Head and Neck v5
advertisement

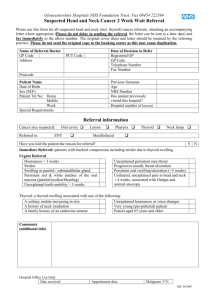
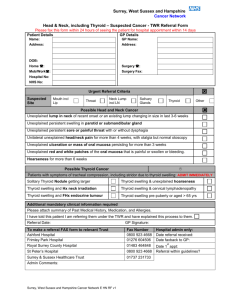
Head and Neck Cancer – Suspected Cancer TWR referral form Please fax this form back within 24 hours of seeing the patient for 24 hospital appointment within 14 days PATIENT’S DETAILS Surname First name(s) Address Date of birth Home telephone: Mobile/Work telephone: NHS number: Hospital number: REFERRER’S DETAILS (General Medical Practitioner or General Dental practitioner) Name Surgery address Surgery telephone Surgery fax GP’s Details (if not already included above) GP’s name Surgery name Surgery address Surgery telephone: Surgery fax: URGENT TWR REFERRAL CRITERIA Suspected site – Please tick as appropriate Mouth (inc. lip) Throat Neck Lump incl LN Salivary Thyroid Other glands Possible Head and Neck Cancer TICK Unexplained lump in neck of recent onset or an existing lump changing size in last 3-6 weeks Unexplained persistent swelling in parotid or submandibular gland Unexplained persistent sore of painful throat with or without dysphagia Unilateral unexplained head/neck pain for more than 4 weeks, with otalgia but normal otoscopy Unexplained ulceration or mass of oral mucosa persisting for more than 3 weeks Unexplained red and white patches of the oral mucosa that is painful or swollen or bleeding Hoarseness for more than 6 weeks Possible Thyroid Cancer Patients with symptoms of tracheal compression, including stridor due to thyroid swelling: ADMIT IMMEDIATELY Solitary Thyroid Nodule getting larger Thyroid swelling &unexplained hoarseness Thyroid swelling and Hx neck irradiation Thyroid swelling and cervical lymphadenopathy Thyroid swelling and FHx endocrine tumour Thyroid swelling pre-puberty or aged >65 years ADDITIONAL MANDATORY CLINICAL INFORMATION REQUIRED: TICK Attach summary of past medical history, medication and allergies Summary of past medical history, medication, and allergies attached? I have told this patient I am referring them under the TWR and have explained this process Referral letter attached? Referral date: Referrer’s signature TO MAKE A REFERRAL TO FRIMLEY PARK HOSPITAL, fax this form and any additional correspondence to: 01276 604506