speech-language checklist for preschool children
advertisement

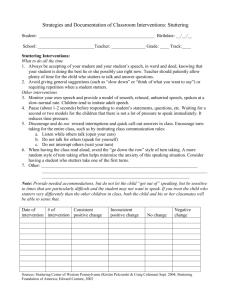
SPEECH-LANGUAGE IMPAIRED CHECKLIST For Preschool Children Date: ___________________ Child’s Name: ________________________________________________ Age:__ Person completing this form: ___________________________________ Relationship to Child: __________________________________________ Primary Language spoken by child: _____________________________________ LANGUAGE Does this child’s use and understanding of spoken language seem typical for his/her age? yes no Does this child ask/answer questions like other same age children? yes no Does this child use appropriate sentence length/structures? yes no Is this child able to follow simple directions during classroom activities? yes no Does this child carry on short conversations typical for his age? yes no Does this child listen/respond to stories read in a small group or at home? yes no Does this child’s ability to understand/use language make it difficult for him/her to participate fully in classroom activities? yes no No Concerns regarding language. ARTICULATION Check if the child is able to produce the following sounds: p m n k g f w b h Do teachers/classmates have difficulty understanding his/her speech? yes no Does this child’s speech make it difficult for him/her to fully participate during oral classroom activities? yes no Does this child’s speech make it difficult for him/her to play with or socially interact with classmates? yes no No Concerns regarding articulation. STUTTERING Does this child often repeat syllables, words or phrases more than other children his/her age? yes no Does this child demonstrate the following physical behaviors? Eye blinking facial grimacing foot tapping Does this child often seem to have difficulty getting words out? yes no Does this child’s stuttering make it difficult for him/her to talk to teachers and/or classmates? yes no Does this child seem to avoid speaking at school during some activities? yes no No Concerns regarding stuttering. VOICE Does this child’s voice sound unusual for his/her age? yes Has this child seen a physician because of his/her voice? yes Does this child’s voice make it difficult for him/her to interact with teachers or classmates? yes Does this child’s voice make it difficult for him/her to participate in oral classroom activities? yes PRAGMATIC LANGUAGE Does this child use appropriate eye contact? Does this child understand changes in tone of voice? Does this child understand changes in facial expressions? Does this child use a variety of facial expressions? Does he/she use greetings (say “hello”, “goodbye”)? Does he/she use verbal courtesies (please, thank you, excuse me)? Does he/she interact with other children? Does this child flap his hands when he/she is excited? yes yes yes yes yes yes yes yes no no no no no no no no no no no no Does this child demonstrate any of the following behaviors? Check all that apply: Frequently walks on his/her toes Lines up toys No fear of danger Produces jargon/speaks his/her own language “Echoes” or repeats exactly what he hears others say Flap his/her hands when he/she is excited/upset ADDITIONAL COMMENTS ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ PLEASE RETURN FORM TO: ___________________________________________