Critical Incident Form (fillable MS Word format)
advertisement
")
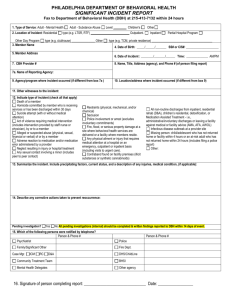
Mental Health Waiver Critical Incident Submission Form Person Reporting Contact Name Date of Incident Phone Number ( _/_ _/_ MH Waiver Agency Name _ ) Time of Incident _-_ :_ __AM/PM_ _ Incident Details Location of Incident Client’s Residence Nursing Home Community Other Location (please specify) Agency Office/Facility Incident Category Client Abuse Alleged Physical Abuse Alleged Insufficient information at this time Emergency Evacuation Verbal Abuse Alleged Fire Violation of client’s rights Bomb Breach of client’s confidential information Other Death Federal Notification Suicide Secret Service Homicide FBI Accident Other Accidental Overdose (resulting in death) Medical Event Medical Error Accidental Injury Illness, Age or Medical Reason Accidental Overdose (did not result in death) Please fax completed form to 860-638-5302, Attn: Dan Gerwien Updated 2/3/14 1 Mental Health Waiver Critical Incident Submission Form Medication Error/Reaction Firearms Medical Event- Other Hostage Drug Sale/Distribution/Possession Missing Client Missing, Risk to self or others Missing, no known risk Homicide/Manslaughter Serious Suicide Attempt Suicide Attempt by Active Participant Property Damage Property Damage Suicide Attempt within 30 days of Discharge from Mental Health Waiver Serious Crime Alleged Threats Physical Assault Threats to Agency Sexual Assault Threats to Person Risk of Injury to Minor Other Arson Other incident (please specify) Please check any substances that were present at the incident Alcohol Over-the-counter Medication Prescribed Medication No Evidence of substances being present Illicit Drug(s) If present, is there evidence that the incident may have been the result of substance overdose (alcohol, drug, etc.)? Yes No Please fax completed form to 860-638-5302, Attn: Dan Gerwien Updated 2/3/14 2 Mental Health Waiver Critical Incident Submission Form Is it likely that this incident will cause media coverage? Already Reported Not likely to be reported Likely or possible that it will be reported Individuals Involved in Incident Client Name Client Medicaid ID or SSN Client Date of Birth _ _/_ _/_ _ What was the client’s role in the incident? Victim Perpetrator Other (please specify) Is client involved currently enrolled on the MH Waiver? Yes, client is currently enrolled No, client unenrolled within the past 30 days Please describe the events of the incident, specifying individuals involved and why incident occurred Please fax completed form to 860-638-5302, Attn: Dan Gerwien Updated 2/3/14 3