APA Template - Dana Raymer`s Professional Portfolio
advertisement

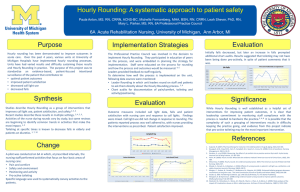
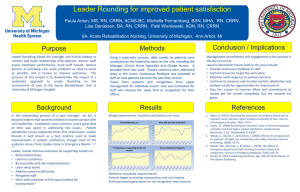
Running head: LEADERSHIP STRATEGY ANALYSIS Leadership Strategy Analysis – Quality Improvement Process Dana L. Raymer Ferris State University 1 LEADERSHIP STRATEGY ANALYSIS 2 Abstract For this paper, the activity of hourly rounding will be analyzed from a quality improvement perspective. The quality improvement process set forth includes describing the issue of lack of compliance with hourly rounding policies at Mercy Hospital-Cadillac. Team members are selected, the issue is studied further, and strategies are developed and implemented to improve this area of clinical practice. Evaluation methods are also presented to measure the success of the planned strategies toward desired outcomes. Being able to analyze practices from a quality improvement perspective is important in today’s nursing, as hospitals and nurses are required to be as efficient as possible while providing quality care. LEADERSHIP STRATEGY ANALYSIS 3 Leadership Strategy Analysis – Quality Improvement Process Nurses need to continuously strive to improve the quality and safety of patient care. Analyzing activities and policies in order to improve them is an important process for nurses to engage in, in order to improve patient outcomes. Approximately one year ago, Mercy HospitalCadillac implemented an hourly rounding initiative. This practice was in line with current evidence that showed that checking on patients every hour resulted in improved outcomes and increased patient satisfaction. Staff compliance with this initiative has been poor, so this practice will be reviewed and strategies will be developed and put into effect that will improve adherence to this activity that has proven positive effects. Clinical Need for Hourly Rounding Studies on the subject of hourly rounding have shown that this practice can reduce the frequency of patients' call light use, reduce the incidence of pressure ulcers and reduce the occurrence of falls (Claude-Gutekust, Donches, Dries, Kessler, & Snyde, 2012). Hourly rounding has also been found to increase patient satisfaction and safety while improving clinical excellence and reducing fragmentation of care (Rondelli, Ecker, Crawford, Seelinger, & Omery, 2012). The lack of staff compliance with hourly rounding policies at Mercy Hospital-Cadillac can have major financial impacts, as Medicare is no longer reimbursing hospitals for the cost of treating hospital-acquired pressure ulcers and injuries from falls, and Medicare incentive payments will soon be made in part based upon patient satisfaction. Interdisciplinary Team “QI team members should represent a cross section of workers who are involved with the problem” (Yoder-Wise, 2011, p. 395). Members of the team assembled to analyze this issue should include the director of nursing, unit level managers, charge nurses, staff nurses and nurse LEADERSHIP STRATEGY ANALYSIS 4 assistants. Staff nurses should include representatives from all shifts and all inpatient units. According to Yoder-Wise (2011), including nurses involved in patient care in quality improvement exercises increases both quality and safety of patient care and also positively impacts job satisfaction and nurses’ perception of work environment. That is why it is important to make sure that the nurses who are going to be actually completing the hourly rounding are involved with the analysis and decision making process. Data Collection Method A questionnaire regarding nurses’ perceptions of the importance of hourly rounding and perceived barriers to implementing hourly rounding can be developed and disseminated for staff to answer. This will enable the team to decide what factor or factors are negatively impacting staff’s willingness or ability to complete hourly rounding satisfactorily. Perhaps the staff needs more education so they understand the positive results that occur because of hourly rounding or maybe they need to be shown studies that show that hourly rounding saves time because care is not fragmented by frequent call lights. A histogram can be used to display responses and easily see which issues staff feels are the most prohibitive regarding implementation. Outcomes According to Yoder-Wise (2011), after analysis of data is completed, the quality improvement team should identify goals for improvement that involve both a standard of practice and a nursing-sensitive outcome. In this situation, a process goal could be set that states that all inpatient units will have a 90% or greater compliance rate with hourly rounding. Nursing-sensitive patient outcomes are “those that improve if there is a greater quantity or quality of nursing care” (Yoder-Wise, 2011, p. 399). Patient outcome goals could include a LEADERSHIP STRATEGY ANALYSIS 5 decrease in call lights, pressure ulcers or falls related to increased compliance with hourly rounding. Implementation Strategies Formal education of staff has been shown to be an important factor in implementation of hourly rounding (Rondinelli et al., 2012). This includes educational in-services, PowerPoint presentations and workshops that provide evidence of improved patient outcomes and expected hourly rounding activities. This education should focus on the areas identified on the questionnaire as the most common barriers to implementation or misconceptions regarding importance of implementation. A unit-level team that assists with decision-making and developing rounding tools has also been shown to be both a major support and facilitator of hourly rounding implementation (Rondinelli et al., 2012). This team concept would be an example of the Diffusion of Innovations Theory, where unit leaders and role models are used to influence peers to adopt the change in practice (Kaminski, 2011). Evaluation It is important that data is gathered and evaluated throughout the course of implementation to ascertain whether progress towards goals is occurring (Yoder-Wise, 2011). Because the hospital has been unsuccessful during a previous attempt at initiating hourly rounding, it is very important that evaluation occurs frequently and consistently so that this failure does not occur again. To begin, evaluators could gather logs to ascertain whether or not staff is in the room at regularly designated intervals. Once the timing of hourly rounding is sustained, then evaluators can move to assessing whether or not staff is asking specific questions such as if the patient is in pain or performing certain actions such as repositioning patients by directly questioning patients regarding what occurs during hourly rounding. Data related to LEADERSHIP STRATEGY ANALYSIS 6 patient falls, pressure ulcer occurrences and number of call lights should be obtained before the hourly rounding strategies are implemented and then monthly throughout. If this data does show improvement in these measures after implementation, it can be presented to staff to show that these factors are all indeed reduced by hourly rounding and that nurses are directly improving patient outcomes by making this change in their practice. If the data does not show improvement in these measures, further evaluation should be performed to determine why hourly rounding has not had the same positive impact on patient outcomes that has occurred at other facilities that practice hourly rounding. Conclusion In conclusion, research has shown that hourly rounding has many positive impacts on patient outcomes and satisfaction. Despite this evidence, Mercy Hospital-Cadillac has not been successful with making hourly rounding part of nursing practice at their facility. It is important that this is analyzed and strategies are developed and implemented in order to improve compliance with this activity that has been proven to increase positive outcomes for patients. As nurses we have an ethical duty to promote good for our patients, and this duty includes improving current practices for the benefit of our patients. LEADERSHIP STRATEGY ANALYSIS 7 References Claude-Gutekust, M., Donches, A., Dries, R., Kessler, B., & Snyde, M. (2012). The merry-goround of patient rounding: assure your patients get the brass ring. MedSurg Nursing, 21(4), 240. Retrieved from http://0go.galegroup.com.libcat.ferris.edu/ps/i.do?id=GALE%7CA299760273&v=2.1&u=lom_f errissu&it=r&p=AONE&sw=w Kaminski, J. (2011). Diffusion of innovation theory, Theory in nursing informatics column. Canadian Journal of Nursing Informatics, 7(2). Retrieved from http://cjni.net/journal/?p=1444 Rondinelli, J., Ecker, M., Crawford, C., Seelinger, C., & Omery, A. (2012). Hourly rounding implementation: A multisite description of structures, processes and outcomes. The Journal of Nursing Administration, 42(6), 326-332. doi: 0.1097/NNA.0b013e31824ccd43 Yoder-Wise, P. S. (2011). Leading and managing in nursing (5th ed.). St. Louis, Missouri: Elsevier Mosby.