New York State Medicaid Preferred Drug Program
Sovaldi® Combination Therapy Prior Authorization Worksheet
Fax Number: (800) 268-2990
Enrollee Information
ENROLLEE NAME:
ENROLLEE MEDICAID ID NUMBER (2 LETTERS, 5 NUMBERS, 1 LETTER):
ENROLLEE DATE OF BIRTH:
GENDER:
Female
Male
Prescriber Information
PRESCRIBER NAME:
CONTACT PERSON:
10-DIGIT NPI NUMBER:
OFFICE PHONE NUMBER:
(
)
-
OFFICE FAX NUMBER:
(
)
-
Are you a gastroenterologist, hepatologist, transplant physician or infectious disease specialist?
YES
NO
If no, are you working in collaboration with a specialist listed above?
YES
NO
If no, do you have clinical experience with the management and treatment of hepatitis c virus (HCV) infection?
YES
NO
Clinical experience is defined as the management AND treatment of at least 10 patients with HCV infection within the past 12 months
and at least 10 HCV-related CME credits in the last 12 months.
Clinical Criteria
MEDICAL STATUS
Diagnosis (Please check all that apply):
Chronic Hepatitis C Infection
HCV Genotype:
Has documentation confirming genotype been submitted?
Is the patient interferon ineligible?
Without cirrhosis
Compensated cirrhosis
Decompensated cirrhosis
Hepatocellular Carcinoma awaiting liver transplantation
Has documentation confirming hepatocellular carcinoma been submitted?
Status post-liver transplant
Yes
Yes
No
No
Yes
No
Please indicate liver fibrosis stage (METAVIR score) :
0
1
2
3
4
Other
Liver fibrosis should be confirmed utilizing one of the following methods: liver biopsy, transient elastography (FibroScan®) score ≥ 9.5kPa,
FibroSure® score ≥ 0.58, APRI score > 1.5 or radiological imaging consistent with cirrhosis (e.g. evidence of portal hypertension).
BASELINE RNA LEVEL:
DATE TAKEN:
Has documentation confirming baseline HCV RNA been submitted?
Yes
No
TREATMENT HISTORY
Is the patient initiating or continuing a Sovaldi regimen?
If continuation of therapy, what is the regimen? :
If continuation of therapy, was the Sovaldi regimen started in another health care setting?
Is the patient treatment-naïve with Sovaldi?
Is the patient treatment-naïve with Daklinza?
Please check the box that best describes the patient’s HCV Treatment status:
Initiation
Continuation
Yes
Yes
Yes
No
No
No
Treatment-naïve
Prior relapser (achieved undetectable HCV RNA at end of previous treatment with peginterferon and ribavirin but detectable within
24 weeks after treatment)
Prior partial responder (≥2 log decrease in HCV RNA at week 12 of previous treatment with peginterferon and ribavirin but did not
achieve undetectable HCV RNA at end of treatment)
Prior null responder (achieved <2 log decrease in HCV RNA at week 12 of previous treatment with peginterferon and ribavirin)
For billing questions, call 1-800-343-9000.
For clinical concerns or Preferred Drug Program questions, visit www.nyhealth.gov
and http://newyork.fhsc.com or call 1-877-309-9493.
© 2015, Magellan Health Services, Inc. All Rights Reserved.
Magellan Medicaid Administration
Sovaldi® Combination Therapy Prior Authorization Worksheet
TREATMENT HISTORY (CONT.)
Please provide previous HCV therapy completed prior to the date of this request (IF APPLICABLE):
DRUG:
DOSAGE FORM:
STRENGTH:
DRUG:
DOSAGE FORM:
STRENGTH:
DRUG:
DOSAGE FORM:
STRENGTH:
How many weeks of previous therapy have been completed prior to the date of this request?
DIRECTION:
DIRECTION:
DIRECTION:
CONCOMITANT CONDITIONS/COMORBIDITIES
Is the patient co-infected with chronic hepatitis B infection?
Is the patient co-infected with HIV/AIDS?
If yes, has the patient had undetectable viral load for the past 6 months?
Has the patient had a liver transplant?
Does the patient have co-existent liver disease, such as nonalcoholic steatohepatitis (NASH)?
Does the patient have type 2 diabetes mellitus (insulin resistant)?
Does the patient have debilitating fatigue that is impacting their quality of life
(e.g., secondary to extra-hepatic manifestations and/or liver disease)?
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
Yes
No
Does the patient have evidence of extra-hepatic manifestation of hepatitis C?
If yes, please check all that apply below:
Yes
No
Documentation of the presence of extra-hepatic manifestations based on lab results or imaging results (e.g., CBC, erythrocyte
sedimentation rate (ESR)/C-reactive protein (CRP), urinalysis, BUN/creatinine and angiography) must be submitted.
Hematological:
Cryoglobulinemia (e.g. Type 2 or 3 essential mixed cryoglobulinemia)
Lymphoma
Multiple myeloma
Renal Disease:
Proteinuria
Nephrotic syndrome
Membranoproliferative glomerulonephritis
Renal failure
Cutaneous:
Porphyria cutanea tarda
Lichen myxedematosus
Rheumatologic:
Behçet’s disease
Raynaud’s syndrome
Systemic lupus erythematosus
Rheumatoid arthritis
PREGNANCY
For female patients of child bearing potential: Has a negative pregnancy test been collected
within 30 days prior to initiation of therapy OR medical record submitted documenting pregnancy status?
Revision Date: October 2015
For billing questions, call 1-800-343-9000.
For clinical concerns or Preferred Drug Program questions, visit
www.nyhealth.gov and http://newyork.fhsc.com or call 1-877-309-9493.
Yes
No
Page 2
Magellan Medicaid Administration
Sovaldi® Combination Therapy Prior Authorization Worksheet
TREATMENT READINESS
Please indicate which of the following scales/assessment tools was used to evaluate the readiness of the patient (only one is required):
SAMHSA-HRSA Center for Integrated Health Solutions – Drug & Alcohol Screening Tools – Available at:
http://www.integration.samhsa.gov/clinical-practice/screening-tools#drugs
If checked, please provide the name of SAMSHA-HRSA drug and alcohol screening tool used (required):
Psychosocial Readiness Evaluation and Preparation for Hepatitis C Treatment (PREP-C) – Available at: www.prepc.org
Has the patient demonstrated treatment readiness, including the ability to adhere to the
prescribed treatment regimen?
Yes
No
CONTINUATION OF THERAPY REQUESTS **THIS PORTION IS NOT REQUIRED FOR INITIAL THERAPY REQUESTS
WEEK 4 ( ±2 WEEKS)
HCV RNA LEVEL:
DATE TAKEN:
WEEK 12 HCV RNA LEVEL:
DATE TAKEN:
Has documentation confirming HCV RNA levels at the appropriate week been submitted?
Yes
No
Has the patient completed all HCV evaluation appointments and procedures and demonstrated
compliance to their treatment regimen?
Yes
No
CURRENT TREATMENT REGIMEN
Please indicate the treatment regimen that is being prescribed:
Accepted Regimens and Treatment Duration for Sovaldi Combination Therapy in HCV
Diagnosis
Treatment Regimen
Length of Authorization
HCV Genotype 1 or 4
(interferon eligible)
Sovaldi + peginterferon alfa +
ribavirin
12 weeks
HCV Genotype 1 or 4
(interferon ineligible)
Sovaldi + ribavirin
24 weeks
HCV Genotype 1
HCV Genotype 1
with cirrhosis
Sovaldi + Olysio
12 weeks
Sovaldi + Olysio
24 weeks
HCV Genotype 2
HCV Genotype 2
with cirrhosis
HCV Genotype 3
Sovaldi + ribavirin
12 weeks
Sovaldi + ribavirin
16 weeks
Sovaldi + ribavirin
24 weeks
Sovaldi + peginterferon +
ribavirin
12 weeks
HCV Genotype 3
HCV Genotype 3
Patients with Genotype 1-4
awaiting liver transplant
Sovaldi + Daklinza
12 weeks
48 weeks or time of liver
transplantation, whichever comes first
Sovaldi + ribavirin
Please provide dosing information for the treatment regimen selected above:
Sovaldi
STRENGTH:
DIRECTION:
QUANTITY:
REFILLS:
Daklinza STRENGTH:
DIRECTION:
QUANTITY:
REFILLS:
Pegasys
Pegintron DOSAGE FORM:
DIRECTION:
Ribavirin
Other Ribavirin Product
Olysio
STRENGTH:
Other
STRENGTH:
Revision Date: October 2015
STRENGTH:
DIRECTION:
DIRECTION:
QUANTITY:
DIRECTION:
QUANTITY:
QUANTITY:
REFILLS:
QUANTITY:
REFILLS:
REFILLS:
REFILLS:
For billing questions, call 1-800-343-9000.
For clinical concerns or Preferred Drug Program questions, visit
www.nyhealth.gov and http://newyork.fhsc.com or call 1-877-309-9493.
Page 3
Magellan Medicaid Administration
Sovaldi® Combination Therapy Prior Authorization Worksheet
Please answer the following questions if requesting a non-preferred ribavirin product as part of treatment:
Patient has experienced a treatment failure with a preferred drug.
Yes
No
Patient has experienced an adverse drug reaction with a preferred drug.
Yes
No
There is a documented history of successful therapeutic control with a nonpreferred drug and transition to a
preferred drug is medically contraindicated.
Yes
No
Other (Please specify the clinical reason the patient is unable to use a preferred agent in the same drug class. If necessary, fax
additional pages):
Please provide any additional information that should be considered in the space below:
I attest that this is medically necessary for this patient and that all of the information on this form is accurate to
the best of my knowledge. I attest that documentation of the above diagnosis and medical necessity is available
for review if requested by New York Medicaid.
PRESCRIBER’S SIGNATURE
Revision Date: October 2015
DATE
For billing questions, call 1-800-343-9000.
For clinical concerns or Preferred Drug Program questions, visit
www.nyhealth.gov and http://newyork.fhsc.com or call 1-877-309-9493.
Page 4
Sofosbuvir (Sovaldi™)
Sofosbuvir is a new oral treatment option for patients with chronic hepatitis C virus (HCV) genotype 1, 2, 3, or 4 infection, including
those with hepatocellular carcinoma meeting Milan criteria (awaiting liver transplant) and those with HCV/ human
immunodeficiency virus (HIV)- 1 co-infection. Approved by the Food and Drug Administration (FDA) in December 2013, sofosbuvir is
the first direct-acting antiviral (DAA) agent in the nucleoside/nucleotide polymerase inhibitor class. A nucleotide analog, sofosbuvir
interferes with the HCV life cycle by inhibiting HCV NS5B ribonucleic acid (RNA)-dependent RNA polymerase to prevent replication of
the HCV virus. Sofosbuvir is indicated for use in combination with peginterferon alfa and ribavirin (PR) for HCV genotypes 1 and 4
and in combination with ribavirin (RBV) for genotypes 2 and 3 as well as for genotype 1 in patients who are interferon ineligible.1
Advantages of sofosbuvir
Sofosbuvir is taken orally once daily with or without food as a component of an antiviral treatment regimen. The treatment regimen
and duration is dependent on both the HCV genotype and patient characteristics. Published phase 3 trials have demonstrated the
efficacy of sofosbuvir in combination with PR for patients with genotype 1 or 4 and in combination with RBV alone for patients with
genotype 2 or 3. Additionally, per unpublished data from the manufacturer, sustained virologic response (SVR) has been successfully
achieved in patients co-infected with HIV-1 and in patients with hepatocellular carcinoma (HCC) awaiting liver transplantation. 1
Recommended treatment regimens are identical for patients with HCV mono-infection or HCV/HIV-1 co-infection. In clinical trials,
treatment duration was fixed and not guided by HCV RNA response. The primary endpoint was defined as HCV RNA less than the
lower level of quantification (<25 IU/mL) at 12 weeks post treatment (SVR12).
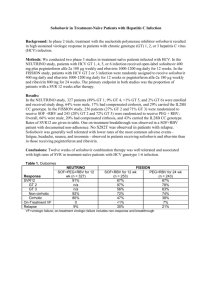
Published phase III trials:
Trial
Subjects
NEUTRINO1,2
327 treatment-naïve adults
FISSION1,2
499 treatment-naïve adults
POSITRON1,3
FUSION1,3
278 interferon intolerant, ineligible or
unwilling adults (81% no prior treatment)
201 adults with prior breakthrough,
relapse, or null response with interferon
Treatment arms
SOF + PR x 12 weeks
Adjusted historical control
SOF + RBV x 12 weeks
PR x 24 weeks
SOF + RBV x 12 weeks
Placebo x 12 weeks
SOF + RBV x 12 weeks
SOF + RBV x 16 weeks
Overall
SVR12 rate
90%
60%
67%
67%
78%
0%
50%
71%
SVR12 rate by genotype
2
3
4
96%
--NR
95%
56%
--78%
63%
93%
61%
--0%
0%
82%
30%
--89%
62%
1
89%
NR
SOF = sofosbuvir; PR = peginterferon + ribavirin; RBV = ribavirin; NR=not reported
Cautions
Coadministration of amiodarone with sofosbuvir in combination with another DAA is not recommended due to risk of severe
symptomatic bradycardia.
Sofosbuvir is a substrate of P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP) drug transporters. Do not
coadminister sofosbuvir with potent P-gp inducers due to risk of reduced sofosbuvir concentrations and treatment failure.
Sofosbuvir should not be used as monotherapy and only as a component of an antiviral regimen dependent on the patient’s
genotype and other conditions (see table below). Sofosbuvir dose must not be reduced nor should treatment be interrupted.
For patients with severe renal impairment or with end stage renal disease, no dose recommendations are available.
Where does sofosbuvir fit into therapy and how should it be used?
In January 2014, The American Association for the Study of Liver Diseases and Infectious Diseases Society of America, in
collaboration with the International Antiviral Society – USA, launched www.hcvguidelines.org for the purpose of disseminating
expert opinion on management of chronic HCV as newer HCV DAA become available and treatment evidence emerges. There are no
comparative efficacy data available to date among the HCV DAA, but it is likely that guidelines for optimal regimens will continue to
evolve and will need to integrate patient-specific as well as economic factors. Many patient-specific factors must be taken into
consideration when deciding to initiate therapy and baseline genotype must be established to guide treatment regimen and
duration as outlined below. Sofosbuvir is dosed 400 mg once daily with or without food. The goal of treatment is undetectable HCV
RNA at least 12 weeks post-treatment (SVR12).
Sofosbuvir Treatment Regimen and Duration Recommendations1
HCV Mono-infected and HCV/HIV Co-infected
Treatment
Duration
Genotype 1 or 4
SOF + PR
12 weeks
Genotype 2
SOF + RBV
12 weeks
Genotype 1 interferon ineligible or Genotype 3
SOF + RBV
24 weeks
Note: For patients with HCC awaiting liver transplantation, the recommended treatment is SOF + RBV for up to 48 weeks or until transplant, whichever occurs first.
References: 1. Sovaldi™ product information. Gilead Sciences, 2015. 2. Lawitz et al. NEJM 2013;368(20):1878-87. 3. Jacobson et al. NEJM 2013;368(20):1867-77.
Revision Date: April 2015
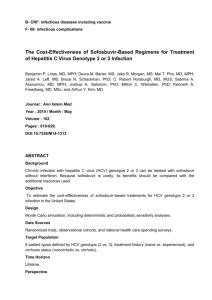
Sofosbuvir Initiation and Monitoring
Once patient readiness for chronic hepatitis C virus (HCV) treatment has been determined, the algorithm below outlines
key decision points for initiating and monitoring combination therapy including sofosbuvir.
Note: Ribavirin is contraindicated in pregnancy therefore all female patients of childbearing age (or female partners of
male patients) should be sure they are not pregnant prior to beginning treatment and should use 2 methods of nonhormonal birth control throughout treatment. Also note, HCV RNA testing should be conducted using a sensitive assay.
Has the patient been diagnosed with HCV genotype 1, 2, 3 or
4 and received quantitative HCV RNA testing?
No
Seek alternative treatment options
or conduct testing prior to
treatment
Yes
Does the patient have hepatocellular carcinoma and
awaiting liver transplantation?
Yes
Genotype 1 interferon
ineligible or genotype 2 or 3
or
Initiate sofosbuvir 400 mg once daily
with weight based ribavirin
Genotype 1 interferon
eligible or genotype 4
Initiate sofosbuvir 400 mg once daily with
peginterferon alpha and weight based ribavirin
Continue sofosbuvir 400 mg once daily as a component of antiviral
therapy to the end of treatment week 12
Repeat quantitative HCV RNA. Is HCV RNA ≤ 25 IU/ ml?
No
Evaluate patient adherence and
consider discontinuing therapy.
If therapy is discontinued no
further HCV RNA testing is required
Yes
Hepatocellular carcinoma: continue
regimen for up to an additional 36
weeks or until liver transplantation,
whichever occurs first, for total
treatment duration of 48 weeks
Genotype 1 interferon ineligible or
genotype 3: continue regimen for
an additional 12 weeks for total
treatment duration of 24 weeks
Genotype 1 interferon eligible or
genotype 2 or 4: treatment is
complete
Obtain HCV RNA 12 weeks after the end of treatment to determine
sustained virological response (SVR12)
Revision Date: April 2015
Daclatasvir (Daklinza™)
Daclatasvir (Daklinza™) is indicated for the treatment of chronic hepatitis C virus (HCV) genotype 3 infection in combination with
sofosbuvir (Sovaldi®) in adult patients. 1 Daclatasvir, a direct-acting antiviral (DAA) agent, is a HCV NS5A inhibitor that received Food
and Drug Administration (FDA) approval in July 2015. Sustained virologic response rates (SVR) with the combination of daclatasvir
and sofosbuvir (HCV nucleotide analog NS5B polymerase inhibitor) are reduced in HCV genotype 3 infected patients with cirrhosis.
Safety and efficacy has not been established in patients with decompensated cirrhosis or liver transplant patients.
Daclatasvir is a substrate of cytochrome P450 3A (CYP3A) and is primarily metabolized by CYP3A. Additionally, daclatasvir is an
inhibitor of P-glycoprotein (P-gp), organic anion transport polypeptide (OATP) 1B1 and 1B3 and breast cancer resistance protein
(BCRP). The metabolism of daclatasvir can alter the drug concentrations of other drugs and conversely other drugs may alter the
drug concentration of daclatasvir.
The recommended oral dosage of daclatasvir is 60 mg once daily with or without food. Daclatasvir must be given in combination
with sofosbuvir 400 mg once daily for 12 weeks. The daclatasvir dose should be reduced to 30 mg once daily when given in
combination with drugs that strongly inhibit CYP3A. Conversely, when used in combination with drugs that moderately induce
CYP3A, the daclatasvir dose should be increased to 90 mg once daily. Daclatasvir is contraindicated in combination with drugs that
strongly induce CYP3A (i.e., phenytoin, carbamazepine, rifampin, and St. John’s wort). Daclatasvir is commercially available in 30 mg
and 60 mg tablets.
Advantages of daclatasvir
The daclatasvir and sofosbuvir combination is an oral regimen consisting of one tablet of each drug given once daily for 12 weeks
with or without food. The combination is FDA approved for the treatment of patients with HCV genotype 3 infection. No dose
adjustments are needed for patients with renal impairment. Additionally, no dose adjustments are needed for patients with mild
(Child-Pugh A), moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment.
Safety and efficacy of the combination of daclatasvir and sofosbuvir was evaluated in one phase 3 open label trial (ALLY-3) in HCV
genotype 3 infected patients.2 The primary endpoint of the study was defined as HCV RNA less than the lower level of quantification
(<25 IU/mL) at 12 weeks post-treatment (SVR12). Overall, 89% of the patients achieved SVR12. SVR12 rates for treatment-naïve and
treatment-experienced patients were 90% and 86%, respectively. The SVR12 rate for patients with compensated cirrhosis was 63%
compared to 96% for those patents without cirrhosis.
Cautions
Daclatasvir is contraindicated in combination with drugs that strongly induce CYP3A, as the effectiveness of
daclatasvir is reduced. The daclatasvir dose should be increased when given in combination with drugs that
moderately induce CY3A and reduced when given in combination with drugs that inhibit CYP3A.
Co-administration of amiodarone with daclatasvir and sofosbuvir can result in bradycardia and is not
recommended. If the combination cannot be avoided then cardiac monitoring is recommended.
For patients utilizing daclatasvir concurrently with dabigatran, the patient’s renal function should be monitored.
Dabigatran dose adjustments may be required.
Daclatasvir can increase the therapeutic concentration of digoxin. For patients initiating digoxin therapy, start
with the lowest digoxin dose and for patients already receiving digoxin, reduce digoxin dose by 30% to 50% or
modify the dosing frequency. Digoxin blood levels should be monitored.
Concurrent administration of daclatasvir and lipid lowering agents, 3-hydroxy-3-methyl-glutaryl-CoA reductase
inhibitors (HMG-CoA reductase inhibitors/ statins) can result in an increase in the therapeutic levels of statins.
Patients should be monitored for adverse events.
SVR12 can be reduced in HCV genotype 3 infected patients with cirrhosis. Daclatasvir safety and efficacy has not
been established in patients with decompensated cirrhosis or liver transplant patients. No dosage adjustments
are needed for patients with mild (Child-Pugh A), moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic
impairment.
Currently there is no daclatasvir data in pregnant women and the benefits and risks should be evaluated before
prescribing to a pregnant woman. In animal studies (i.e., rats and rabbits) embryofetal toxicity was observed at
maternally toxic doses that produced exposures 33 and 98 times the human exposure, respectively.
Revision Date: September 1, 2015
Where does daclatasvir fit into therapy?
In January 2014, The American Association for the Study of Liver Diseases and Infectious Diseases Society of America, in
collaboration with the International Antiviral Society – USA, launched www.hcvguidelines.org for the purpose of disseminating
expert opinion on management of CHC as newer HCV DAA become available and treatment evidence emerges. There are no
comparative efficacy data available to date for the HCV DAA, but it is likely that guidelines for optimal regimens will continue to
evolve and will need to integrate patient-specific as well as economic factors.
Many patient-specific factors must be taken into consideration when deciding to initiate therapy and baseline host and viral factors
will affect relapse rates and treatment duration. The goal of treatment is undetectable HCV RNA 12 weeks post-treatment (SVR12).
Daclatasvir with sofosbuvir for 12 weeks is an option for patients with HCV genotype 3 infections without cirrhosis.
References: 1. Dakinza™ prescribing information. Bristol-Myers Squibb, 2015. 2. Nelson, D. et al. Hepatology. 2015; 61(4): 1127-1135.
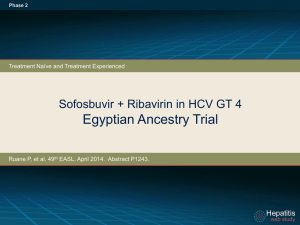
Daclatasvir Initiation and Monitoring
Once patient readiness for chronic hepatitis C virus (HCV) treatment has been determined, the algorithm below outlines
key decision points for initiating and monitoring of daclatasvir.
Has the patient been diagnosed with HCV
genotype 3 without cirrhosis* and received
quantitative HCV RNA testing?
NO
Seek alternative treatment options or
conduct testing prior to treatment
YES
NO
Has a review of the patient’s medication
record been completed?
YES
Complete a medication profile review prior
to initiating treatment.
Dose adjustments are required for drugs
that moderately induce CYP3A and drugs
that are strong inhibitors of CYP3A.**
Drugs that strongly induce CYP3A are
contraindicated.
Start the combination daclatasvir and
sofosbuvir with one tablet of each agent daily
for 12 weeks.
Obtain HCV RNA level 12 weeks after
completion of therapy to determine SRV12.
CYP3A = cytochrome P450 3A; SVR= sustained virological response
*SVR rates are reduced in HCV genotype 3 infected patients with cirrhosis
**Refer to the daclatasvir product label for a list of drugs that are strong or moderate inducers of CYP3A, drugs that are strong inhibitors of CYP3A
and other drugs that require dose adjustments and monitoring.
Revision Date: September 1, 2015