Health Information Questionnaire - Patient Medical History
advertisement

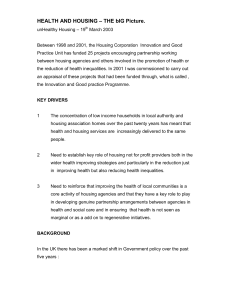
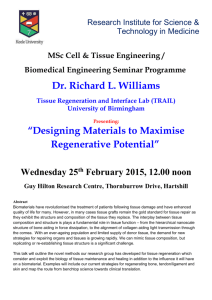
Page 1 of 2 HEALTH INFORMATION QUESTIONNAIRE PATIENT NAME ________________________________________________ AGE ________ DOB _______/_______/_______ INSURANCE CARRIER ________________________________________________ SSN # ________---________---________ ADDRESS __________________________________________ CITY/ST ___________________________ ZIP ____________ HOME PHONE ______________________________________ CELL PHONE _______________________________________ EMAIL ________________________________________________________________________________________________ CAN WE CONTACT YOU VIA (CIRCLE) MAIL PHONE EMAIL TEXT EMERGENCY CONTACT ____________________________ PHONE ________________RELATIONSHIP _______________ HOW DID YOU HEAR ABOUT REGENERATION?_____________________________________________________________ Have you ever had any of the following conditions? (check all that apply) AIDS Anemia Arthritis Auto Immune Deficiency Asthma Blood Disease Blood Transfusion Chemotherapy (active) Have you ever had Diabetes Dizziness Epilepsy Fainting Hay Fever Heart Disease Hepatitis High Blood Pressure Infection Kidney Disease Liver Disease Lupus Melanoma Mental Disorder Nervous Disorder Radiation Therapy Previous Cosmetic Facial treatments? Respiratory Problems Sinus Problems Stroke Thyroid Problems Tuberculosis Ulcers Venereal Disease Other – Please Explain _______________________ Have you ever had (check all that apply) Atopic Dermatitis Psoriasis Rosacea Seborrheic Dermatitis Botox Collagen Fillers Chemical Peel Waxing Date _________________ Date _________________ Date _________________ Date _________________ Cold Sores or Fever Blisters Frequency: <1 per year 1 – 3 per year 4+ per year Viitiligo Other skin conditions Please explain ___________________ Facial Surgery Laser Surgery Microdermabrasion Other – Please Explain ____________________ Date _________________ Date _________________ Date _________________ Date _________________ Other Regeneration, P.C. Office 402-483-0431 Fax 402-483-9905 Are you Pregnant? Yes No Due Date: _______________________ Are you Lactating? Yes No Do you Tan? Yes No Last Tanning Session ______________ Do you scar abnormally? Yes No www.regenerationpc.com Page 2 of 2 Are you currently using: Do you have allergies to: Rentin-A, Renova, Retinoic Acid Products Prescription Acne Medication Birth Controls Pills / Patch Hormone Replacement Accutane Past Accutane Use _______________________ Medications Cosmetics Latex/Other List current medications/supplements that you are taking _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ List any questions that you have _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Regeneration, P.C. Office 402-483-0431 Fax 402-483-9905 www.regenerationpc.com