy and ensure there are links with KCC communications team 19. Lactation consultants should engage with GPs to support the Tongue Tie pathway. 20. To work with maternity and health visitor leads to promote Healthy Start 21. To work with Education services, schools, youth services and Kent Community Health Trust to influence the school curriculum re: breastfeeding promotion to include relevant information as required by young people to support breastfeeding later in life. 22. To work with local authorities to promote breastfeeding friendly communities including Welcome mark development 23. To work with workplace health leads in local authorities to make it easier for breastfeeding women to return to work 24. To have in place user satisfaction measures and regularly review and learn from user feedback 25. To build an evidence base of effective practice in Kent 26. To undertake any additional work that is identified to support infant feeding in Kent as agreed with the Commissioners 7. SERVICE PROCESSES AND STANDARDS Monitoring The Service Provider will be required to report quarterly by the 31st of the following month against all the Key Performance Indicators (attached). Reports will need to be prepared for the following geographic areas: Kent Kent Borough and District Councils Clinical Commissioning Groups Service User Review Process The provider must demonstrate appropriate effective service user and public involvement in the development, delivery and review of services by responding as appropriate to user surveys/questionnaires (see KPIs for more information). Quality Assurance The Service must work to national guidance and standards including New Baby Friendly Initiative Standards (UNICEF, 2012) Public Health Outcomes Framework (Department of Health, 2012) Healthy Child Programme (Pregnancy and the first five years of life) (Department of Health and Department for Children, Schools and Families, 2009) Healthy Child Programme: the two year review (Department of Health and Department for Children, Schools and Families, 2009) NICE guidance on antenatal and postnatal care replaced by CG 62 Antenatal Care Routine Care for the Healthy Pregnant Woman (NICE, 2003) and CG37 Postnatal care: Routine postnatal care of women and their babies (NICE, 2006) Healthy Lives Healthy People (Department of Health, 2010) Healthy Lives, Brighter Futures (Department of Health and Department for Children, Schools and Families, 2009) National Service Framework for Children, Young People and Maternity Services (Department of Health and Department for Education and Skills, 2004) Maternal and child nutrition NICE guidance 11(NICE 2011) Midwifery 2020 Programme: the Core Role of the Midwife Work-stream (Department of Health, 2010) Tackling health inequalities in infant and maternal health outcomes. Report of the Infant Mortality National Support Team. (Department of Health, 2010) Marmot, M. (2010). Fair society, healthy lives: the Marmot Review: strategic review of health inequalities in England post 2010. Maternity Matters: choice, access and continuity of care in a safe service (Department of Health, 2007) The Service must work to the principles of equal opportunities as detailed below. The Service must have a designated Child Protection Officer and have a Child Protection Policy. Staffing 1. This contract may be subject to TUPE arrangements 2. The provider will be responsible for sourcing and financing, where appropriate, suitable premises for community services. Risk assessments and Equality Impact Assessments should be undertaken to ensure that no individuals are discriminated against. For example premises should be accessible for all, including women with disabilities and those without transport. It would be expected that the majority of public facing services would be Children’s Centre based, lactation clinics may be hospital based and training related to the Baby Friendly Initiative would be local to the workforce. 3. Current Activity and Costs £475,000 per annum for 3 years, see Key Performance Indicators 4. The Service must ensure that all recruitment and employment of staff shall be conducted under the principles of equal opportunities in full compliance with the 2010 Equality Act. The Service must ensure that all staff and volunteers, who deliver the services under this agreement, even where they do not undertake the checks themselves (for example volunteers in Children’s Centres) are: (a) Subject to an Enhanced Disclosure from the Disclosure and Barring Service (DBS) And (b) Should a disclosure raise any past or current offences the Service Provider will confidentially discuss such disclosures with the appropriate commissioner During the period of this agreement offences committed by staff involved in the delivery of this service and which become known to the Service Provider, will be discussed in confidence with the lead commissioner Workforce Development Lactation Consultants must have the International Board Certified Lactation Consultant accreditation. Peer support co-ordinators should be trained and accredited and all other staff and volunteers will have an accredited qualification or be working towards accreditation. All staff should have annual appraisal and CPD plans. All volunteers must receive accredited training, supervision, Children’s Centre mandatory training and updates. Training provided for external staff e.g. health visitors, midwives, children’s centre and other staff groups must follow current guidance, be accredited where possible and include robust evaluation. Marketing and Communication The Provider must adhere to the marketing and communication guidelines set by Kent County Council and as agreed with the Commissioner including the use of relevant branding and logos. Compliments and complaints Service users should be consulted regularly about the quality and accessibility of services, to ensure that the service meets their expectations. The quality and safety of services will be assured through the use of the governance framework. This will include analysis of critical incidents, complaints and compliments, risk assessment, internal audits, continuing professional development identified through staff reviews and both monitoring of sickness and absenteeism and actions to mitigate against service disruption. The commissioner should immediately be informed of any critical incidents and action planned/taken. Equal opportunities In carrying out the Services the Service Provider will be “exercising public functions” for the purposes of section 149(2) of the Equality Act 2010. As such, the Service Provider is required to pay regard to the Public Sector Equality Duty under section 149(1) of that Act and to deliver Services accordingly. The Equality Act 2010 relates to service users and employees. The Service Provider has responsibilities’ as a provider to service users and as an employer to its employees. Services will respond positively to the needs of all groups who have a protected characteristic within the Equality Act 2010. These characteristics are race, religion or belief, sexual orientation, pregnancy and maternity, age, disability, gender and gender identity. The Service is expected to engage with these groups through all necessary means to ensure inclusion is in a positive and meaningful way. In delivery of any services commissioned on behalf of Kent County Council Providers must demonstrate awareness and be responsive to the accessibility and needs of groups described above either in or attempting to access services. Accessibility relates to (but is not limited to); physical and mental impairment, communication needs, those with either a hearing or sight impairment, translation/interpretation if English is not a first language, the expectation with regards to acceptance of individuals defined under gender identification, respect of faith and beliefs. The Equality Act 2010 replaces the Disability Discrimination Act 1995 (reviewed 2005). Proof of compliance will be required in the form of a current and up to date Access Audit with an action plan outlining any needs and how these will be addressed. An Equality Impact Assessment (EIA) is a requirement that the Service Provider will complete annually. The EIA will cover these characteristics: age, disability, gender, gender identity, race, religion or belief, pregnancy and maternity and sexual orientation, which need to be assessed against delivery. This should be submitted annually as part of the performance management programme. Health Inequalities Health inequalities are avoidable variations in health status of groups and individuals and are a complex issue. There is evidence that populations in areas with high deprivation experience higher morbidity and mortality than those areas with low deprivation (Marmot strategic review, 2010). Health inequalities are ultimately measured by Life Expectancy at Birth and All Age All-Cause Mortality rates and a range of shorter-term performance indicators set by the Public Health Outcome Framework. One of the success factors for improving public’s health for local authorities and Clinical Commissioning Groups will be assessed on how well they are reducing health inequalities in their area. Kent County Council Public Health have developed a screening tool (HIWIA) to enable all commissioning to be assessed in terms of the potential for increasing or decreasing Health Inequalities and it is required that all providers utilise this screening tool to evaluate the programmes they deliver and identify a targeted action plan to address to improve Health Inequalities outcomes. Six Ways to Wellbeing Six Ways to Wellbeing are actions that are shown by research to improve people’s wellbeing. They can’t change our circumstances but building them into our daily lives can help us feel better, no matter what our starting point. The list was drawn up by an independent think tank, The New Economics Foundation, which was commissioned by the government’s Foresight Project on Mental Capital and Wellbeing to review evidence on improving wellbeing in research studies from around the world. The Six Ways to Wellbeing and the Wheel of Wellbeing have been developed by the South London and Maudsley NHS Trust. The Six Ways – connect, give, take notice, keep learning, be active and grow your world – can improve your mood, strengthen your relationships and help you to cope when life doesn’t go to plan. It is a requirement that all programmes commissioned by Public Health actively contribute to the Six Ways to Wellbeing. Sustainability The concepts of ‘well-being’ and ‘sustainability’ are inextricably linked. The central purpose of Local Government Act 2000 was to give local authorities the ability, via enabling powers and community strategies to “improve the economic, social and environmental well-being of each area in its inhabitants and contribute to the achievement of sustainable development in the UK.” Since the Planning Act 2004, sustainable development has also been established as the statutory purpose of the planning system in which local authorities play a critical role. As it is now a statutory rather than a theoretical concept, a working definition of sustainability is required which can be found in the UK Sustainable Development Strategy 2005. This defines five principles of sustainability: Environmental enhancement: respecting the limits of the planet’s environment by protecting and enhancing it, its natural resources and biodiversity; Social justice: meeting the diverse needs of all people in existing and future communities, promoting personal well-being, social cohesion and inclusion, and creating equal opportunity for all; Sustainable economy: building a strong, stable and sustainable economy which provides prosperity and opportunities for all, and in which environmental and social costs fall on those who impose them and efficient resource use is incentivised; Sound evidence: ensuring policy is developed and implemented on the basis of strong scientific evidence, whilst taking into account scientific uncertainty as well as public attitudes and values; Community engagement: actively promoting effective, participative systems of governance in all levels of society. The provider must ensure that the above sustainability objectives and outcomes are fully addressed within their programmes. 7. POLICIES AND PROCEDURES In providing this service the following policies and procedures must be in place, implemented and adhered to along with any new policies that are put in place during the course of the contract: a) Quality assurance b) Complaints c) Equalities and diversity d) Health and Safety e) Recruitment and selection f) Induction and training g) Supervision and appraisal h) Adult/Child protection i) Environmental Management Systems j) Positive Disclosure k) Information Governance l) Clinical Governance m) n) o) p) q) r) s) Data Protection Lone working policy Serious Incident Policy Risk Assessment Framework Privacy Impact Assessment Business Continuity Policy Social Media Policy 8. PERFORMANCE MONITORING Baseline Performance Targets – Quality, Performance & Productivity Performance Indicator Heading Media Strategy 6-8 week data collection Indicator Undertake campaigns, media and advertising to include Start4Life and evidence of working with C4L Team including Kent wide website and use of technology i.e. applications 95% coverage achieved Method of Measurement Evidence that there is a communication plan in place with all local Borough and Districts in line with Mind the Gap and other local plans, portfolio of press releases/press coverage to demonstrate reach. Number of hits Published data Frequency of Monitoring Consequence of Breach Quarterly progress report to Public Health Commissioners N/A Quarterly Performance Indicator Heading Indicator Method of Measurement Frequency of Monitoring Quarter on quarter improvement in Kent and all local authority areas. Across Kent we would expect to see a 1% rise in prevalence annually. In addition the greatest improvements will be evidenced in areas with the lowest rates. Published data Quarterly Follow up of women to track longer term outcomes 1% random audit of outcome for each clinic by phone contact at four months of age spread across the year Audit Report Quarterly as above Baby Friendly Initiative Progress Kent Community NHS Trust to BFI full accreditation by end of March 2016. (Assessment fees pre- paid by Public Health)A staged plan for achieving this will be required by the 6 month review. 6-8 week prevalence Progress Report and evidence of stages achieved Quarterly to Public Health Commissioners Consequence of Breach Performance Indicator Heading Indicator Method of Measurement Frequency of Monitoring Quarterly as above Progress to Maternity BFI accreditation in all Kent hospital NHS Trusts by March 2016. (Assessment fees pre- paid by Public Health)A staged plan for achieving this will be required by the 6 month review. Progress Report and evidence of stages achieved Document and present evidence to locality managers that participants have achieved training outcomes through: completed workbooks, e-learning certificates, competency sign-off and BFI audit Training Records Quarterly as above 50 audit days per year. Audit Report Quarterly as above Provide BFI RAG progress report to Public Health Progress report Quarterly as above Consequence of Breach Performance Indicator Heading Specialist Lactation Support Indicator Method of Measurement Frequency of Monitoring Anonymised report showing activity through the period by CCG of mother Quarterly to Public Health Commissioners Provide qualitative data: anonymised non identifiable personal stories on mothers experience of using service A minimum of 4 Case Studies supported by interviews with women Quarterly as above Customer satisfaction at point of service offered for all mothers, minimum 10% coverage. Log of complaints and compliments with actions taken User Satisfaction Survey summary report Log Lactation Clinic records of number, presenting problem and treatment of mothers/babies attending clinics/referrals made (as a minimum 2 weekly specialist clinics to be held in each district authority area, spaced out over weekdays to enable women to access a clinic on any day of the week within reasonable travelling distance) Quarterly as above Consequence of Breach Performance Indicator Heading Peer Support Indicator Method of Measurement Frequency of Monitoring A 3 year plan to be put in place and monitored to ensure that peer supporters annually provide support and advice to 11,000 post-natal women within 48 hours of leaving hospital or of time of home birth(based on NICE peer support bench marking tool) Children Centre and other clinic records analysed Kent wide, local authority and CCG areas All peer supporters attending accredited Peer Support training courses Training Records Quarterly to Public Health & Child Health Commissioners Evidence participant outcomes-80% participants to pass course Evaluation reports Quarterly as above Evident enrichment for volunteersnumbers at each supervision session recorded Peer supporter records Quarterly as above Evidence partnership working in every District authority area (Mind the Gap health inequality plans)-minutes of meetings/action plans available as requested Quarterly as above Quarterly Consequence of Breach Performance Indicator Heading Indicator Method of Measurement Frequency of Monitoring Quarter on quarter increase in the number of mothers who are contacted ante-natally from Q2 2014/15 baseline Summarised contact logs by Kent/local authority area/CCG areas Quarterly Evidence that peer supporters are full volunteers with Children’s Centres and have had the necessary checks, where peer supporters also support hospitals these checks need to have been undertaken/ transferable Peer supporter records Quarterly as above Year on year increase in number of volunteers supporting groups, with evidence that the majority are working in areas of deprivation defined by local Mind the Gap plans Peer supporter records Quarterly as above Consequence of Breach Performance Indicator Heading Indicator Method of Measurement Frequency of Monitoring Evidence of qualitative data; Personal stories A Case study provided in each local authority district including interviews with mothers Quarterly as above Randomised audit of 10% mothers satisfaction with attendance at support groups Summary report Supporting primary care in their role for supporting Community BFI 5% of practices undertake training per annum Training log, certificates, evidence of e-learning Quarterly as above Supporting children’s centres in their role of supporting Community BFI All children’s centres to have received training over a 24 month period then a rolling programme of updates Training log, certificates Quarterly as above There will be challenges in each geographical area, the service will need to evidence plans as part of Mind the Gap local processes that show how they will address the inequality related to infant feeding. Evidence in Mind the Gap locality plans Quarterly Tackling Inequalities Quarterly as above Consequence of Breach Performance Indicator Heading Indicator Method of Measurement Frequency of Monitoring To work with local authorities to promote breastfeeding friendly environments Welcome scheme for Kent County Council implemented in all districts and boroughs as part of Mind the Gap within 18 months Publication of scheme, evidence of support resources and log of all participating venues who are accredited Quarterly as above To provide social marketing approaches in areas of low take-up Identify and work in partnership with 3 areas per annum (Using Bentley Christmas Tree model or similar methodology) Evaluation report Quarterly as above Consequence of Breach Performance Indicator Heading To work with Education, schools the KCHT C&YP Team to promote breastfeeding education as part of the curriculum To work with informal youth groups to promote infant feeding Indicator Method of Measurement Frequency of Monitoring Curricula Increase year on year the number of schools who include breastfeeding as part of the curriculum To work with youth services to determine the most effective way of introducing this education informally Quarterly as above Evidence of planning and evaluation Quarterly Consequence of Breach Performance Indicator Heading Indicator Method of Measurement Frequency of Monitoring To work with workforce leads in local authorities to enable breastfeeding mothers to return to work Breastfeeding Friendly scheme for inclusion in workplace health improvement plans. Quarter on quarter increase in number of workplaces with schemes in place Number of workplaces with verified schemes in place Quarterly as above The service has plans in place to measure uptake of services from groups that might be negatively impacted The service needs to ensure that use of services by the following groups are measured and included in performance reports: Age Disability Gender Race Beliefs/Religion Sexual orientation Pregnancy and maternity Marriage and civil partnerships Carers responsibilities Women living in deprived areas Women with low educational attainment Service monitoring Equity Audits Quarterly as above Consequence of Breach 9. Activity 9.1 Activity The provider will provide robust information during the life of the contract in relation to their activity, as detailed in section 8. Monthly exception reporting if not on track 9.2 Activity Plan / Activity Management Plan Not used for this contract 9.3 Capacity Review Not used for this contract REPORTING Reports must be submitted quarterly, by the 31ST working day of September, December and April for the duration of the contract. It may be necessary on occasion to request data and reports earlier, as breastfeeding is a Public Health Outcome Framework indicator. An annual report will be required by the end of April of each contractual year. Address for reports: PHperformance@kent.gov.uk Data will be gathered, analysed and displayed by provider. Reports should be submitted by the following areas Kent County Council Clinical Commissioning Groups Mind the Gap reports for Districts and Boroughs Any changes to the format of the report can be discussed between Provider and Commissioner to ensure it is useful to both sides throughout the contract term. Reports must cover Performance and Activity and indicators from the table above. PERFORMANCE MEETINGS Performance Meetings will be held quarterly or as requested by Kent County Council or the provider. The Service will be reviewed at 6 months and then annually during the life of the contract. Appendix 1 Glossary of Terms Community Infant Feeding Service Covering feeding during the first six months of life, a key aim is to increase breastfeeding rates because of the health benefits this results in for babies and mothers but it also includes supporting any woman who is experiencing difficulties feeding her baby by any method. Lactation Consultant A person qualified to advice on infant feeding, who has an International Board Certified Lactation Consultant (IBCLC). Work in partnership with health professionals they would help mothers with babies with latching difficulties, painful nursing, low milk production, or inadequate weight gain Lactation Specialist A person qualified to advise on infant feeding, the minimum qualification would be National Childbirth Counsellor or Association of Breastfeeding Mothers counsellor. Peer Supporter A person who has experience of breastfeeding her baby who volunteers to provide peer support to women who are experiencing difficulties breastfeeding. The peer supporter would have received training and attend regular updates and supervision from a Lactation Specialist. Baby Friendly Initiative (www.unicef.org.uk/babyfriendly ) BFI is an accredited programme of service improvement which is open to Maternity Units & NHS Community Trusts who provide midwifery and health visiting services. It is based on a set of standards which include policy development, adherence to the WHO code on infant formula, rigorous prescribed training and audit UNICEF (UNICEF.org.uk) United Nations Childrens Fund advocates for measures to give children the best start in life, because proper care at the youngest age forms the strongest foundation for a person’s future. UNICEF UK is responsible for The Baby Friendly Initiative. Public Health Outcomes Framework (www.phoutcomes.info) Public Health will be measured against a framework which sets out 66 health measures so councils and the Government are able to see real improvements being made and take any action needed Tongue Tie Tongue-tie is a problem that occurs in babies who have a tight piece of skin between the underside of their tongue and the floor of their mouth. It can sometimes affect the baby's feeding, making it hard for them to attach properly to their mother's breast. There is a procedure that can be undertaken to cut the skin to help feeding. Appendix 2 The location and number of breastfeeding groups and peer supporters will be agreed in partnership with the KCC Infant feeding programme management service. Lead Provider Childrens Centre Core service Peer support programmes per locality. These should be seen as a locality provision and shared across the centres of the locality. Recruitment of volunteer peer supporters from the local community who are mothers who have breastfed for at least 6 weeks. Aim for two new courses per year. Provision of volunteer status with up to date DBS, safeguarding and other necessary volunteer training. Estimate 20 new recruits per year Provision of a peer support coordinator/”breastfeeding champion” . This is a clerical role. JD available. 0.6 WTE per locality Provision of a training room for the ps training and for quarterly supervision of the breastfeeding volunteers. Deliver two peer support accredited courses per year for up to 12 mothers Quarterly ps training update/enrichment Fee for ps trainees to Greenwich UNICEF Baby Friendly Initiative for CCs One-off Fee to BFI for all CCs Training and audit for all staff (with HV service) Venues for training Resources for training Enable all staff to attend BFI training programme Manage requirements of BFI within the CC eg WHO Code compliance. Performance reporting Provide volume and reach data for the breastfeeding groups from data collated and inputted on estart Provide qualitative feedback of the peer support service from mothers. . KCC commissioned Infant feeding programme team Direct payment from Public Health Provide qualitative feedback of the peer support service from peer supporters Lactation Clinics-one per locality alongside peer supporters Provide lactation specialist LC or bfc with established organisations (NCT,LLL etc) Provide premises for group with lactation clinic Provide play worker at breastfeeding groups to support peer supporters with children This does not include any bf services funded by KCC that are not linked to CCs eg community BFI, data recovery , lactation services alongside