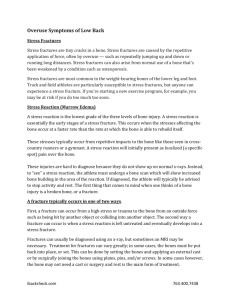
Stress Fractures About the Tibia, Foot, and Ankle
advertisement

Stress Fractures About the Tibia, Foot, and Ankle 1. Michael K. Shindle, MD, 2. Yoshimi Endo, MD, 3. Russell F. Warren, MD, 4. Joseph M. Lane, MD, 5. David L. Helfet, MD, 6. Elliott N. Schwartz, MD and 7. Scott J. Ellis, MD From the Summit Medical Group, Morristown, NJ (Dr. Shindle), the Department of Radiology and Imaging (Dr. Endo), the Department of Orthopedic Surgery (Dr. Warren and Dr. Ellis), and the Orthopedic Trauma Service (Dr. Lane and Dr. Helfet), Hospital for Special Surgery, New York, NY, and the Northern California Institute for Bone Health (Dr. Schwartz), Oakland, CA. Dr. Warren or an immediate family member has received royalties from Biomet and Smith & Nephew and has stock or stock options held in Cayenne, OrthoNet, and ReGen Biologics. Dr. Lane or an immediate family member is a member of a speakers’ bureau or has made paid presentations on behalf of Eli Lilly, Harvest Technologies, Novartis, and Weber Chilcott; serves as a paid consultant to Amgen, CollPlant, Bone Therapeutics SA, BioMimetic, DFine, Graftys, and Zimmer; has received research or institutional support from Amgen; and serves as a board member, owner, officer, or committee member of the Orthopaedic Research Society, the Musculoskeletal Tumor Society, the American Academy of Orthopaedic Surgeons, the Association of Bone and Joint Surgeons, and the American Society for Bone and Mineral Research. Dr. Helfet or an immediate family member has stock or stock options held in OHK Medical Devices and FxDEVICES. Dr. Schwartz or an immediate family member is a member of a speakers’ bureau or has made paid presentations on behalf of Amgen, Eli Lilly, and Novartis and has received research or institutional support from Amgen, Eli Lilly, and Merck. None of the following authors or any immediate family member has received anything of value from or owns stock in a commercial company or institution related directly or indirectly to the subject of this article: Dr. Shindle, Dr. Endo, and Dr. Ellis. Next Section Abstract In competitive athletes, stress fractures of the tibia, foot, and ankle are common and lead to considerable delay in return to play. Factors such as bone vascularity, training regimen, and equipment can increase the risk of stress fracture. Management is based on the fracture site. In some athletes, metabolic workup and medication are warranted. High-risk fractures, including those of the anterior tibial diaphysis, navicular, proximal fifth metatarsal, and medial malleolus, present management challenges and may require surgery, especially in high-level athletes who need to return to play quickly. Noninvasive treatment modalities such as pulsed ultrasound and extracorporeal shock wave therapy may have some benefit but require additional research. Previous SectionNext Section Risk Factors A dynamic balance exists between the accumulation of microdamage and the host bone’s repair processes. Intrinsic and/or extrinsic factors that disrupt this balance can increase the risk of stress fracture. Intrinsic factors include metabolic state, menstrual patterns, level of fitness, muscle endurance, anatomic alignment, microscopic bone structure, and bone vascularity. Extrinsic factors include training regimen, dietary habits, and equipment (eg, footwear, playing surface). Stress fractures commonly occur in poorly vascularized areas of bone. Bone in relative watershed areas lacks the ability to respond to stress and heal. This is particularly true of highrisk stress fractures (ie, fractures of the navicular, fifth metatarsal, and anterior tibia). Poor blood supply combined with high stress makes management of fractures in these areas challenging and can delay an athlete’s return to play.1,2 Previous SectionNext Section Diagnosis Several history and physical examination findings are found in all types of stress fractures. Typically, patients have an insidious onset of pain over a 2- to 3-week period. Onset of pain often correlates with a recent change in training habits or equipment. A thorough history should be obtained for all patients; medical history should include questions regarding known endocrinopathies (eg, diabetes mellitus), autoimmune and eating disorders, depression, malabsorption syndromes, bariatric surgery, and gastroesophageal reflux disease. Dietary history should include questions regarding the intake of calcium, vitamin D, protein, and alcoholic and caffeinated beverages. A medication history is helpful for detecting secondary causes of stress fractures. In the physical examination, the hallmark of a stress fracture is tenderness over the affected bone. Percussion of the bone away from the site of the fracture may produce pain. Functional testing such as hopping on one foot may also elicit pain. Previous SectionNext Section Imaging Plain radiography is the most useful imaging modality for initial radiographic assessment of stress fractures of the lower extremity. It is readily available, is inexpensive, and may preclude the need for additional imaging if the radiographic features are consistent with a stress fracture. Radiographic appearance of the fracture is affected by whether cortical or cancellous bone is involved and the acuity of the injury. In stress fractures that involve cortical bone such as that found in the metatarsal shaft, the earliest radiographic findings may include a subtle radiolucency or poor definition of the cortex.3 Later findings include thickening and sclerosis of the endosteum and periosteal new bone formation, which may take weeks to months to form after the onset of symptoms.4 Stress fractures that involve cancellous bone (eg, calcaneus) appear as a band of sclerosis characteristically oriented perpendicular to the trabeculae4 (Figure 1). Typically, radiographic findings lag behind clinical symptoms by weeks and may not appear at all if activity has been modified.4 When a stress fracture is suspected and initial radiographs are nondiagnostic, repeat radiographs obtained 2 weeks after initial imaging may reveal the fracture.4 If urgent diagnosis is needed, bone scan and MRI are often helpful. Bone scan is particularly useful for identifying potential areas of pathology in patients with noncontiguous, simultaneous fractures (eg, fractures of the second metatarsal and midshaft of the tibia). Technetium-99m–labeled diphosphonate bone scan is very sensitive and aids in early detection of stress fractures; this scan is a valuable diagnostic tool when initial radiographs are negative. Stress fractures are visible on bone scans days to weeks earlier than on radiographs5 (Figure 2). Although bone scan has a high degree of sensitivity, it is not always specific. Focal tracer uptake can be the result of any process that remodels bone (eg, tumor, infection, stress reaction without fracture). MRI has become indispensable for evaluation of radiographically occult stress fractures. This modality allows evaluation of the soft tissues and provides greater anatomic detail than does plain radiography. Fluid-sensitive sequences (eg, short-tau inversion recovery, fat-saturated T2weighted sequences) are highly sensitive for endosteal marrow edema and periosteal edema, which are typically the earliest features of stress fractures6 (Figure 3). Muscle edema, cortical thickening, and a hypointense fracture line through the cortex or medullary cavity are also visible on MRI. It is considered to be at least as sensitive as and more specific than bone scan for detection of stress fractures.7 Ultrasonography can be sensitive in identifying radiographically occult stress fractures in relatively superficial bones such as the metatarsals.8 Although the ultrasound beam cannot penetrate the cortex to facilitate evaluation of the endosteum or marrow below, ultrasonography can be used to evaluate the outer surface of the cortex for step-off, a hypoechoic band, periosteal reaction, and hyperechoic callus formation.8,9 Benefits of this modality include the absence of ionizing radiation as well as the ability to perform a focused, real-time evaluation of the fracture. Localized tenderness with transducer pressure at the injury site is an important ancillary finding. Doppler can be used to identify hypervascularity and increase the diagnostic accuracy as well as better define the acuity of ultrasonography (Figure 4). CT is rarely indicated for initial evaluation of suspected stress fractures because it has a higher radiation dose than conventional radiography and low sensitivity compared with MRI.10 However, CT can be useful when a more accurate evaluation of the osseous anatomy is needed. For example, when MRI is equivocal, the exquisite bony detail provided by CT allows differentiation of complete versus incomplete fracture. CT may be used to identify a subtle fracture line not seen on other modalities. Fracture complications such as nonunion may be better visualized on CT, especially if susceptibility artifact from adjacent hardware limits MRI evaluation. Some authors advocate using a CT classification to guide management of certain types of stress fractures, particularly navicular fractures.10 Previous SectionNext Section Nonsurgical Management In general, management of stress fractures includes rest and immobilization. It is useful to classify fractures as low risk or high risk to help determine the appropriate nonsurgical or surgical management. At our institution, patients with stress fractures have a consultation with a metabolic bone disease specialist, who evaluates the need for serum and urine testing based on a thorough history and physical examination. A complete metabolic panel, including serum calcium, albumin, alkaline phosphatase, and serum vitamin D levels, as well as a calculated glomerular filtration rate, is ordered for all patients. Hormonal levels are assessed if the patient has a history of amenorrhea, oligomenorrhea, sexual dysfunction, or certain endocrinopathies (eg, hyperthyroidism, hyperparathryoidsim). In addition, bone densitometry is ordered for patients with a history of multiple stress fractures or the female athletic triad (ie, eating disorder, osteoporosis, amenorrhea). If an eating disorder is discovered, a multidisciplinary approach to treatment is indicated.11 Medication A slow healing process may interrupt participation in sports for a relatively long period of time. In addition, nonsurgical treatment may result in delayed union or nonunion. In certain circumstances, surgical management is indicated to promote union, thereby allowing a quicker return to weight-bearing activity. However, inherent limitations in the ability of some fractures to heal have sparked an interest in developing effective pharmacologic interventions to either prevent stress fractures or accelerate recovery. If laboratory workup reveals low levels of calcium, vitamin D, or phosphorus, underlying causes should be investigated and, at a minimum, a strict regimen of supplementation should be instituted. The recommended daily allowances of calcium and vitamin D are 1,000 mg and 800 to 1,000 IU, respectively.12 However, debate exists regarding whether this amount is too low for athletes. At our institution, we recommend 1,200 to 1,500 mg/d of calcium and 800 to 3,000 IU/d of vitamin D. A variety of medications that has been used to manage osteoporosis and osteopenia has also been used to manage stress fractures. Diphosphonates prevent osteoclast-mediated bone resorption and thus may prevent the initial bone loss observed in the remodeling response to high bone strain, potentially preventing stress fracture.13 Stewart el al14 treated five collegiatelevel athletes with intravenous pamidronate weekly for 5 weeks. Four of five athletes were able to continue training and compete within 1 week of therapy. The remaining patient missed only 3 weeks of training, which suggests that pamidronate may be useful when used as an adjuvant therapy. Another study evaluated the prophylactic use of risedronate in a high-risk military population.15 There was no statistically significant difference between the treatment and placebo groups with regard to the total stress fracture incidence. Until the results of well-designed clinical trials become available, it is prudent to limit use of diphosphonates for management of stress fractures. The risks and benefits of any prescribed medication must be considered. Diphosphonates should not be used in patients of childbearing age. Teriparatide (Forteo, Eli Lilly, Indianapolis, IN) is a 1-34 amino acid moiety of the N-terminal portion of the 1-84 amino acid parathyroid molecule and is produced by recombinant DNA technology. Like the full parathyroid molecule, bursts of teriparatide are anabolic to bone and result in additional osteoblast formation from precursor stem cells, which results in earlier and increased formation of callus, thereby improving fracture healing. This effect has been reported in numerous preclinical studies.16-19 These data have led to the use of teriparatide in numerous anecdotal situations and in patients with acute traumatic, osteoporotic, and stress fractures and delayed fracture healing or nonunion. Forteo has been approved by the FDA for treatment of osteoporosis in women with a high risk of fracture. It is used off label to increase bone mass in men who are at high risk of fracture (ie, those with osteoporosis, those taking glucocorticoids). In addition, one must be cognizant of the contraindications and warnings associated with this drug; Forteo has a black box warning because its use was associated with osteosarcoma in a rat model.18 Further research is needed to determine the effect of teriparatide on fracture healing in humans. The use of anabolic agents (eg, anti-sclerostin antibody) for fracture prevention and acute fracture healing requires additional research, as well. It is likely that over the next 5 to 10 years, the role of platelet-rich plasma, mesenchymal stem cells, bone morphogenetic proteins, and other modalities will be further clarified. Pulsed Ultrasound Use of other modalities such as pulsed ultrasound has been proposed for management of stress fractures. Although the exact mechanism remains unknown, pulsed ultrasound is thought to induce aggrecan and proteoglycan synthesis in chondrocytes, leading to increased endochondral ossification.20 In a recent prospective, randomized, double-blind study, 43 tibial stress fractures were randomized to treatment with either placebo or pulsed ultrasound. There was no significant reduction in healing time between the two groups. However, other studies have shown that pulsed ultrasound may decrease the time to clinical healing; therefore, additional studies are warranted.21 Extracorporeal Shock Wave Therapy Extracorporeal shock wave therapy (ESWT), another noninvasive technique, has proved to be effective for fracture healing and management of delayed union and nonunion in an animal model.22 ESWT is thought to induce periosteal detachment and microfractures of the trabeculae, which in turn can stimulate fracture healing.23 Taki et al23 reported on five athletes with recalcitrant stress fractures treated with ESWT and suggested that it is an effective treatment method for intractable stress fractures in athletes. Additional basic science and clinical studies are necessary to determine the effectiveness of ESWT as well as optimal energy density levels and impulse rates. Previous SectionNext Section Management of Specific High-Risk Stress Fractures Anterior Tibial Diaphysis Anterior tibial (ie, so-called dreaded black line) stress fractures are less common but more concerning than posteromedial tibial stress fractures. Radiographic findings associated with stress fracture of the anterior tibia include a thickened anterior cortex with a lucent line in the anterior midshaft of the tibia (Figure 5). Management of this fracture is challenging, especially in the high-performance athlete. Constant tension from posterior muscle forces and poor vascularity may predispose to delayed union and nonunion and even complete fracture. Beals and Cook24 reported poor results with nonsurgical management of stress fractures of the anterior tibial diaphysis. Five of eight patients with these fractures who were allowed full activity went on to complete fracture. Only 8 of 20 patients (40%) treated with rest alone were able to return to full activity after an average of 4.4 months. Batt et al25 treated four delayed-union stress fractures of the anterior midshaft of the tibia with bracing and modified rest; the mean time to return to full activity was 12 months. Such long periods of convalescence may end a professional athlete’s career. Other authors have reported better success with nonsurgical management of these fractures. Rettig et al26 reported that seven of eight basketball players with anterior stress fractures achieved union with rest and electrical stimulation. Mean treatment time was 8.7 months. The players returned to sport at a mean of 12.5 months. Intramedullary (IM) nailing of chronic anterior tibial stress fractures is effective in many cases, but it does not uniformly lead to healing.27 The pain relief promoted by the nail may allow return to sport before complete bone healing. Borens et al28 used an anterior tension band plating technique to treat four high-performance female athletes with anterior tibial stress fractures. Compression plating of the anterolateral aspect of the tibia was done with a 3.5-mm 6-hole locking compression plate (Figure 6). All four patients underwent bone grafting with demineralized bone matrix. Immediately postoperatively, patients began range-of-motion exercises for the knee and ankle as well as isometric exercises without resistance. Physical therapy was initiated, with weight bearing of the affected extremity limited to 20 lbs for 8 weeks, followed by progression to full weight bearing and return to sport as tolerated over the next 2 to 4 weeks. All four athletes returned to full activity at a mean of 10 weeks. The authors postulated that anterior tension band plating may be superior to IM nailing because (1) biomechanically, a plate that is placed at a distance from the central axis of the bone has a mechanical advantage over an IM device in neutralizing tensile forces and fracture micromotion, (2) an anterior plate has the added advantage of being ideally placed to resist the tensile forces that lead to anterior stress fractures, and (3) plating avoids disruption of the knee extensor mechanism and the anterior knee pain frequently associated with IM nailing of the tibia.29 Navicular The navicular is susceptible to stress fracture based on specific vascular and biomechanical properties. The central one third of the navicular body has been identified as a zone of maximum shear stress.30 During the foot-strike phase of running, and especially in the equinus foot, compression forces are generated from distal to proximal across the medial and lateral aspects of the navicular via the first and second metatarsocuneiform joints. The talar head resists the forces across the first metatarsal and medial cuneiform, whereas forces across the second metatarsal and middle cuneiform are not resisted. Because of these forces, the navicular experiences a zone of maximal shear stress just lateral to the center of the talar head in the talonavicular articulation. In addition, the central zone of the navicular body is devoid of a direct blood supply and has difficulty healing30 (Figure 7). Often, there is a considerable delay in the diagnosis of navicular fracture; therefore, a high index of suspicion should be maintained for this stress fracture in the athlete with foot pain (Figure 8). Physical examination may reveal focal dorsal pain over the midportion of the navicular, which is also referred to as the N spot.31,32 Management of navicular stress fractures continues to evolve. These fractures can heal without surgery; however, such healing comes at the cost of prolonged immobilization and limitation of activity. These fractures are high risk; therefore, aggressive management is necessary. Nonsurgical management should include use of a nonweight-bearing cast until the fracture has healed. Torg et al33 performed a systematic review of nonsurgical and surgical management of tarsal navicular stress fractures and concluded that nonsurgical non-weight–bearing management is the standard of care for initial treatment of both partial and complete stress fractures of the tarsal navicular. In a separate study, Torg et al34 reported a 100% success rate in 10 patients treated with non-weight–bearing cast immobilization for 6 to 8 weeks, with an average return to activity at 3.8 months. In a study of 82 patients with navicular stress fractures managed nonsurgically, Khan et al32 reported that 19 of 22 patients (86%) treated for 6 weeks in a non-weight–bearing cast returned to full activity at an average of 5.6 months postinjury. Only 9 of 13 patients (69%) managed with casting for a shorter duration (ie, 2 to 5 weeks) returned to full activity. In five patients with no activity restrictions, only one returned to full activity. This study demonstrates the importance of strict non-weight–bearing restrictions with casting for a minimum of 6 weeks. Surgical management of navicular stress fractures includes screw fixation with or without exposure of the fracture site (Figure 9). Elite athletes with type I navicular stress fractures may choose to undergo percutaneous screw fixation to return to competition quickly and to reduce the risk of recurrent stress fracture. At our institution, the preferred technique is to expose the fracture site and use compression screw fixation with two screws placed such that the threads gain as much purchase in the larger fragment of bone as possible, which usually entails placing the screws from lateral to medial. However, screw placement depends on the exact location of the fracture. Partially threaded cannulated screws are the easiest to place and can deliver compression but are weaker than solid screws. Postoperative rehabilitation includes non-weight– bearing ambulation with a removable walking cast for 4 weeks, partial weight bearing for 2 weeks, and gradual return to activity at 8 weeks. Some authors recommend repeat imaging to confirm healing before permitting return to full sporting activities.30 Proximal Fifth Metatarsal Stress fracture of the proximal fifth metatarsal typically occurs just distal to the metaphysealdiaphyseal junction of the fifth metatarsal (Figure 10). These fractures are common in basketball, football, and soccer players, and are considered high risk because of the high incidence of nonunion due to poor blood supply. We suggest nonsurgical management with strict non-weight– bearing ambulation in a short leg cast for 6 to 8 weeks. Because of the high incidence of delayed union and nonunion, surgeons may consider more aggressive management of these fractures. If the patient is an elite-level athlete, has persistent unresolved pain, or develops an established pseudarthrosis, then surgical intervention is indicated. Torg et al35 reported on 15 acute fractures of the base of the fifth metatarsal treated with protected weight bearing and cast immobilization; 93% healed at an average of 6.5 weeks. One patient had a nonunion that required surgery. The authors concluded that non-weight– bearing and cast immobilization for 6 to 8 weeks is successful in patients in which IM sclerosis is not present on radiographs. However, surgical intervention should be considered in patients with radiographic evidence of IM sclerosis that partially obliterates the medullary cavity or in patients who engage in high-level athletic activity. Clapper et al36 reported on 100 acute fractures divided into three groups: avulsion fractures, which were treated with a hard-soled shoe or walking cast with weight bearing as tolerated; proximal stress fractures, which were treated with a nonweight–bearing cast for 8 weeks and then progressive weight bearing in a walking cast; and (3) shaft or neck fractures, which were treated with a short-leg walking cast and weight bearing as tolerated. The cast was removed 4 weeks postinjury; if symptoms persisted, the cast was reapplied and worn for an additional 2 to 4 weeks. Twenty-five patients had proximal stress fractures of the fifth metatarsal. In this group, union occurred in only 18 patients (72%), and 7 had clinical and radiographic evidence of nonunion 25 weeks after injury. These patients underwent IM screw fixation and had a union rate of 100% at an average of 12.1 weeks. Goals of early surgical management are to minimize the risk of nonunion and refracture and to decrease the time to return to sport. Foot anatomy must be taken into consideration, and additional procedures, such as lateralizing calcaneal osteotomy for a cavovarus foot, should be considered. At our institution, internal fixation with a solid stainless steel IM screw has become the procedure of choice (Figure 10, B). The patient is kept non-weight–bearing for 3 weeks; then partial weight bearing is allowed with a removable boot, and stationary bicycle and pool therapy is begun. Transition to full weight bearing begins at 5 weeks. In general, return to activity is allowed 2 months after surgery, depending on the resolution of pain and radiographic evidence of healing. Porter et al37 reported on 23 consecutive athletes treated with fixation using a 4.5-mm cannulated screw; all athletes returned to sport at an average of 7.5 weeks. Great Toe Sesamoids Stress fractures of the great toe sesamoids are not uncommon in athletes, particularly football players, runners, golfers, and gymnasts. The medial sesamoid bone is more likely to develop a stress fracture because it is larger than the lateral sesamoid and lies directly under the head of the first metatarsal. Repeated dorsiflexion of the great toe during running and jumping can result in tensile forces on the sesamoid sufficient to cause a transverse stress fracture. Patients typically present with pain on palpation of the plantar aspect of the sesamoid bones as well as pain with dorsiflexion of the metatarsophalangeal joint of the great toe. Plain radiographs, particularly AP and sesamoid views, may be helpful, and MRI can be used to identify areas of edema or necrosis (Figure 11). Stress fracture of the sesamoid must be differentiated from bipartite sesamoid. In the general population, the reported incidence of bipartite sesamoid ranges from 5% to 30%, and the incidence of bilaterality is approximately 80%.38,39 Bipartite sesamoid occurs more commonly in the medial sesamoid, and radiographs typically reveal a sesamoid with smooth margins. Radiographically, a stress fracture can be differentiated from a bipartite sesamoid by the presence of a transverse fracture line with jagged margins. Nuclear imaging can be useful to help differentiate acute or stress fractures from a bipartite sesamoid. Nonsurgical management is the standard of care and should include a non-weight–bearing cast that extends to the distal tip of the toe to prevent dorsiflexion. After initial casting, an orthosis with a dancer’s pad or a stiff-soled running shoe with a built-in metatarsal bar may be used. Other conditions may place additional force on the sesamoids (eg, plantar flexed first ray, isolated gastrocnemius contracture, pes cavus alignment; these should be considered in the treatment plan. Early surgical intervention may be required for stress fractures in the sesamoids of the great toe because of the high incidence of delayed union, nonunion, or refracture associated with these fractures. Surgery may consist of bone grafting, cast immobilization, and open reduction and internal fixation, or excision of the offending sesamoid bone and reconstruction of the flexor hallucis brevis and intersesamoid ligament. Medial Malleolus Stress fractures of the medial malleolus are relatively uncommon. They can occur during running and jumping activities. Etiology of these stress fractures may be secondary to repetitive impingement of the talus on the medial malleolus during ankle dorsiflexion and tibial rotation.40 In patients with negative plain radiographs and evidence of incomplete fracture line on advanced imaging such as MRI, treatment is individualized based on the patient’s prior level of activity (Figure 12). Most patients can be treated successfully with activity modification and cast immobilization or ankle bracing. However, nonunion has been reported with high shear forces exerted at the fracture site.40 We recommend internal fixation with two 4.0-mm cancellous screws or a plate in patients with a complete fracture line visible on radiographs or in patients with nonunion. Bone grafting should be considered for management of nonunion. Previous SectionNext Section Summary Stress fractures most commonly occur in the tibia, foot, and ankle and may result in considerable delay in return to play. Many factors can affect these injuries, including metabolic state, blood supply, training regimen, and foot anatomy (eg, varus or valgus hindfoot, plantar flexed first ray). The location of the injury can help in predicting the rate of healing and dictating treatment. Nonsurgical management of these fractures with medication such as teriparatide and other anabolic agents (eg, anti-sclerostin antibody) is promising, but further research is warranted. Additional research is also needed on other nonsurgical treatment options, including pulsed ultrasound and ESWT. In general, good results have been reported with weight-bearing restrictions and cast immobilization; however, surgical intervention may be required to manage high-risk stress fractures in athletes who must return to sport quickly. Previous SectionNext Section Figures View larger version: In this page In a new window Figure 1 Lateral radiograph of the foot demonstrating a stress fracture of the calcaneus. The arrow marks a linear band of sclerosis perpendicular to the trabeculae. View larger version: In this page In a new window Figure 2 Technetium-99m-methylene diphosphonate bone scan of anterior tibias demonstrating focal tracer uptake in the lateral aspect of the midshaft of the right tibia, which is consistent with a stress fracture. View larger version: In this page In a new window Figure 3 Axial short-tau inversion recovery magnetic resonance image through the midshaft of the tibia demonstrating endosteal marrow edema (arrow) and periosteal edema (arrowhead) associated with a tibial stress fracture. View larger version: In this page In a new window Figure 4 Ultrasound with power Doppler of the dorsum of the second metatarsal bone demonstrating callus formation along the metatarsal diaphysis, with associated hyperemia consistent with a healing stress fracture. View larger version: In this page In a new window Figure 5 Plain AP (A) and lateral (B) radiographs of the tibia and fibula in a 23-year-old female professional basketball player with an anterior tibial stress fracture. The fracture is not visible on the AP radiograph, but the black line (arrow) that represents an anterior tibial stress fracture can be seen on the lateral radiograph. C, Magnification of the lateral radiograph demonstrating the black line (arrow). View larger version: In this page In a new window Figure 6 Management of an anterior tibial stress fracture with compression plating. A, The preoperative plan outlines patient position, exposure, and equipment to be used. B, Intraoperative photograph demonstrating the stress fracture following débridement. AP (C) and lateral (D) intraoperative fluoroscopic images demonstrating the position and appearance of the plate. Postoperative AP (E) and lateral (F) radiographs demonstrating a healed tibial stress fracture at 8 weeks. View larger version: In this page In a new window Figure 7 Multiplanar reformatted axial CT scan of the foot demonstrating subchondral sclerosis along the proximal articular surface of the navicular with a central linear fracture line and lucent cavity (arrow) in the cancellous bone that is consistent with a chronic stress fracture. View larger version: In this page In a new window Figure 8 Coronal fast spin-echo magnetic resonance image demonstrating a navicular fracture (arrow). View larger version: In this page In a new window Figure 9 Intraoperative AP fluoroscopic image demonstrating medial to lateral placement of two 4.0-mm cannulated screws. Stronger, solid screws can also be used for compression fixation. Compression can be obtained using partially threaded screws or by overdrilling the medial fragment. View larger version: In this page In a new window Figure 10 A, Preoperative AP radiograph of the foot demonstrating a stress fracture of the fifth metatarsal base in a 20-year-old collegiate soccer player. The fracture is located just distal to the fourth and fifth metatarsal articulation. The large degree of sclerosis is suggestive of the chronic nature of the fracture. B, Postoperative AP radiograph of the foot obtained 2.5 months after fixation of the fracture. A solid, partially threaded screw was used to bypass and compress the fracture site. Healing is observed on all sides of the fracture. View larger version: In this page In a new window Figure 11 A, Coronal short-tau inversion recovery magnetic resonance image of the foot demonstrating marrow edema within the lateral hallux sesamoid (arrow). B, Sagittal proton density sequence demonstrating a hypointense signal within the lateral hallux sesamoid with a central linear signal that represents a fracture (arrow). C, Sesamoid radiograph demonstrating sclerosis of the lateral sesamoid and the irregular contour of the plantar surface (arrow) secondary to a chronic stress fracture. View larger version: In this page In a new window Figure 12 Axial (A) and coronal (B) proton density sequences of the ankle demonstrating linear hypointense focus (arrows) in the anterior medial malleolus that represents a stress fracture that extends to the tibiotalar articular surface. (Courtesy of Carolyn M. Sofka, MD, New York, NY.) Previous Section References 1. Evidence-based Medicine: Levels of evidence are listed in the table of contents. In this article, references 6, 15, 17-20, and 22 are level I studies. References 5, 7, and 8 are level III studies. References 10, 14, 23-29, 32-37, and 40 are level IV studies. References 1-4, 9, 11-13, 16, 30, 31, 38, and 39 are level V expert opinion.References printed in bold type are those published within the past 5 years. 2. 1.↵ 1. Boden BP, 2. Osbahr DC BodenBP, OsbahrDC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8(6):344-353.pmid:11104398 Abstract/FREE Full Text 3. 2. 1. Anderson RB, 2. Hunt KJ, 3. McCormick JJ AndersonRB, HuntKJ, McCormickJJ: Management of common sports-related injuries about the foot and ankle. J Am Acad Orthop Surg 2010;18(9):546556.pmid:20810936 Abstract/FREE Full Text 4. 3.↵ 1. Daffner RH, 2. Pavlov H DaffnerRH, PavlovH: Stress fractures: Current concepts. AJR Am J Roentgenol 1992; 159(2):245-252.pmid:1632335 Abstract/FREE Full Text 5. 4.↵ 1. Sofka CM SofkaCM: Imaging of stress fractures. Clin Sports Med 2006;25(1):53-62, viii.pmid:16324973 CrossRefMedlineWeb of Science 6. 5.↵ 1. Roub LW, 2. Gumerman LW, 3. Hanley EN Jr, 4. Clark MW, 5. Goodman M, 6. Herbert DL RoubLW, GumermanLW, HanleyEN Jr, ClarkMW, GoodmanM, HerbertDL: Bone stress: A radionuclide imaging perspective. Radiology 1979;132(2):431-438.pmid:461804 Abstract/FREE Full Text 7. 6.↵ 1. Kiuru MJ, 2. Niva M, 3. Reponen A, 4. Pihlajamäki HK KiuruMJ, NivaM, ReponenA, PihlajamäkiHK: Bone stress injuries in asymptomatic elite recruits: A clinical and magnetic resonance imaging study. Am J Sports Med 2005;33(2):272-276.pmid:15701614 Abstract/FREE Full Text 8. 7.↵ 1. Gaeta M, 2. Minutoli F, 3. Scribano E GaetaM, MinutoliF, ScribanoE, et al: CT and MR imaging findings in athletes with early tibial stress injuries: Comparison with bone scintigraphy findings and emphasis on cortical abnormalities. Radiology 2005;235(2):553-561.pmid:15858094 Abstract/FREE Full Text 9. 8.↵ 1. Banal F, 2. Gandjbakhch F, 3. Foltz V BanalF, GandjbakhchF, FoltzV, et al: Sensitivity and specificity of ultrasonography in early diagnosis of metatarsal bone stress fractures: A pilot study of 37 patients. J Rheumatol 2009;36(8):1715-1719.pmid:19567620 Abstract/FREE Full Text 10. 9. 1. Arni D, 2. Lambert V, 3. Delmi M, 4. Bianchi S ArniD, LambertV, DelmiM, BianchiS: Insufficiency fracture of the calcaneum: Sonographic findings. J Clin Ultrasound 2009;37(7):424-427.pmid:19353549 MedlineWeb of Science 11. 10.↵ 1. Saxena A, 2. Fullem B, 3. Hannaford D SaxenaA, FullemB, HannafordD: Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg 2000;39(2):96-103.pmid:10789100 Medline 12. 11.↵ 1. Young AJ, 2. McAllister DR YoungAJ, McAllisterDR: Evaluation and treatment of tibial stress fractures. Clin Sports Med 2006;25(1):117-128, x.pmid:16324978 CrossRefMedlineWeb of Science 13. 12.↵ 1. Holick MF HolickMF: Vitamin D deficiency. N Engl J Med 2007;357(3):266-281.pmid:17634462 CrossRefMedlineWeb of Science 14. 13.↵ 1. Shima Y, 2. Engebretsen L, 3. Iwasa J, 4. Kitaoka K, 5. Tomita K ShimaY, EngebretsenL, IwasaJ, KitaokaK, TomitaK: Use of bisphosphonates for the treatment of stress fractures in athletes. Knee Surg Sports Traumatol Arthrosc 2009;17(5):542-550.pmid:19048230 Medline 15. 14.↵ 1. Stewart GW, 2. Brunet ME, 3. Manning MR, 4. Davis FA StewartGW, BrunetME, ManningMR, DavisFA: Treatment of stress fractures in athletes with intravenous pamidronate. Clin J Sport Med 2005;15(2):92-94.pmid:15782053 Medline 16. 15.↵ 1. Milgrom C, 2. Finestone A, 3. Novack V MilgromC, FinestoneA, NovackV, et al: The effect of prophylactic treatment with risedronate on stress fracture incidence among infantry recruits. Bone 2004;35(2):418-424.pmid:15268892 Medline 17. 16.↵ 1. Koester MC, 2. Spindler KP KoesterMC, SpindlerKP: Pharmacologic agents in fracture healing. Clin Sports Med 2006;25(1):63-73, viii.pmid:16324974 CrossRefMedlineWeb of Science 18. 17. 1. Komatsubara S, 2. Mori S, 3. Mashiba T KomatsubaraS, MoriS, MashibaT, et al: Human parathyroid hormone (1-34) accelerates the fracture healing process of woven to lamellar bone replacement and new cortical shell formation in rat femora. Bone 2005;36(4):678687.pmid:15781006 Medline 19. 18.↵ 1. Andreassen TT, 2. Ejersted C, 3. Oxlund H AndreassenTT, EjerstedC, OxlundH: Intermittent parathyroid hormone (1-34) treatment increases callus formation and mechanical strength of healing rat fractures. J Bone Miner Res 1999;14(6):960-968.pmid:10352105 CrossRefMedlineWeb of Science 20. 19. 1. Holzer G, 2. Majeska RJ, 3. Lundy MW, 4. Hartke JR, 5. Einhorn TA HolzerG, MajeskaRJ, LundyMW, HartkeJR, EinhornTA: Parathyroid hormone enhances fracture healing: A preliminary report. Clin Orthop Relat Res 1999;366(366):258263.pmid:10627743 Medline 21. 20.↵ 1. Rue JP, 2. Armstrong DW III, 3. Frassica FJ, 4. Deafenbaugh M, 5. Wilckens JH RueJP, ArmstrongDW III, FrassicaFJ, DeafenbaughM, WilckensJH: The effect of pulsed ultrasound in the treatment of tibial stress fractures. Orthopedics 2004;27(11):1192-1195.pmid:15566133 MedlineWeb of Science 22. 21.↵ 1. Heckman JD, 2. Ryaby JP, 3. McCabe J, 4. Frey JJ, 5. Kilcoyne RF HeckmanJD, RyabyJP, McCabeJ, FreyJJ, KilcoyneRF: Acceleration of tibial fracture healing by non-invasive low-intensity pulsed ultrasound. J Bone Joint Surg Am 1994;76(1):26-34. Medline 23. 22.↵ 1. Johannes EJ, 2. Kaulesar Sukul DM, 3. Matura E JohannesEJ, Kaulesar SukulDM, MaturaE: High-energy shock waves for the treatment of nonunions: An experiment on dogs. J Surg Res 1994;57(2):246252.pmid:8028332 CrossRefMedlineWeb of Science 24. 23.↵ 1. Taki M, 2. Iwata O, 3. Shiono M, 4. Kimura M, 5. Takagishi K TakiM, IwataO, ShionoM, KimuraM, TakagishiK: Extracorporeal shock wave therapy for resistant stress fracture in athletes: A report of 5 cases. Am J Sports Med 2007;35(7):1188-1192.pmid:17293467 FREE Full Text 25. 24.↵ 1. Beals RK, 2. Cook RD BealsRK, CookRD: Stress fractures of the anterior tibial diaphysis. Orthopedics 1991;14(8):869-875.pmid:1923968 MedlineWeb of Science 26. 25.↵ 1. Batt ME, 2. Kemp S, 3. Kerslake R BattME, KempS, KerslakeR: Delayed union stress fractures of the anterior tibia: Conservative management. Br J Sports Med 2001;35(1):74-77.pmid:11157470 Abstract/FREE Full Text 27. 26.↵ 1. Rettig AC, 2. Shelbourne KD, 3. McCarroll JR, 4. Bisesi M, 5. Watts J RettigAC, ShelbourneKD, McCarrollJR, BisesiM, WattsJ: The natural history and treatment of delayed union stress fractures of the anterior cortex of the tibia. Am J Sports Med 1988;16(3):250-255.pmid:3381982 Abstract/FREE Full Text 28. 27.↵ 1. Chang PS, 2. Harris RM ChangPS, HarrisRM: Intramedullary nailing for chronic tibial stress fractures: A review of five cases. Am J Sports Med 1996;24(5):688-692.pmid:8883694 Abstract/FREE Full Text 29. 28.↵ 1. Borens O, 2. Sen MK, 3. Huang RC BorensO, SenMK, HuangRC, et al: Anterior tension band plating for anterior tibial stress fractures in high-performance female athletes: A report of 4 cases. J Orthop Trauma 2006;20(6):425-430.pmid:16825970 CrossRefMedlineWeb of Science 30. 29.↵ 1. Court-Brown CM, 2. Gustilo T, 3. Shaw AD Court-BrownCM, GustiloT, ShawAD: Knee pain after intramedullary tibial nailing: Its incidence, etiology, and outcome. J Orthop Trauma 1997;11(2):103105.pmid:9057144 CrossRefMedlineWeb of Science 31. 30.↵ 1. Mann JA, 2. Pedowitz DI MannJA, PedowitzDI: Evaluation and treatment of navicular stress fractures, including nonunions, revision surgery, and persistent pain after treatment. Foot Ankle Clin 2009;14(2):187-204.pmid:19501802 CrossRefMedline 32. 31.↵ 1. Golano P, 2. Fariñas O, 3. Sáenz I GolanoP, FariñasO, SáenzI: The anatomy of the navicular and periarticular structures. Foot Ankle Clin 2004;9(1):1-23.pmid:15062212 Medline 33. 32.↵ 1. Khan KM, 2. Fuller PJ, 3. Brukner PD, 4. Kearney C, 5. Burry HC KhanKM, FullerPJ, BruknerPD, KearneyC, BurryHC: Outcome of conservative and surgical management of navicular stress fracture in athletes: Eighty-six cases proven with computerized tomography. Am J Sports Med 1992;20(6):657666.pmid:1456359 Abstract/FREE Full Text 34. 33.↵ 1. Torg JS, 2. Moyer J, 3. Gaughan JP, 4. Boden BP TorgJS, MoyerJ, GaughanJP, BodenBP: Management of tarsal navicular stress fractures: Conservative versus surgical treatment. A meta-analysis. Am J Sports Med 2010;38(5):1048-1053.pmid:20197494 Abstract/FREE Full Text 35. 34.↵ 1. Torg JS, 2. Pavlov H, 3. Cooley LH TorgJS, PavlovH, CooleyLH, et al: Stress fractures of the tarsal navicular: A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64(5):700712.pmid:7085695 MedlineWeb of Science 36. 35.↵ 1. Torg JS, 2. Balduini FC, 3. Zelko RR, 4. Pavlov H, 5. Peff TC, 6. Das M TorgJS, BalduiniFC, ZelkoRR, PavlovH, PeffTC, DasM: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for non-surgical and surgical management. J Bone Joint Surg Am 1984;66(2):209-214.pmid:6693447 Medline 37. 36.↵ 1. Clapper MF, 2. O’Brien TJ, 3. Lyons PM ClapperMF, O’BrienTJ, LyonsPM: Fractures of the fifth metatarsal: Analysis of a fracture registry. Clin Orthop Relat Res 1995;(315):238-241.pmid:7634674 Medline 38. 37.↵ 1. Porter DA, 2. Duncan M, 3. Meyer SJ PorterDA, DuncanM, MeyerSJ: Fifth metatarsal Jones fracture fixation with a 4.5-mm cannulated stainless steel screw in the competitive and recreational athlete: A clinical and radiographic evaluation. Am J Sports Med 2005;33(5):726733.pmid:15722272 Abstract/FREE Full Text 39. 38.↵ 1. Nihal A, 2. Trepman E, 3. Nag D NihalA, TrepmanE, NagD: First ray disorders in athletes. Sports Med Arthrosc 2009;17(3):160-166.pmid:19680112 CrossRefMedline 40. 39. 1. Cohen BE CohenBE: Hallux sesamoid 104.pmid:19232995 disorders. Foot Ankle Clin 2009;14(1):91- MedlineWeb of Science 41. 40.↵ 1. Shelbourne KD, 2. Fisher DA, 3. Rettig AC, 4. McCarroll JR ShelbourneKD, FisherDA, RettigAC, McCarrollJR: Stress fractures of the medial malleolus. Am J Sports Med 1988;16(1):60-63.pmid:3344882 Abstract/FREE Full Text « Previous | Next Article »Table of Contents This Article 1. doi: 10.5435/JAAOS-20-03-167 J Am Acad Orthop Surg March 2012 vol. 20 no. 3 167-176 1. AbstractFree 2. » Full Text 3. Full Text (PDF) - Classifications 1. o Review Article - Services 1. Email this article to a colleague 2. Alert me when this article is cited 3. Alert me if a correction is posted 4. Similar articles in this journal 6. Download to citation manager 7. + Citing Articles + Google Scholar + PubMed + Related Content Navigate This Article 1. Top 2. Abstract 3. Risk Factors 4. Diagnosis 5. Imaging 6. Nonsurgical Management 7. Management of Specific High-Risk Stress Fractures 8. Summary 9. Figures 10. References This Article 1. doi: 10.5435/JAAOS-20-03-167 J Am Acad Orthop Surg March 2012 vol. 20 no. 3 167-176 1. AbstractFree 2. » Full Text 3. Full Text (PDF) Navigate This Article 1. Top 2. Abstract 3. Risk Factors 4. Diagnosis 5. Imaging 6. Nonsurgical Management 7. Management of Specific High-Risk Stress Fractures 8. Summary 9. Figures 10. References This Month's Issue March 2012Vol. 20, No. 3 1. 1. Alert me to new issues of JAAOS About the Journal Supplements to JAAOS Editorial Board Authors & Reviewers Letters Submissions Subscriptions JAAOS SAE CME Reprints Permission Requests Advertising Specialty Society Meetings Feedback Contact Us Help The American Academy of Orthopaedic Surgeons publishes the Journal of the American Academy of Orthopaedic Surgeons. Stanford University Libraries' HighWire Press ® assists in the publication of JAAOS Online Copyright © 2012 by the American Academy of Orthopaedic Surgeons