Coarctation - Leeds Congenital Hearts
advertisement

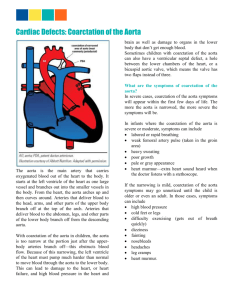
Coarctation Coarctation is a stenosis of the proximal descending aorta varying in anatomy, physiology and clinical presentation. Coarctation of the aorta is a relatively common defect that accounts for approx 5% of all congenital heart defects. Coarctation of the aorta may occur as an isolated defect or in association with various other lesions, most commonly bicuspid aortic valve and ventricular septal defect (VSD). It may be a feature of a congenital abnormality syndrome, particularly Turner’s syndrome. The coarctation may be discrete, or a long, tubular narrowing; the former is more common. The classic coarctation is located in the thoracic aorta distal to the origin of the left subclavian artery at about the level of the ductal structure (juxtaductal). The suprasternal notch echo window allows evaluation of the aortic arch to assess the transverse aortic arch, isthmus, and severity of coarctation. Doppler is used to measure the gradient at the site of coarctation and to identify the pattern of diastolic decay typically seen in patients with severe obstruction. Coarctations may be repaired surgically or they may be stented. The echo assessment of these patients is very similar to that of a newly diagnosed coarctation. If stented, it is often possible to visualise the proximal end of the stent. There may be 2D artefacts associated with the stent, therefore, stand alone CW Doppler is essential to assess the descending aortic velocity. Other imaging modalities may be useful in this patient population. 2D Echo / Colour Doppler Location of constriction, diameter in mm Aortic root, ascending aorta, transverse aorta and descending aortic dimensions Turbulence / acceleration on colour Doppler Left ventricular dimensions particularly wall thickness Presence of bicuspid aortic valve Presence/degree of aortic regurgitation Doppler Measurements Peak velocity across bicuspid aortic valve / ascending aorta. Peak velocity across the coarctation, noting the step-up at the site of the narrowing Presence of diastolic decay of coarctation jet envelope N.B. Stand alone Doppler is essential in obtaining the descending aortic signal Common Pitfalls/Limitations If the velocity in the ascending aorta is increased, it is important to apply the full Bernoulli equation to assess the severity of the coarctation. Full Bernoulli: 4(V22 – V12) The Doppler severity of the coarctation may be underestimated in patients with significant collateral vessels supplying the descending aorta. Repaired coarctations may be associated with aneurysm formation, this is difficult to exclude on echo, therefore, further imaging investigations may be indicated (e.g. MRI).