apprentice in speech language pathology (asl)
advertisement
")
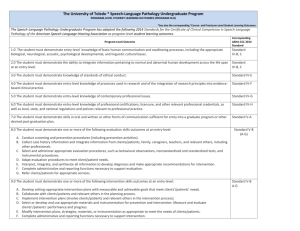
New Mexico Regulation and Licensing Department BOARDS AND COMMISSIONS DIVISION New Mexico Speech-Language Pathology, Audiology and Hearing Aid Dispensing Practices Board T on ey An a ya Bu i ld in g ▪ PO Box 251 01 ▪ Sa nt a Fe, N ew Mexi co 87505 ( 505) 476 -4640 ▪ Fax (505) 476 -4620 ▪ www.r ld .st at e.nm.u s APPRENTICE IN SPEECH LANGUAGE PATHOLOGY (ASL) 2015 ANNUAL RENEWAL Name Address City, State, Zip License # Initial License Date: NOTE: ALL RENEWALS MUST BE COMPLETED AND POSTMARKED NO LATER THAN August 30 OR A $75.00 LATE PENALTY FEE WILL BE ASSESSED. NO EXCEPTIONS!!!! In order to renew your Temporary Paraprofessional Apprentice License in Speech Language Pathology (ASL) and Pursuant to the Rules and Regulations you must meet the following requirements: IF YOU HAVE BEEN LICENSED 2 OR MORE YEARS AND HAVE PROVIDED DOCUMENTATION OF ACCEPTANCE INTO A MASTER’S DEGREE PROGAM PLEASE SUBMIT THE FOLLOWING DOCUMENTATION: (A temporary paraprofessional license may not be renewed if the licensee has not been accepted into a Master’s Degree program within two years of initial licensure.) $50.00 Renewal Fee Verification of Employment Form Verification of Education Form Course work completed in Communicative Disorders or other courses as outlined in the degree plan with minimum GPA of 3.0 Current Degree Plan Copy of transcripts from college or university Temporary paraprofessional licenses as an apprentice in speech-language is a terminal license and as such may be renewed no more than five times total. IF YOU HAVE BEEN LICENSED FOR LESS THAN 2 YEARS, AND HAVE NOT BEEN ACCEPTED INTO A MASTER'S DEGREE PROGRAM, SUBMIT EVIDENCE OF THE FOLLOWING: $50.00 Renewal Fee Verification Employment Form Verification of Education Form Transcript indicating enrollment and completion of nine semester hours of graduate courses with at least three hours in Communication Disorders. (Six may be in a related field.) CONTINUED ON BACK Revision date: 07/2010 New Mexico Speech -Language Pathology, Audiology and Hearing Aid Dispensing Practices Board ASL Renewal Please read and answer the following questions: 1. Are you in arrears in court-ordered child support in New Mexico? ____Yes ____No 2. Have you been convicted of a felony in the past 2 years? ____Yes ____No 3. Have you had any disciplinary action taken against you in any state? ____Yes ____No Applicant’s Signature___________________________________________________ Date___________ (Signature must be notarized) State of _________________________________________ County of_____________________________ Before me on this day personally appeared the above named applicant who being by me duly sworn upon oath says that all the acts, statements and answers contained in this application are true and correct. Sworn and subscribed to before me____________________________ on this _______ day of_____,20_____ ____________________________________ Notary Public SEAL My Commission Expires:______________ New Mexico Regulation and Licensing Department BOARDS AND COMMISSION DIVISION Page 2 of 5 Revision date: 03/2008 New Mexico Speech -Language Pathology, Audiology and Hearing Aid Dispensing Practices Board ASL Renewal VERIFICATION OF EMPLOYMENT AND SUPERVISION FOR TEMPORARY PARAPROFESSIONAL LICENSE AS AN APPRENTICE IN SPEECH-LANGUAGE (ASL) PART I - EMPLOYMENT AND SUPERVISION Name of Employer (school district or business): ______________________________________________ Address: _____________________________________________________________________________ City: _______________________ State: __________________ Zip: _________ Phone: ______________ Name of Worksite Assignment (if other than above): __________________________________________ Name of Speech-Language Pathology Supervisor: ____________________________________________ Beginning Date of Supervision: _________________ Ending Date of Supervision: __________________ I hereby certify that I am the SLP supervisor assigned to the applicant listed above and that I will be supervising this individual at all assigned worksites. My total supervision will be completed as follows: A minimum of 10% of contact time must be under direct supervision. A minimum of 10% of indirect contact time must be monitored. I acknowledge that I am aware I am legally responsible for the caseload assigned to the ASL. Supervisor’s Signature: _________________________________________ License # ______________ PART II - TO BE COMPLETED BY APPLICANT’S CURRENT EMPLOYER Name of Applicant: ______________________________________________ Date: _________________ Address: ____________________________ City: _______________ State: __________ Zip: _________ This is to verify that _________________________________________ is an employee in good standing. (Employee name) I confirm that the above named employee will engage in the following performance responsibilities. Check all that apply. Screen speech-language and/or hearing abilities; Conduct treatment programs and procedures that are planned, selected and/or designed by the Supervising Speech-Language Pathologist; Prepare written daily plans based on the overall intervention plan designed by the Supervising SpeechLanguage Pathologist; Record, chart, graph or otherwise display data relative to the client performance and report changes in performance to the supervising SLP; Maintain daily service delivery/treatment notes and complete daily charges as requested; Assist the Speech-Language Pathologist during assessment of clients, such as those who are difficult to test; Perform clerical duties (including maintenance of therapy/diagnostic materials, client files) as directed by the supervising SLP New Mexico Regulation and Licensing Department BOARDS AND COMMISSION DIVISION Page 3 of 5 Revision date: 03/2008 New Mexico Speech -Language Pathology, Audiology and Hearing Aid Dispensing Practices Board ASL Renewal Participate with the Speech-Language Pathologist in research projects, in-service training, and public relations programs. VERIFICATION OF EMPLOYMENT AND SUPERVISION continued I confirm that the above named employee shall NOT engage in the following: Administer diagnostic tests Interpret data into diagnostic statements or clinical management strategies or procedures Select or discharge cases Treat clients without following the individualized treatment plan Interpret clinical information including data or impressions relative to client performance Independent composition of clinical reports except for progress notes to be held in the client’s file Refer clients to other professionals or agencies Provide client or family counseling Develop or modify client's IEP/IFSP Clinical Report or Plan of Care in any way without the approval of the supervising SLP Disclose clinical or confidential information Sign any formal documents without the supervising SLP’s signature I confirm that provision for supervision will be provided for the above named employee. Furthermore, the supervisor will meet the following minimal requirements: At least two years of experience working as a Speech-Language Pathologist Hold a New Mexico occupational license as a Speech-Language Pathologist Provide a minimum of 10% direct and 10% indirect contact time with the above named employee The supervising Speech-Language Pathologist will be given a copy of this form. I recognize that it is the employer’s responsibility to be sure that the supervising SLP is provided a work schedule that will allow for the necessary supervision of the employee listed above. School District or Business: __________________________________________________________ PART III - SIGNATURES Signature of Supervisor: Title: Date: Signature of Employer: Title: Date: Signature of Applicant: Title: Date: New Mexico Regulation and Licensing Department BOARDS AND COMMISSION DIVISION Page 4 of 5 Revision date: 03/2008 New Mexico Speech -Language Pathology, Audiology and Hearing Aid Dispensing Practices Board ASL Renewal VERIFICATION OF EDUCATION FOR TEMPORARY PARAPROFESSIONAL LICENSE AS AN APPRENTICE IN SPEECH-LANGUAGE To be completed by program director in the college in which the applicant is currently enrolled. Name of Applicant: ________________________________________ Date: ________________ Address: ______________________________________________________________________ City: ________________________ State: _____________ Zip: _________ Phone: I _____________________________ am requesting the release of the following information: Applicant Name Check one of the following: Enrolled in a Master’s Degree program in Speech-Language Pathology or Communication Disorders and completes a minimum of 9 semester hours per year of graduate courses in Communication Disorders. (Specify university and attach copy of degree plan) OR Enrolled in and completes 9 semester hours of graduate courses per year with at least 3 hours in Communication Disorders, 6 hours may be taken in a related field. (Specify university) Indicate dates nine (9) hours of coursework will be or have been completed: Has applicant met the GPA requirement of 3.0? Yes No Acceptance into a Master’s Degree program must take place within two years of initial license. Program Director’s Name (Print) Program Director’s Signature Date New Mexico Regulation and Licensing Department BOARDS AND COMMISSION DIVISION Page 5 of 5 Revision date: 03/2008